Tesamorelin: Complete Research Guide
On this page
Quick Reference Card
Attribute
Also Known As
- Detail
- Tesamorelin acetate, GHRH(1-44) amide, TH9507, Somatoliberin (modified), Egrifta, Egrifta SV
Attribute
Administration
- Detail
- Subcutaneous injection
Attribute
Research Status
- Detail
- FDA-approved for HIV-associated lipodystrophy (November 2010). Off-label for body recomposition and metabolic optimization. WADA-prohibited.
Attribute
Typical Dose Range
- Detail
- 1-2 mg subcutaneous once daily; 2 mg is the FDA-approved dose
Attribute
Half-Life
- Detail
- 8-26 minutes in healthy subjects; approximately 38 minutes at steady state in HIV-infected patients
Attribute
Cycle Length
- Detail
- 12-16 weeks on, 2-4 weeks off (community protocols); clinical trials support up to 52 weeks of continuous use with monitoring
Attribute
Storage
- Detail
- Lyophilized: 2-8C refrigerated, protected from light; Reconstituted: 2-8C, use within 7-28 days depending on reconstitution solution
Overview / What Is Tesamorelin?
The Basics
Tesamorelin is a synthetic version of growth hormone-releasing hormone (GHRH), the natural signal your brain sends to the pituitary gland when it wants growth hormone produced. What sets it apart from most peptides in this space is a simple fact: the FDA approved it. It cleared two large Phase III clinical trials involving over 800 patients, making it the only growth hormone secretagogue with that level of clinical proof behind it.
The compound works by telling your pituitary gland to release growth hormone in the same rhythmic, pulsing pattern your body uses naturally. This is fundamentally different from injecting synthetic growth hormone directly. Think of it as turning up the volume on a signal your body already sends, rather than replacing the signal with an external one. That distinction has real consequences for safety, because your body's built-in braking system (a molecule called somatostatin) still works while tesamorelin is active. It is difficult to push growth hormone to dangerous levels with this compound because the feedback loop stays intact.
Its primary proven use is reducing visceral fat, the deep abdominal fat wrapped around your organs. In clinical trials, it reduced this specific type of fat by 15-20% over 26 weeks. This is not general weight loss. Tesamorelin preferentially targets visceral fat while leaving subcutaneous fat (the fat under your skin) largely unchanged, and it preserves lean muscle mass in the process.
One important caveat: the effects require ongoing use. Patients who stopped taking tesamorelin in clinical trials saw their visceral fat return within months.
The Science
Tesamorelin is a synthetic 44-amino-acid GHRH analog consisting of the complete human GHRH(1-44) sequence with a trans-3-hexenoic acid modification at the N-terminus [1]. This lipid modification confers resistance to dipeptidyl peptidase-IV (DPP-IV), the enzyme primarily responsible for rapid degradation of native GHRH, extending biological activity without altering the core receptor binding properties [2][3].
The compound was developed by Theratechnologies Inc. and received FDA approval in November 2010 under the brand name Egrifta for the reduction of excess visceral adipose tissue in HIV-infected patients with lipodystrophy [1][2]. An updated formulation (Egrifta SV) received approval in November 2019, offering improved room-temperature stability prior to reconstitution.
Approval was based on two Phase III randomized, double-blind, placebo-controlled trials: LIPO-010 (N=412) and CTR-1011 (N=404), using 2:1 randomization with 2 mg daily subcutaneous dosing. Both met their primary endpoint of significant visceral adipose tissue (VAT) reduction versus placebo at 26 weeks [2][4]. This evidence base is structurally distinct from other GH secretagogues: sermorelin's adult body composition data derives from a single trial of 19 subjects [5], and CJC-1295 without DAC has no published human trials [6].
Molecular Identity
Attribute
Common Names
- Detail
- Tesamorelin, Tesamorelin acetate, GHRH(1-44) amide, TH9507, Somatoliberin (modified)
Attribute
Trade Names
- Detail
- Egrifta (2010), Egrifta SV (2019)
Attribute
Amino Acid Sequence
- Detail
- Tyr-Ala-Asp-Ala-Ile-Phe-Thr-Asn-Ser-Tyr-Arg-Lys-Val-Leu-Gly-Gln-Leu-Ser-Ala-Arg-Lys-Leu-Leu-Gln-Asp-Ile-Met-Ser-Arg-Gln-Gln-Gly-Glu-Ser-Asn-Gln-Glu-Arg-Gly-Ala-Arg-Ala-Arg-Leu-NH2
Attribute
Peptide Length
- Detail
- 44 amino acids, C-terminal amidation
Attribute
N-Terminal Modification
- Detail
- trans-3-hexenoic acid moiety conjugated to Tyr1
Attribute
Molecular Formula
- Detail
- C221H366N72O67S
Attribute
Molecular Weight
- Detail
- 5135.86 Da (free base); ~5579 Da (acetate salt)
Attribute
CAS Number
- Detail
- 218949-48-5 (free base); 901758-09-6 (acetate salt)
Attribute
PubChem CID
- Detail
- 16137828
Attribute
DrugBank ID
- Detail
- DB08869
Attribute
FDA UNII
- Detail
- MQG94M5EEO
Attribute
Functional Class
- Detail
- GHRH receptor agonist; growth hormone secretagogue; pituitary hormone-stimulating peptide
Mechanism of Action
The Basics
Your pituitary gland releases growth hormone in pulses, with the largest bursts happening during deep sleep. Tesamorelin amplifies this natural process. It mimics the signal (GHRH) that your hypothalamus normally sends to trigger these pulses, but it lasts longer because of a small chemical modification that protects it from being broken down too quickly.
Here is the cascade in practical terms: Tesamorelin activates the pituitary, which releases a burst of growth hormone. That growth hormone travels to the liver and other tissues, where it triggers production of IGF-1 (insulin-like growth factor 1). IGF-1 is the molecule that does most of the downstream work, shifting your metabolism toward burning fat (especially visceral fat) while preserving muscle tissue.
The critical safety feature is what happens next. As growth hormone and IGF-1 levels rise, your hypothalamus releases more somatostatin, which puts the brakes on further growth hormone release. This negative feedback loop creates a natural ceiling that makes it very difficult to push growth hormone to dangerous levels with tesamorelin alone. This is why it has a fundamentally different risk profile compared to injecting synthetic growth hormone directly, which bypasses this brake entirely.
The reason tesamorelin preferentially targets visceral fat is not because the compound itself is "targeted." Visceral fat cells have a higher density of growth hormone receptors than subcutaneous fat cells. When growth hormone levels rise, visceral fat is simply more responsive to the signal, making it the first fat depot to be mobilized.
The Science
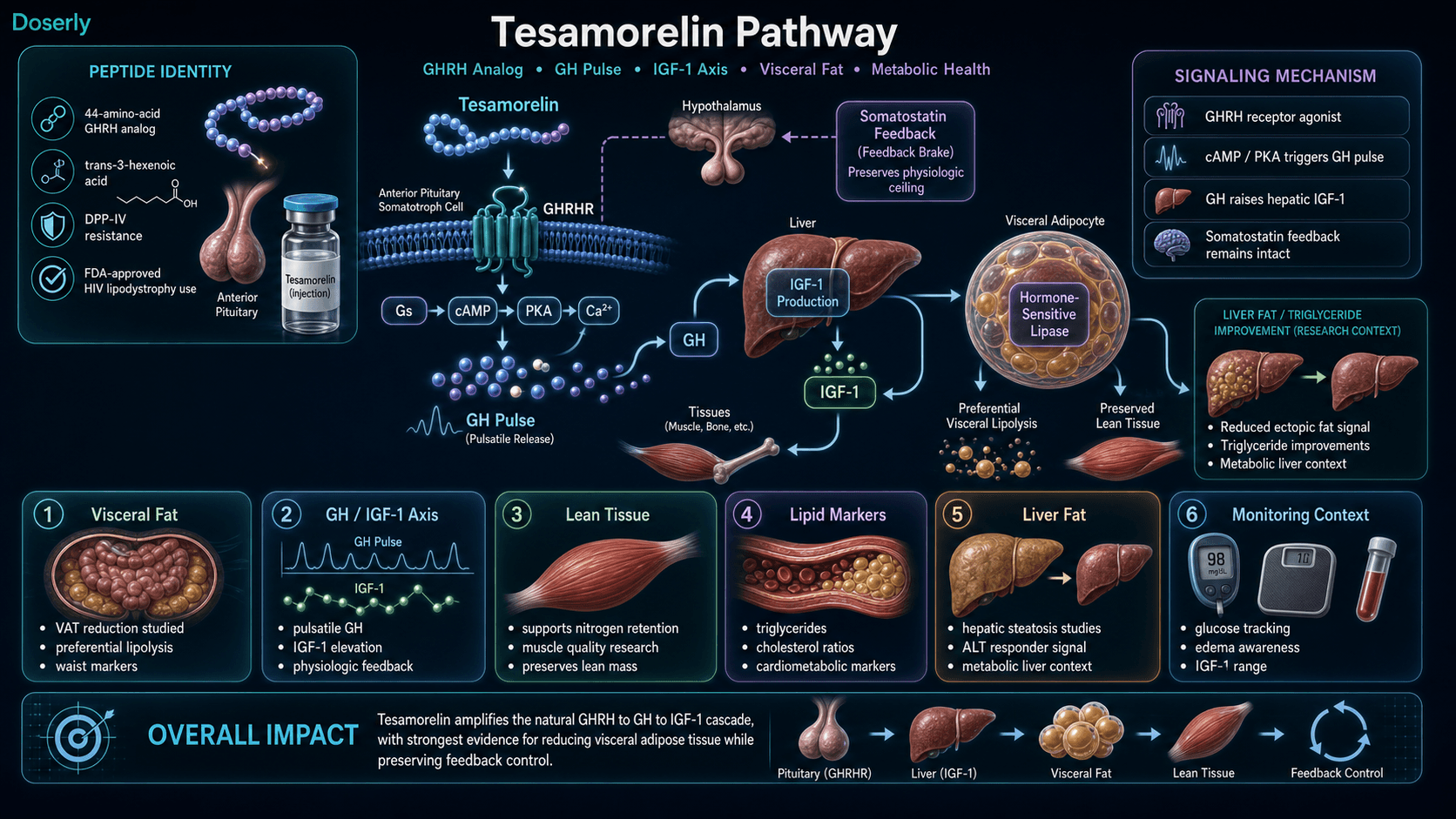
Tesamorelin acts as a selective agonist at the growth hormone-releasing hormone receptor (GHRHR), a class B (secretin-like) G-protein coupled receptor expressed on anterior pituitary somatotroph cells [2][3]. Binding activates the Gs-coupled cAMP/PKA signaling cascade, increasing intracellular cyclic adenosine monophosphate (cAMP) and downstream calcium signaling, leading to growth hormone (GH) synthesis and pulsatile release [3].
The trans-3-hexenoic acid N-terminal modification confers resistance to DPP-IV cleavage without significantly altering GHRH receptor binding affinity, which remains comparable to or slightly exceeds that of native human GHRH [2]. This structural feature is primarily responsible for the improved proteolytic stability relative to unmodified GHRH(1-44).
Downstream effects of tesamorelin-stimulated GH release include:
- IGF-1 elevation: GH-stimulated hepatic IGF-1 production increases by approximately 106-109 ng/mL at the 2 mg daily dose, mediating the majority of GH's effects on tissue metabolism [2][4].
- Preferential visceral lipolysis: Visceral adipocytes express higher densities of GH receptors than subcutaneous adipocytes, resulting in preferential mobilization of visceral fat stores through hormone-sensitive lipase activation [7].
- Somatostatin feedback preservation: Unlike exogenous GH administration, tesamorelin-stimulated GH release triggers physiologic somatostatin upregulation, maintaining the pulsatile GH secretion pattern and preventing sustained supraphysiological levels [5].
- Lean tissue preservation: GH and IGF-1 elevation enhances protein synthesis and nitrogen retention, supporting lean body mass maintenance during periods of negative energy balance [6][7].
Pathway Visualization Image
Pharmacokinetics
The Basics
Tesamorelin works quickly but does not stay in the bloodstream for long. After a subcutaneous injection, it reaches peak levels within a couple of hours and has a surprisingly short half-life, ranging from roughly 8 minutes to about 38 minutes depending on the individual and the study. That means it clears from your blood faster than most people expect.
This raises an obvious question: if it disappears so fast, how does it work? The answer is that the brief receptor activation is potent enough to trigger a full growth hormone cascade. Tesamorelin acts like a starter motor, not a sustained engine. It fires the pituitary to release growth hormone, and then the growth hormone and IGF-1 carry the metabolic effects forward for hours afterward. The short half-life actually contributes to the pulsatile pattern that makes this compound physiologically distinct from continuous growth hormone administration.
One detail that matters for practical use: the bioavailability after subcutaneous injection is less than 4%. This means the vast majority of what you inject never reaches the bloodstream. The effective dose accounts for this low absorption, which is why the clinical dose is 2 mg, a relatively large amount compared to many other peptides.
The Science
Tesamorelin demonstrates rapid absorption following subcutaneous administration, with absolute bioavailability below 4% [2]. Despite low systemic exposure, the pharmacodynamic response (GH release) is robust, indicating potent receptor activation at the pituitary level [2][3].
Pharmacokinetic parameters include:
Parameter
Bioavailability (SC)
- Value
- < 4%
Parameter
Tmax
- Value
- Within hours of injection
Parameter
Elimination half-life
- Value
- 8-26 minutes (healthy); ~38 minutes (HIV patients at steady state)
Parameter
Volume of distribution
- Value
- 4.8 +/- 1.9 L/kg
Parameter
Clearance
- Value
- ~0.58 L/kg/hour
Metabolism occurs primarily through proteolytic cleavage by serum peptidases. The N-terminal hexenoyl moiety may undergo beta-oxidation. Exact elimination pathways are not fully characterized in humans. No formal human metabolism studies have been documented [2].
The pharmacodynamic profile extends beyond plasma kinetics: GH release patterns persist through the natural nocturnal cycle when dosed before sleep, and IGF-1 elevation (the primary mediator of downstream effects) has a substantially longer half-life of approximately 12-15 hours [2][4].
Research & Clinical Evidence
Visceral Fat Reduction in HIV-Associated Lipodystrophy
The Basics
This is the area where tesamorelin has its strongest evidence, and it is worth understanding just how strong that evidence is. Two large clinical trials, each with over 400 patients, showed that tesamorelin at 2 mg daily reduced visceral fat by 12-20% over 26 weeks compared to placebo. These were gold-standard trials: randomized, double-blind, placebo-controlled, the kind of evidence the FDA requires before approving a drug.
The effects were specific to visceral fat. Subcutaneous fat (the fat you can pinch) was largely unchanged. Waist circumference decreased by 1.3 to 1.8 cm versus placebo. Triglycerides dropped by 37 mg/dL. Patients reported significant improvements in body image and self-perception.
In a 52-week extension, patients who continued on tesamorelin maintained their fat loss and even saw modest additional improvement. But here is the part that cannot be overlooked: patients who switched to placebo at the 26-week mark regained an average of 24.5% of their visceral fat by week 52. The fat comes back, and it comes back aggressively. This positions tesamorelin as a maintenance therapy, not a one-time reset.
The Science
LIPO-010 (N=412) and CTR-1011 (N=404) were both Phase III, randomized, double-blind, placebo-controlled trials using 2:1 randomization with 2 mg daily subcutaneous dosing [2][4].
Primary endpoint results at 26 weeks:
- LIPO-010: Least-squares mean VAT reduction of -19.6% versus placebo (95% CI: -23.7% to -15.3%) [4]
- CTR-1011: Least-squares mean VAT reduction of -11.7% versus placebo (95% CI: -16.2% to -7.1%) [4]
- IGF-1 increase: approximately 106-109 ng/mL in treatment groups [2][4]
- Waist circumference: -1.8 cm (LIPO-010) and -1.3 cm (CTR-1011) versus placebo [4]
- Triglyceride reduction: 37 mg/dL versus placebo [2]
Pooled analysis of both trials confirmed sustained efficacy with continuous treatment through 52 weeks, with VAT maintained at 17.5% below baseline and waist circumference reduced by 3.4 cm [2]. The discontinuation data showed a -25.8% difference between continued and discontinued groups (P=0.0008) [8].
Hepatic Steatosis and Liver Health
The Basics
Beyond visceral fat, tesamorelin has shown promise for reducing fat in the liver. In HIV patients with non-alcoholic fatty liver disease (NAFLD), tesamorelin reduced the amount of fat stored in the liver and improved markers of liver function. This is significant because fatty liver disease is a growing health concern that can progress to more serious conditions if left unaddressed.
The connection makes biological sense. Visceral fat and liver fat are metabolically linked, and reducing one tends to improve the other. One study found that patients who responded well to tesamorelin's visceral fat reduction also saw their liver enzymes (ALT) drop by 7.4 U/L, with benefits persisting through 52 weeks.
The Science
A randomized trial in HIV patients with MRI-confirmed NAFLD demonstrated that tesamorelin reduced hepatic fat fraction and improved histologic features including steatosis and fibrosis progression [7]. A study of 38 patients on integrase strand transfer inhibitor (INSTI)-based regimens showed hepatic fat decline of -4.2% versus -0.5% placebo [9]. VAT responders showed ALT reductions of 7.4 U/L persisting to 52 weeks, suggesting a mechanistic link between visceral adiposity reduction and hepatic health improvement [10].
Neurocognitive Function
The Basics
Emerging research suggests tesamorelin may have benefits beyond fat loss. A study in 73 HIV patients with both cognitive difficulties and central obesity tested whether tesamorelin could improve thinking and memory. Waist circumference decreased significantly more with tesamorelin (2.7 cm more than control), and cognitive test scores trended in a positive direction, though the study was too small to reach statistical significance.
This research is preliminary, but the potential connection between growth hormone restoration, metabolic health, and cognitive function is an active area of investigation.
The Science
In a controlled trial of 73 HIV-positive participants with neurocognitive impairment and abdominal obesity, 2 mg daily tesamorelin for 6 months produced a 2.7 cm greater waist reduction versus standard care with significant IGF-1 elevation [11]. Composite cognitive scores trended toward improvement (+0.146 vs +0.103) but did not reach statistical significance, likely due to insufficient sample size. The study provides preliminary support for the hypothesis that GH/IGF-1 axis restoration may support cognitive function in populations with metabolic-cognitive overlap.
Muscle Quality Improvement
The Basics
Clinical imaging has revealed an effect beyond fat loss: tesamorelin appears to improve the quality and density of abdominal muscles. CT scans of over 340 patients showed that core muscles became denser and firmer during treatment, independent of fat loss. This suggests the compound is not just removing fat from around the organs but is actively improving the condition of nearby muscle tissue through its growth hormone and IGF-1 effects.
The Science
CT-based analysis of 341 HIV patients demonstrated that tesamorelin improved skeletal muscle attenuation in the abdominal compartment, with rectus abdominis muscle density increasing by 4.86 Hounsfield units [12]. These improvements in muscle quality occurred independently of VAT changes and persisted after adjusting for IGF-1 elevation, suggesting direct GH-mediated effects on muscle tissue composition.
Biomarker Evidence Matrix
Only categories with sufficient data are scored. Evidence Strength reflects clinical and preclinical research quality. Reported Effectiveness reflects community-reported outcomes from the sentiment analysis.
Category
Fat Loss
- Evidence Strength
- 9/10
- Reported Effectiveness
- 9/10
- Summary
- Two Phase III RCTs (N=816) demonstrate 12-20% visceral fat reduction. Community reports overwhelmingly confirm measurable visceral fat loss with specific biometric data.
Category
Weight Management
- Evidence Strength
- 7/10
- Reported Effectiveness
- 7/10
- Summary
- Clinical trials show body composition improvement (fat loss with lean mass preservation). Community describes recomposition rather than simple weight loss.
Category
Muscle Growth
- Evidence Strength
- 6/10
- Reported Effectiveness
- 6/10
- Summary
- CT imaging shows improved muscle density and quality. Community reports lean mass preservation during deficit, some increased lifting capacity.
Category
Sleep Quality
- Evidence Strength
- 4/10
- Reported Effectiveness
- 7/10
- Summary
- One clinical trial explored GHRH/sleep architecture connection (NCT insomnia study). Community consistently reports improved sleep quality as a secondary benefit.
Category
Energy Levels
- Evidence Strength
- 3/10
- Reported Effectiveness
- 6/10
- Summary
- Limited direct clinical evidence for energy. Some community reports of improved daily energy, though confounded by concurrent lifestyle changes.
Category
Recovery & Healing
- Evidence Strength
- 5/10
- Reported Effectiveness
- 7/10
- Summary
- GH/IGF-1 pathway supports tissue repair. Community reports improved post-workout recovery and injury healing, though often while stacking other compounds.
Category
Mood & Wellbeing
- Evidence Strength
- 4/10
- Reported Effectiveness
- 6/10
- Summary
- Phase III trials documented improved body image distress scores. Community reports improved mood, likely partially mediated by body composition changes.
Category
Body Image
- Evidence Strength
- 7/10
- Reported Effectiveness
- 7/10
- Summary
- Clinical trials measured body image satisfaction as secondary endpoint with significant improvement. Strong community reports of satisfaction with physical changes.
Category
Gut Health
- Evidence Strength
- 5/10
- Reported Effectiveness
- 4/10
- Summary
- Hepatic fat reduction suggests metabolic health improvement. Limited direct gut health data. Community reports of reduced bloating are ambiguous.
Category
Joint Health
- Evidence Strength
- 3/10
- Reported Effectiveness
- 5/10
- Summary
- Arthralgia listed as common side effect. Community reports are mixed: some joint aches, others improved comfort as part of general recovery.
Category
Fluid Retention
- Evidence Strength
- N/A (side effect)
- Reported Effectiveness
- 5/10
- Summary
- Clinical trials report 5-10% edema rate. Community confirms water retention as most discussed side effect, manageable with antihistamines and dose adjustment.
Category
Side Effect Burden
- Evidence Strength
- 8/10
- Reported Effectiveness
- 6/10
- Summary
- Phase III trials document generally mild side effect profile. Community reports overall good tolerability with injection site reactions as primary concern.
Category
Physical Performance
- Evidence Strength
- 4/10
- Reported Effectiveness
- 6/10
- Summary
- IGF-1 elevation supports performance. Community reports maintaining or increasing training capacity during caloric deficit.
Category
Skin Health
- Evidence Strength
- 3/10
- Reported Effectiveness
- 4/10
- Summary
- GH/IGF-1 supports collagen synthesis theoretically. Minimal community discussion of skin-specific effects.
Category
Longevity & Neuroprotection
- Evidence Strength
- 4/10
- Reported Effectiveness
- 5/10
- Summary
- Neurocognitive study (N=73) showed trend toward improvement. Limited community discussion of longevity applications.
Category
Treatment Adherence
- Evidence Strength
- 7/10
- Reported Effectiveness
- 6/10
- Summary
- Daily injection protocol well-established. Community discusses cost barriers and injection site management as adherence challenges.
Benefits & Potential Effects
The Basics
Tesamorelin's primary benefit is targeted visceral fat reduction. This is not general weight loss; it is the specific removal of the metabolically dangerous fat wrapped around your organs. Clinical trials showed a 15-20% reduction in this type of fat over 26 weeks, with improvements in triglycerides and waist circumference. Many users describe the experience as their body changing shape rather than the number on the scale moving dramatically. Clothes fit differently, the midsection tightens, but total weight may stay relatively stable because lean tissue is preserved.
Beyond fat loss, several secondary benefits are consistently reported. Sleep quality often improves within the first couple of weeks, likely because the compound restores the natural growth hormone pulses that are strongest during deep sleep. Recovery from exercise tends to become more predictable. Some users notice improved mood and energy, though these effects are harder to separate from the psychological benefits of visible body changes.
For users combining tesamorelin with GLP-1 agonists (such as tirzepatide or semaglutide), the compound serves a specific protective role: it preserves lean muscle mass during the aggressive fat loss that GLP-1 drugs produce. Research suggests that 25-40% of weight lost on GLP-1 agents alone can be lean tissue. Tesamorelin's growth hormone support helps shift that balance toward fat-only loss.
The Science
The documented benefits of tesamorelin span several physiological domains, all mechanistically linked through the GH/IGF-1 axis:
- Visceral adipose tissue reduction: 12-20% VAT decrease over 26 weeks in Phase III trials, mediated by preferential lipolysis in visceral adipocytes through upregulated hormone-sensitive lipase activity [2][4][7].
- Lipid profile improvement: Triglyceride reduction of 37-51 mg/dL, improved cholesterol-to-HDL ratios, and overall cardiometabolic marker improvement sustained through 52 weeks [2][4].
- Hepatic fat reduction: Up to 37% reduction in hepatic steatosis in NAFLD populations, with ALT improvement of 7.4 U/L in VAT responders [7][9][10].
- Lean body mass preservation: Maintained or increased lean tissue mass during treatment periods, with improved skeletal muscle attenuation on CT imaging [12].
- Body image improvement: Statistically significant improvements in trunk and belly appearance distress scores as secondary endpoints in Phase III trials [2].
- Potential neurocognitive benefit: Trending improvement in composite cognitive scores in HIV patients with neurocognitive impairment, potentially mediated by IGF-1's neuroprotective effects [11].
Side Effects & Safety Considerations
The Basics
Tesamorelin's side effect profile is generally mild, and this is well-established through large clinical trials rather than just community reports. The most common issues, in order of frequency, are injection site reactions, fluid retention, and muscle or joint aches.
Injection site reactions deserve special attention because they follow an unusual pattern. Most users experience no issues for the first few weeks. Then, around weeks 4-8, itchy raised welts (similar to mosquito bites) start appearing at injection sites. This is not an allergic reaction; it is a histamine response caused by the peptide activating mast cells in the subcutaneous tissue. The skin is sensitizing to repeated exposure, not reacting to a single injection. Mitigation strategies include taking an antihistamine before injection, using deeper injection technique, rotating to less reactive sites (love handles are often best tolerated), diluting the reconstituted solution, and injecting more slowly.
Fluid retention can manifest as puffy fingers, mild ankle swelling, or tingling in the hands similar to carpal tunnel syndrome. This is a class effect shared by anything that raises growth hormone levels. It is dose-dependent and typically resolves with dose reduction.
The most important monitoring concern is blood sugar. Growth hormone is inherently diabetogenic, meaning it promotes insulin resistance as part of its normal metabolic function. For most people this does not reach clinically significant levels, but for anyone with pre-existing insulin resistance, prediabetes, or type 2 diabetes, glucose monitoring during use is essential.
The Science
Phase III trial adverse event data (tesamorelin 2 mg vs. placebo):
Adverse Event
Injection site reactions
- Tesamorelin
- 30-51%
- Placebo
- 21-24%
Adverse Event
Myalgia/muscle pain
- Tesamorelin
- 4-8%
- Placebo
- 2%
Adverse Event
Fluid retention/edema
- Tesamorelin
- 5-10%
- Placebo
- 1-6%
Adverse Event
Serious adverse events
- Tesamorelin
- Similar rates
- Placebo
- Similar rates
Injection site reactions are histamine-mediated, involving mast cell activation in subcutaneous tissue with progressive sensitization over 4-8 weeks of use [8]. The mechanism is distinct from pH-related injection pain seen with compounds like NAD+.
Glucose metabolism: The FDA flagged higher glucose intolerance risk across the overall development program, though individual pivotal trials did not show statistically significant glycemic deterioration [1][4]. A dedicated safety trial in type 2 diabetic patients (Clemmons et al.) showed no major worsening of HbA1c or fasting glucose [13]. Monitoring recommendations: fasting glucose and HbA1c at baseline and regular intervals.
IGF-1 elevation: Approximately 106-109 ng/mL increase across trials [2][4]. No malignancy signal during trial windows (up to 52 weeks). Active malignancy is a contraindication due to IGF-1's role in cell proliferation. Monitoring target: high-normal physiologic range, not supraphysiologic (>350-400 ng/mL warrants dose reduction) [8].
Contraindications: Active malignancy, pregnancy (Category X), known hypersensitivity to tesamorelin or mannitol [1][2].
No signal for increased cardiovascular events, hepatotoxicity, or hypothalamic-pituitary-testicular axis (HPTA) suppression in trial data [2][4].
Side effect profiles are most useful when you can compare them against your own experience in real time. Doserly lets you log symptoms, severity, and timing alongside your dosing data, creating a side-by-side view of your protocol and your body's response.
This kind of systematic tracking catches things that memory alone misses. A subtle mood shift that began three days after a dose increase. Sleep disruption that correlates with evening administration. These patterns become visible when the data is laid out on a timeline, and they give your healthcare provider actionable information rather than vague concerns. Early detection of emerging side effects means earlier intervention.
Capture changes while they are still fresh.
Log symptoms, energy, sleep, mood, and other observations alongside protocol events so patterns do not live only in memory.
Trend view
Symptom timeline

Symptom tracking is informational and should be interpreted with a qualified clinician.
Dosing Protocols
The Basics
Tesamorelin dosing is more standardized than most peptides because it has an FDA-approved protocol to anchor the discussion. The clinical dose is 2 mg injected subcutaneously once daily, typically in the evening before bed. Most sources suggest starting at 1 mg for the first 1-2 weeks to assess tolerability before increasing to the full 2 mg.
Timing matters for this compound. Administering before bed aligns the drug's effects with the body's natural nocturnal growth hormone secretion pattern, when the largest GH pulses normally occur. Fasting for at least 2 hours before injection is also consistently recommended, because food intake (particularly carbohydrates and fats) can blunt the growth hormone response.
Cycle length in community protocols typically runs 12-16 weeks on, followed by 2-4 weeks off. Clinical trials, however, ran continuously for up to 52 weeks with sustained benefits. The cycling approach is primarily a community convention aimed at preserving pituitary sensitivity and managing IGF-1 levels, though evidence for pituitary desensitization with tesamorelin specifically is limited.
Some users adopt a 5-days-on, 2-days-off schedule primarily for cost management rather than any pharmacological rationale. The clinical data supporting efficacy is based on daily dosing.
The Science
The FDA-approved dose is 2 mg subcutaneous once daily for the treatment of HIV-associated lipodystrophy [1][2].
Protocol Element
Standard dose
- Clinical/FDA
- 2 mg daily
- Community Consensus
- 1-2 mg daily
Protocol Element
Starting dose
- Clinical/FDA
- 2 mg (no titration in trials)
- Community Consensus
- 1 mg for 1-2 weeks, then 2 mg
Protocol Element
Frequency
- Clinical/FDA
- Daily
- Community Consensus
- Daily; some use 5 on/2 off
Protocol Element
Timing
- Clinical/FDA
- Not specified in label
- Community Consensus
- 30-60 min before bed, 2+ hours fasted
Protocol Element
Cycle length
- Clinical/FDA
- Up to 52 weeks continuous
- Community Consensus
- 12-16 weeks on, 2-4 weeks off
Protocol Element
Route
- Clinical/FDA
- Subcutaneous (abdominal)
- Community Consensus
- Subcutaneous (abdomen, thigh, love handles)
IGF-1 monitoring protocol (from clinical guidance):
- Baseline IGF-1 before initiation
- Repeat at 4-6 weeks to assess response
- If acceptable, recheck at 3 months
- Ongoing monitoring every 2-3 months
- Target: above mid-range of normal reference range, up to upper limit of normal
- If IGF-1 exceeds 350-400 ng/mL, reduce dose or switch to every-other-day administration [8]
Safety monitoring:
- Baseline: CBC, CMP, HbA1c, lipid panel, IGF-1
- Week 4-6: IGF-1 recheck
- Ongoing: IGF-1 every 2-3 months, periodic glucose assessment
Consistency is the difference between a protocol that delivers results and one that wastes time and money. Doserly was built for exactly this: keeping you on track with the precision your protocol demands.
The built-in calculators handle the math you shouldn't be doing in your head. The reconstitution calculator tells you exactly how much bacteriostatic water to add for your target concentration. The dose calculator converts between units, milligrams, and syringe markings so you draw the right amount every time. The injection site heat map tracks where you've administered and when, helping you rotate sites systematically to reduce tissue damage, scarring, and absorption inconsistencies from overusing the same area. Pair that with smart reminders tuned to your protocol's timing requirements, and you build the kind of daily consistency that separates optimized protocols from haphazard ones.
Turn symptom and safety notes into a clearer timeline.
Doserly helps you log doses, symptoms, and safety observations side by side so patterns are easier to discuss with a qualified clinician.
Pattern view
Logs and observations

Pattern visibility is informational and should be reviewed with a clinician.
What to Expect
This timeline reflects patterns from clinical trial data and community reports. Individual responses vary significantly based on dose, baseline body composition, concurrent compounds, training, and diet.
Weeks 1-2:
Most users notice very little in terms of body composition at this stage. What may change first is sleep quality, with deeper sleep and more vivid dreams reported by many users within the first week or two. Energy levels may feel subtly improved upon waking. Injection site reactions are typically absent during this initial period.
Weeks 3-4:
Growth hormone and IGF-1 levels are reaching steady state. Some users begin noticing subtle changes in how their midsection feels (less "internal bloating"). Recovery from exercise may start feeling more predictable. Injection site reactions may begin appearing as the histamine sensitization process starts.
Weeks 4-6:
This is when measurable body composition changes typically become detectable. Users stacking with GLP-1 agonists often notice renewed progress after previously plateauing. Waist measurements may begin trending downward. Injection site welts become more consistent; mitigation strategies (antihistamines, site rotation) become relevant.
Weeks 6-8:
Clinical trial data shows this is the window where visceral fat reduction becomes statistically significant on imaging. Community users often describe clothes fitting noticeably differently, particularly around the midsection. This is the recommended point for the first IGF-1 blood test to guide dose adjustment.
Weeks 8-12:
Continued progressive improvement. Users who have been consistent with dosing, timing, diet, and training report the most dramatic changes during this window. DEXA and biometric scale data often show meaningful shifts in body composition metrics.
Weeks 12-26:
The Phase III trial endpoint window. Visceral fat reduction of 12-20% versus placebo is the documented clinical outcome. Continued improvements in triglycerides, waist circumference, and body composition. Injection site reactions typically stabilize into a predictable pattern.
After discontinuation:
Based on clinical trial extension data, visceral fat begins returning. Patients who stopped at 26 weeks regained approximately 24.5% of lost visceral fat by week 52. This is an important expectation to set: the effects require ongoing use to maintain.
The week-by-week expectations above are drawn from research and community reports, but your experience will be uniquely yours. Doserly's biomarker tracking transforms those general timelines into personal data points you can actually see and measure.
Log the specific markers relevant to this compound, whether that's pain levels, energy, sleep quality, body composition, recovery time, or mood, and watch your own trend lines emerge over weeks and months. Did your key markers start shifting in week three, like the research suggests? Is your experience tracking with what the community reports, or diverging? Over time, this creates something more valuable than any guide: an evidence-based picture of how your body responds to this specific compound, at your specific dose, within your specific health context.
Build reminders around the routine, not just the compound.
Doserly can keep timing, skipped doses, and schedule changes organized so the plan you read about becomes easier to follow and review.
Today view
Upcoming reminders
Reminder tracking supports consistency; it does not select a protocol for you.
Interaction Compatibility
Good With (Synergistic)
- Ipamorelin — Selective GH secretagogue that works through the ghrelin receptor (GHSR), complementing tesamorelin's GHRH receptor activation. The combination amplifies and extends GH pulses without increasing cortisol or prolactin. Commonly dosed at 200-500 mcg alongside tesamorelin.
- Semaglutide / Tirzepatide / Retatrutide — GLP-1 agonists create caloric deficit through appetite suppression; tesamorelin provides anabolic protection to preserve lean mass during fat loss. Different axes, complementary timing (GLP-1 during day, tesamorelin at night).
- CJC-1295 — Another GHRH analog; provides sustained background GH stimulus while tesamorelin triggers acute pulses. Some practitioners use CJC-1295 (no DAC) as an alternative or rotational compound.
- AOD-9604 — GH fragment peptide that targets lipolysis without IGF-1 elevation. Can complement tesamorelin for additional visceral fat targeting without compounding IGF-1 concerns.
- BPC-157 + TB-500 — Foundational repair peptides. Tesamorelin's GH/IGF-1 support enhances the recovery environment these compounds work within.
- MOTS-C — Mitochondrial peptide that activates AMPK and enhances fat oxidation. Works synergistically in metabolic recomposition stacks.
- NAD+ — Cofactor for cellular energy metabolism. Supports the metabolic environment for fat oxidation. Note: do not mix in the same syringe (pH incompatibility).
- DSIP — Sleep peptide that deepens slow-wave sleep, complementing tesamorelin's nocturnal GH enhancement.
- Epithalon — Anti-aging peptide; some protocols combine with tesamorelin for longevity applications.
- GHK-Cu / KPV — Recovery and tissue repair peptides often included in comprehensive protocols.
Not Good With (Caution)
- Exogenous HGH — Using tesamorelin alongside synthetic growth hormone is redundant and counterproductive. HGH bypasses the pituitary feedback system that tesamorelin relies on, and combining them risks supraphysiological GH/IGF-1 levels.
- MK-677 (Ibutamoren) — Oral GH secretagogue. Combining multiple GH-axis stimulators increases risk of sustained IGF-1 elevation beyond safe ranges. If combining, aggressive IGF-1 monitoring is essential.
- Insulin (exogenous) — GH and insulin have opposing metabolic effects. Tesamorelin's diabetogenic potential combined with exogenous insulin requires careful medical management.
- Any compound in the context of active malignancy — IGF-1 elevation is contraindicated with cancer or high neoplasm risk.
Administration Guide
Materials required:
- U-100 insulin syringes (1 mL, 29-31G needle, 5/16 to 1/2 inch)
- Alcohol swabs (70% isopropyl)
- Sharps container
- Bacteriostatic water (with sodium chloride/isotonic formulation preferred to reduce injection site sting)
- Gauze pads
Recommended reconstitution solution:
Bacteriostatic water is the standard reconstitution solution. Using isotonic bacteriostatic water (with sodium chloride) is specifically recommended for tesamorelin to reduce injection site reactions and prevent welts. Inject water slowly down the vial wall and swirl gently; do not shake, as this can denature the peptide.
Timing considerations:
- Administer 30-60 minutes before bed to align with the body's natural nocturnal growth hormone release window
- Maintain at least a 2-hour fast before injection (carbohydrates and fats blunt the GH response)
- If morning administration is more practical, inject fasted before exercise
- Consistency in timing matters more than the specific time chosen
Post-administration care:
- Do not massage the injection site (disrupts absorption)
- Mild redness or warmth at the injection site is normal and typically resolves within 1-2 hours
- Monitor for progressive injection site reactions starting around weeks 4-8
- If welts or itching develop, consider pre-dosing with an antihistamine (cetirizine 10 mg) 30-60 minutes before injection
- Report any spreading welts, hives on other body areas, facial swelling, or breathing difficulty to a healthcare provider immediately
Supplies & Planning
Available vial sizes:
- 5 mg vials (most common for initial trials)
- 10 mg vials
- 20 mg vials (most cost-effective for extended protocols)
- Branded Egrifta SV: supplied as pre-dosed vials with specific diluent
Reconstitution volumes by vial size:
Vial Size
5 mg
- Recommended BAC Water
- 2.5 mL
- Concentration
- 2.0 mg/mL
Vial Size
10 mg
- Recommended BAC Water
- 3.0 mL
- Concentration
- ~3.33 mg/mL
Vial Size
20 mg
- Recommended BAC Water
- 3.0 mL
- Concentration
- ~6.67 mg/mL
General materials for a protocol:
- Peptide vials (quantity depends on dose, cycle length, and vial size; consult your healthcare provider and the reconstitution calculator)
- Insulin syringes: 1 per day (7 per week for daily protocol)
- Bacteriostatic water (isotonic preferred)
- Alcohol swabs
- Sharps container
Readers should consult their healthcare provider for specific dosing and use the reconstitution calculator to determine exact volumes for their protocol.
Storage & Handling
Lyophilized (powder) form:
- Store at 2-8C (36-46F) refrigerated
- Protect from light
- Egrifta SV formulation is stable at room temperature (20-25C / 68-77F) prior to reconstitution
- Long-term storage: -20C or below extends shelf life
Reconstituted (liquid) form:
- Refrigerate immediately at 2-8C (36-46F)
- Use within 7 days when reconstituted with bacteriostatic water (conservative recommendation)
- Some sources report up to 28 days of stability with bacteriostatic water, consistent with standard peptide handling guidelines
- Use immediately if reconstituted with sterile water (no preservative); discard unused portion
- Do not freeze reconstituted solutions
- Protect from light (wrap vials in foil or store in opaque containers)
Handling best practices:
- Allow vials to reach room temperature (10-30 minutes) before reconstitution to prevent condensation
- Swab stopper with alcohol before each draw
- Use sterile needles/syringes for every draw
- Check reconstituted solution for clarity before each use; it should be colorless and clear. Discard if cloudy, discolored, or containing particles
- Label vials with reconstitution date
Lifestyle Factors
Tesamorelin's effects are significantly influenced by concurrent lifestyle practices. The compound works within your existing metabolic framework, so the quality of that framework matters.
Diet: A nutrient-dense, protein-forward diet supports the anabolic effects of elevated GH and IGF-1. Most practitioners recommend 1.6-2.2 g of protein per kilogram of body weight. A slight caloric deficit enhances visceral fat mobilization if fat loss is the primary goal. Avoid large meals, particularly high-carbohydrate or high-fat meals, within 2 hours of injection, as food intake can blunt the GH response.
Exercise: Both cardiovascular activity and resistance training complement tesamorelin's mechanism. Resistance training provides the mechanical stimulus for muscle preservation and growth, which the elevated GH/IGF-1 environment supports. Cardiovascular exercise enhances fat oxidation. Training 3-4 days per week is commonly recommended alongside tesamorelin protocols.
Sleep: This is arguably the most important lifestyle factor for tesamorelin specifically. The compound is designed to amplify nocturnal GH pulses, so the quality of your sleep directly determines how much benefit you extract. Aim for 7-9 hours of quality sleep in a cool, dark environment. Sleep hygiene practices (consistent bedtime, limited screen exposure, avoidance of stimulants in the evening) become genuinely more important when using this compound.
Monitoring: Periodic blood glucose monitoring is advisable, as sustained GH elevation can occasionally impact insulin sensitivity. Fasting glucose and HbA1c at baseline and regular intervals during use provide an early warning system for metabolic changes.
Regulatory Status & Research Classification
United States (FDA):
Tesamorelin (brand name Egrifta) received FDA approval in November 2010 for the reduction of excess abdominal fat in HIV-infected patients with lipodystrophy. An updated formulation (Egrifta SV) was approved in November 2019. This makes tesamorelin the only GH secretagogue with current FDA approval for a therapeutic (non-diagnostic) indication. Off-label use for body recomposition and metabolic optimization is common but not covered by the approval.
Canada (Health Canada):
Tesamorelin (Egrifta) has been reviewed by CADTH (Canadian Agency for Drugs and Technologies in Health) for the same indication. Available with prescription.
European Union (EMA):
Not approved by the European Medicines Agency as of the date of this guide.
WADA Status:
Tesamorelin is prohibited in competitive sport under the World Anti-Doping Agency's banned substance list, classified under Growth Hormone Releasing Factors. Athletes subject to drug testing should be aware that any GH secretagogue use constitutes an anti-doping violation.
Active Clinical Trials:
- NCT03150511: Tesamorelin to Improve Functional Outcomes After Peripheral Nerve Injury
- Multiple completed trials in HIV-associated lipodystrophy, NAFLD, and neurocognitive impairment
Access channels:
- Branded (Egrifta/Egrifta SV): By prescription, typically through endocrinologists or HIV specialists
- Compounding pharmacies: Available at lower cost; the FDA-approved status provides a legal framework for compounding
- Peptide-focused clinicians and functional medicine practitioners: Most common prescribers for off-label use
Regulatory status changes frequently. Always verify the current legal status of any compound in your specific country or jurisdiction before making any decisions.
FAQ
What is tesamorelin and what does it do?
Tesamorelin is a synthetic analog of growth hormone-releasing hormone (GHRH) that stimulates the pituitary gland to release growth hormone in natural pulses. It is FDA-approved for reducing excess visceral abdominal fat in HIV-infected patients with lipodystrophy and is commonly used off-label for body recomposition. Based on Phase III clinical trial data, it reduces visceral fat by 12-20% over 26 weeks.
How is tesamorelin different from growth hormone (HGH)?
Tesamorelin stimulates your own pituitary to release growth hormone in the pulsatile pattern your body uses naturally. HGH replaces your production with synthetic hormone delivered in a continuous, non-pulsatile manner. This distinction means tesamorelin preserves the somatostatin negative feedback system that prevents GH levels from reaching dangerous levels, giving it a different risk profile compared to exogenous HGH.
How long does it take to see results?
Based on available data, sleep quality improvements are commonly reported within 1-2 weeks. Measurable body composition changes typically become detectable by weeks 4-6. The Phase III trial primary endpoint was assessed at 26 weeks, where 12-20% visceral fat reduction was documented. Community reports suggest most users see meaningful results in the 8-12 week range with consistent use.
Does the fat come back when you stop?
Based on the Phase III extension data, yes. Patients who discontinued at 26 weeks regained an average of 24.5% of their lost visceral fat by week 52. This positions tesamorelin as an ongoing intervention rather than a one-time course of treatment. Individuals considering use should factor in the need for sustained administration to maintain results.
Can tesamorelin be combined with GLP-1 agonists like semaglutide or tirzepatide?
Based on available data, tesamorelin and GLP-1 agonists work through different mechanisms and are commonly combined. GLP-1 agonists drive appetite suppression and fat loss, while tesamorelin provides growth hormone support to preserve lean muscle mass during the deficit. The timing logic supports them: GLP-1 effects are active during waking hours, while tesamorelin-driven GH pulses are strongest during sleep.
What blood tests should be monitored?
At minimum, practitioners commonly recommend IGF-1 at baseline and at week 8 (the critical decision point for dose adjustment). Fasting glucose, HbA1c, and a lipid panel at baseline are also standard. For individuals at risk for diabetes, more frequent glucose monitoring is advisable. IGF-1 monitoring is considered essential rather than optional; the target is the high-normal physiologic range.
Does tesamorelin need to be cycled?
This is a point of disagreement across sources. Community protocols typically recommend 12-16 weeks on, 2-4 weeks off. However, clinical trial data demonstrates sustained efficacy with daily dosing for up to 52 weeks. Some clinical sources state there is no receptor desensitization or efficacy drop-off with continuous use. Individuals should discuss cycling decisions with their healthcare provider, considering IGF-1 levels and individual response.
What time of day should it be taken?
Most sources recommend 30-60 minutes before bed, on an empty stomach (at least 2 hours after eating). This timing aligns with the body's natural nocturnal growth hormone secretion pattern, when the largest GH pulses occur during deep sleep. If evening administration is not practical, fasted morning dosing before exercise is a common alternative.
What are the most common side effects?
The most frequently reported effects in clinical trials include injection site reactions (30-51%), fluid retention/edema (5-10%), and muscle aches (4-8%). Injection site reactions follow a progressive sensitization pattern, often appearing around weeks 4-8. Community mitigation strategies include antihistamines before injection, deeper injection technique, and site rotation. Serious adverse events were uncommon in trial data.
Sources & References
Phase III Clinical Trials:
[1] Falutz J, Allas S, Blot K, et al. "Metabolic effects of a growth hormone-releasing factor in patients with HIV." New England Journal of Medicine. 2007;357(23):2359-2370. https://pubmed.ncbi.nlm.nih.gov/18057338/
[2] Falutz J, Potvin D, Mamputu JC, et al. "Effects of tesamorelin (TH9507), a growth hormone-releasing factor analog, in human immunodeficiency virus-infected patients with excess abdominal fat: a pooled analysis of two multicenter, double-blind placebo-controlled phase 3 trials with safety extension data." Journal of Clinical Endocrinology & Metabolism. 2010;95(9):4291-4304. https://pubmed.ncbi.nlm.nih.gov/20554713/
Reviews and Regulatory Documents:
[3] Bedimo R. "Growth hormone and tesamorelin in HIV-associated lipodystrophy." HIV/AIDS - Research and Palliative Care. 2011;3:69-79. https://pubmed.ncbi.nlm.nih.gov/21657002/
[4] CADTH Clinical Review Report: Tesamorelin (Egrifta). Ottawa: Canadian Agency for Drugs and Technologies in Health; 2016.
[5] Walker RF. "Sermorelin: A better approach to management of adult-onset growth hormone insufficiency?" Clinical Interventions in Aging. 2006;1(4):307-308.
[6] Sinha DK, Balasubramanian A, Tatem AJ, et al. "Beyond the androgen receptor: the role of growth hormone secretagogues in the modern management of body composition in hypogonadal males." Translational Andrology and Urology. 2020;9(Suppl 2):S149-S159.
Liver and Metabolic Studies:
[7] Stanley TL, Feldpausch MN, Oh J, et al. "Effect of tesamorelin on visceral fat and liver fat in HIV-infected patients with abdominal fat accumulation: a randomized clinical trial." Lancet HIV. 2019.
[8] Falutz J, Mamputu JC, Potvin D, et al. "Long-term safety and effects of tesamorelin, a growth hormone-releasing factor analogue, in HIV patients with abdominal fat accumulation." AIDS. 2008. https://pubmed.ncbi.nlm.nih.gov/18690162/
[9] Stanley TL, et al. "Efficacy and safety of tesamorelin in people with HIV on integrase inhibitor-based regimens." 2024. https://pubmed.ncbi.nlm.nih.gov/38905488/
[10] Stanley TL, et al. "Visceral fat reduction with tesamorelin is associated with improved liver enzymes in HIV." 2017. https://pubmed.ncbi.nlm.nih.gov/28832410/
Neurocognitive Research:
[11] Effects of Tesamorelin on Neurocognitive Impairment in Persons With HIV and Abdominal Obesity. 2024. https://pubmed.ncbi.nlm.nih.gov/39813152/
Muscle Quality:
[12] Tesamorelin improves fat quality independent of changes in visceral adiposity. Obesity. 2019. https://pmc.ncbi.nlm.nih.gov/articles/PMC6766405/
Safety Studies:
[13] Clemmons DR, et al. "Safety and metabolic effects of tesamorelin in patients with type 2 diabetes: A randomized, placebo-controlled trial." PLOS One. 2017.
Clinical Trials Registry:
[14] Tesamorelin to Improve Functional Outcomes After Peripheral Nerve Injury. ClinicalTrials.gov Identifier: NCT03150511. https://clinicaltrials.gov/study/NCT03150511
Related Peptide Guides
- Ipamorelin — Selective GH secretagogue commonly paired with tesamorelin
- CJC-1295 — GHRH analog with longer half-life
- Sermorelin — Pioneer GHRH analog with distinct regulatory history
- GHRP-2 — Growth hormone-releasing peptide with broader receptor profile
- GHRP-6 — Growth hormone-releasing peptide with appetite-stimulating effects
- Hexarelin — Potent GH secretagogue
- MK-677 — Oral GH secretagogue (ibutamoren)
- Semaglutide — GLP-1 agonist commonly combined with tesamorelin
- Tirzepatide — Dual GLP-1/GIP agonist for metabolic health
- Retatrutide — Triple-agonist investigational GLP-1 compound
- AOD-9604 — GH fragment peptide for lipolysis
- MOTS-C — Mitochondrial peptide for metabolic support
- BPC-157 — Healing peptide often used in recovery stacks
- TB-500 — Tissue repair peptide
- GHK-Cu — Copper peptide for tissue repair
- DSIP — Sleep peptide complementary to nocturnal GH protocols
- IGF-1 LR3 — Extended IGF-1 analog
- PEG-MGF — Mechano growth factor for muscle repair
- NAD+ — Cellular energy cofactor (do not mix in same syringe)
- Follistatin-344 — Myostatin inhibitor for muscle growth
Need the reconstitution math for Tesamorelin: Complete Research Guide?
Open the calculator with Tesamorelin: Complete Research Guide prefilled to estimate concentration, draw volume, and related measurement math from the reconstitution details you already have.