Ipamorelin: Complete Research Guide
On this page
Quick Reference Card
Attribute
Also Known As
- Detail
- IpaMorelin, NNC 26-0161, NNC-26-0161, Aib-His-D-2-Nal-D-Phe-Lys-NH₂
Attribute
Administration
- Detail
- Injectable (subcutaneous)
Attribute
Research Status
- Detail
- Research Compound. Not FDA-approved for any therapeutic indication. WADA prohibited (Section S2). Investigated in Phase II clinical trials for postoperative ileus.
Attribute
Typical Dose Range
- Detail
- 100-300 mcg per injection, 1-3 times daily (subcutaneous)
Attribute
Half-Life
- Detail
- Approximately 2 hours (plasma elimination)
Attribute
Cycle Length
- Detail
- 8-12 weeks on, 2-4 weeks off
Attribute
Storage
- Detail
- Lyophilized: 2-8°C (short-term) or -20°C (long-term); Reconstituted: 2-8°C, use within 4 weeks
Overview / What Is Ipamorelin?
The Basics
Ipamorelin is a synthetic peptide that stimulates your body's own production of growth hormone. Rather than introducing external growth hormone directly, it works by sending a signal to your pituitary gland (a small gland at the base of your brain) to release growth hormone in natural pulses, much like it already does during deep sleep.
What makes ipamorelin stand out from other peptides in its class is selectivity. Older growth hormone peptides like GHRP-6 are effective at triggering GH release, but they also stimulate cortisol (the stress hormone), prolactin, and appetite as unwanted side effects. Ipamorelin essentially skips those off-target effects. It targets the growth hormone pathway with unusual precision, which is why it has earned a reputation as the "cleanest" growth hormone secretagogue available.
People are interested in ipamorelin for a range of reasons: supporting recovery from exercise or injury, improving sleep quality, maintaining lean muscle mass, supporting fat metabolism, and general anti-aging support. It is often combined with GHRH-type peptides like CJC-1295 (no DAC) for enhanced effects, as the two compounds work through complementary pathways. However, ipamorelin remains an investigational compound without FDA approval, and most of the human clinical data comes from early-phase trials and pharmacokinetic studies rather than large-scale efficacy trials.
The Science
Ipamorelin (NNC 26-0161) is a third-generation synthetic pentapeptide growth hormone secretagogue with the amino acid sequence Aib-His-D-2-Nal-D-Phe-Lys-NH₂. It was first characterized in 1998 by Raun and colleagues, who demonstrated that it was the first growth hormone secretagogue to exhibit truly selective GH release without concurrent elevation of ACTH, cortisol, or prolactin [1].
Ipamorelin functions as a potent and selective agonist of the growth hormone secretagogue receptor type 1a (GHS-R1a), also known as the ghrelin receptor, which is predominantly expressed on somatotroph cells of the anterior pituitary gland. Its EC50 for GH release is approximately 1-2 nM, placing it among the most potent GHS-R1a agonists studied [1]. Unlike GHRP-6 and GHRP-2, which exhibit broader receptor activation patterns and stimulate cortisol release at GH-effective doses, ipamorelin maintains its selectivity profile even at doses exceeding 200-fold the GH-effective threshold [1].
Beyond its pituitary effects, ipamorelin has demonstrated pro-motility activity in the gastrointestinal tract via GHSR-1a receptors expressed in the gut, leading to its investigation as a potential therapeutic for postoperative ileus (POI) in Phase II clinical trials [2][3]. The compound also activates insulin secretion pathways in pancreatic islet cells through indirect calcium channel stimulation [4].
Molecular Identity
Attribute
Common Names
- Detail
- Ipamorelin, IpaMorelin, NNC 26-0161, NNC-26-0161
Attribute
Amino Acid Sequence
- Detail
- Aib-His-D-2-Nal-D-Phe-Lys-NH₂
Attribute
Sequence Length
- Detail
- 5 amino acids (pentapeptide)
Attribute
Molecular Formula
- Detail
- C₃₈H₄₉N₉O₅
Attribute
Molecular Weight
- Detail
- 711.85 Da
Attribute
CAS Number
- Detail
- 170851-70-4
Attribute
PubChem CID
- Detail
- 9831659
Attribute
Structure Type
- Detail
- Linear peptide with C-terminal amidation
Attribute
D-Amino Acid Content
- Detail
- D-2-Naphthylalanine (position 3), D-Phenylalanine (position 4)
Attribute
Key Modifications
- Detail
- 2-Aminoisobutyric acid (Aib) at N-terminus for conformational constraint; D-amino acids at positions 3 and 4 enhance metabolic stability against peptidase degradation
Attribute
Functional Class
- Detail
- Ghrelin receptor agonist (GHS-R1a), growth hormone secretagogue
Attribute
Origin
- Detail
- Synthetic; derived from GHRP-1 through structural optimization
Attribute
Salt Forms
- Detail
- Free peptide or acetate salt; supplied as lyophilized powder
Mechanism of Action
The Basics
Your body releases growth hormone in pulses throughout the day, with the largest pulses happening during deep sleep. This release is controlled by two main signals: one that says "release GH now" (growth hormone releasing hormone, or GHRH) and one that says "stop releasing" (somatostatin). Ipamorelin works through a third pathway, the ghrelin receptor pathway, which acts as an independent trigger for GH release.
Think of it like a concert venue with two doors. GHRH opens one door to let growth hormone out. Ipamorelin opens a completely separate door. When both doors are open at the same time (which is why people combine ipamorelin with GHRH-type peptides), you get a much larger pulse of growth hormone than either compound could produce alone.
The key difference between ipamorelin and older peptides like GHRP-6 is precision. GHRP-6 opens the GH door but also accidentally opens doors for cortisol and prolactin. Ipamorelin opens only the GH door. This selectivity means you get the growth hormone benefits without the hormonal side effects that make older peptides more difficult to use.
Once growth hormone is released, it travels to the liver and other tissues where it stimulates the production of IGF-1 (insulin-like growth factor 1), which drives many of the downstream effects people associate with GH therapy: fat metabolism, muscle protein synthesis, tissue repair, and bone remodeling.
The Science
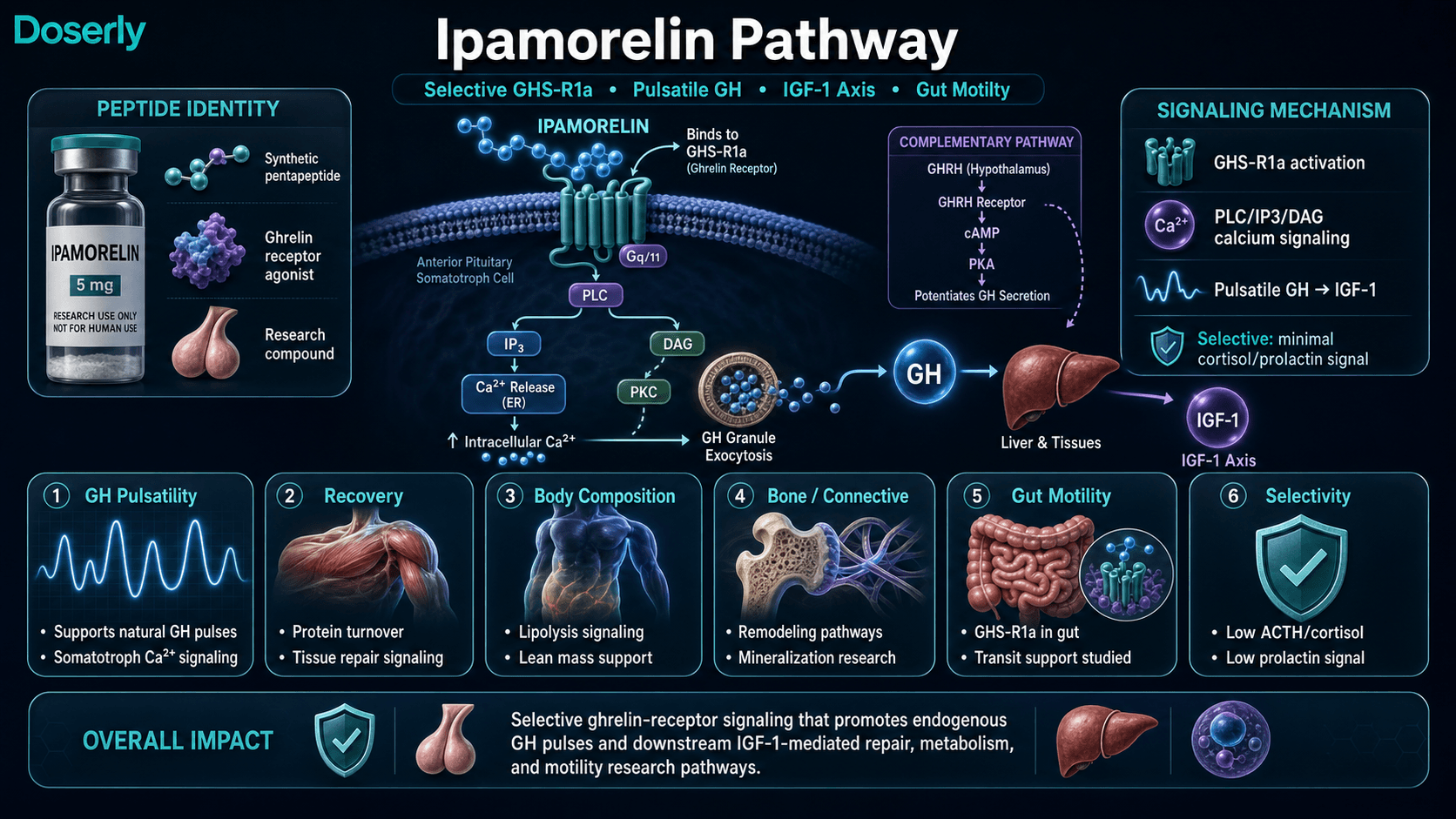
Ipamorelin binds with high affinity to the growth hormone secretagogue receptor type 1a (GHS-R1a), a G protein-coupled receptor expressed primarily on anterior pituitary somatotrophs. Receptor activation initiates intracellular signaling through Gq/11-mediated phospholipase C (PLC) activation, generating the second messengers inositol 1,4,5-trisphosphate (IP3) and diacylglycerol (DAG). IP3 mobilizes intracellular calcium stores from the endoplasmic reticulum, elevating cytoplasmic [Ca²⁺] from approximately 100 nM to 500-1000 nM, which triggers exocytosis of GH-containing secretory granules [1][5].
This signaling cascade is mechanistically distinct from the GHRH pathway, which signals through Gs-coupled adenylyl cyclase activation, elevating cAMP and activating protein kinase A (PKA). The convergence of these two independent pathways on somatotroph cells provides the mechanistic basis for the well-documented synergy between ipamorelin and GHRH analogs, where co-administration produces GH responses 1.5 to 3-fold greater than the arithmetic sum of individual responses [5].
The selectivity profile of ipamorelin is its defining pharmacological feature. In the original characterization study, Raun et al. (1998) demonstrated that GHRP-6 at equipotent GH-releasing doses elevated plasma cortisol concentrations by 30-50%, while ipamorelin at equivalent and supraphysiological doses produced no significant cortisol elevation [1]. This selectivity was confirmed for ACTH, prolactin, aldosterone, TSH, and FSH [1]. The molecular basis for this selectivity lies in the strategic amino acid modifications within the pentapeptide sequence, particularly the Aib residue at the N-terminus and the D-amino acid substitutions at positions 3 and 4.
Electrophysiological studies of isolated somatotroph cells demonstrate that ipamorelin induces characteristic calcium oscillations and membrane depolarization patterns consistent with physiological pulsatile GH release, rather than inducing non-physiological sustained secretion [5]. This preservation of pulsatile secretory dynamics is clinically relevant, as it maintains endogenous feedback regulation through the GH-IGF-1 axis.
Pathway Visualization Image
Pharmacokinetics
The Basics
Ipamorelin is a relatively fast-acting, short-lived peptide. After a subcutaneous injection, it gets absorbed quickly (within about 15-20 minutes), triggers a burst of growth hormone that peaks around 30-60 minutes later, and then clears out of your system within a few hours. The half-life of approximately 2 hours means that by about 4 hours after injection, most of the peptide has been eliminated.
This short half-life is actually part of the design. By triggering a quick, clean pulse of GH and then clearing out, ipamorelin mimics the natural pulsatile pattern your body uses for growth hormone release. This is considered more physiological than approaches that keep GH levels constantly elevated, and it is one reason why chronic daily dosing has not shown significant receptor desensitization in animal studies [6].
Growth hormone levels peak roughly 30-45 minutes after injection and return toward baseline within 3-4 hours. This timeline is important for practical use: bedtime dosing is common because it aligns ipamorelin's GH pulse with the natural nocturnal peak, and the fasting requirement (food intake can blunt GH response) is more manageable at night.
The Science
Following subcutaneous administration, ipamorelin demonstrates rapid absorption with peak plasma concentrations (Cmax) achieved within 30-60 minutes. The absorption half-life approximates 15-20 minutes, while the terminal elimination half-life ranges from 90-120 minutes [7].
Pharmacokinetic-pharmacodynamic modeling in healthy male volunteers demonstrated dose-proportional kinetics across a range of approximately 4-140 nmol/kg administered intravenously, with a single well-defined GH pulse peaking at approximately 0.67 hours post-dose and returning to baseline thereafter [7]. The volume of distribution is consistent with extracellular fluid distribution, suggesting limited tissue accumulation and minimal blood-brain barrier penetration at therapeutic doses [5].
Metabolism occurs primarily through peptidase-mediated hydrolysis, with renal clearance as the principal elimination route. The compound does not demonstrate significant organ accumulation [8]. Dose-response studies establish a sigmoidal curve with threshold effects at approximately 0.1 mcg/kg body weight, an EC50 of approximately 0.3-0.4 mcg/kg, and plateau responses beginning at 0.5-1.0 mcg/kg [5][7].
Notably, a three-week chronic dosing study in rats showed no significant desensitization of GH release mechanisms with daily ipamorelin administration, in contrast to hexarelin and other GHRPs that exhibit progressive GH response attenuation with continuous use [6].
Research & Clinical Evidence
Growth Hormone Selectivity
The Basics
The foundational research on ipamorelin established something that no previous growth hormone peptide had achieved: truly selective GH release. In the original 1998 study, researchers showed that ipamorelin could trigger a powerful growth hormone pulse without increasing stress hormones or prolactin, even at doses far above what was needed for GH release. This selectivity is the single most important finding in ipamorelin research, because it means the GH benefits can be accessed without the hormonal side effects that limited earlier compounds.
The Science
Raun et al. (1998) demonstrated in swine and rat models that ipamorelin released GH with potency comparable to GHRP-6 (ED50 80-115 nmol/kg) while producing no significant elevation of ACTH, cortisol, or prolactin at doses up to 200-fold higher than the GH-effective dose [1]. This selectivity ratio exceeds 100x for GH specificity over other hormonal axes. The study established ipamorelin as the first truly selective growth hormone secretagogue, a classification that remains unique among injectable GHRPs.
Bone Health and Growth
The Basics
Several animal studies suggest that ipamorelin may support bone health. In young rats, it increased the rate of bone growth by up to 24% over two weeks and increased bone mineral density in both leg and spine bones. Separate research showed it could counteract the bone-damaging effects of corticosteroid medications, potentially offering protection for people who require long-term steroid use.
The Science
Johansen et al. (1999) demonstrated dose-dependent longitudinal bone growth in adolescent female rats receiving ipamorelin at 18-450 mcg/day for 15 days, with growth rates increasing from a baseline of 42 mcm/day to 52 mcm/day at the highest dose (24% increase), without abnormal bone turnover markers [9]. Svensson et al. (2000) showed that both ipamorelin and GHRP-6 increased total bone mineral content in the legs and spine of adult female rats, with expanded cortical bone area and increased ash weight (mineral density) [10]. Andersen et al. (2001) demonstrated that ipamorelin counteracted glucocorticoid-induced decreases in bone formation, producing a four-fold increase in bone formation rates in steroid-treated rats [11].
Gastrointestinal Motility and Postoperative Ileus
The Basics
One of ipamorelin's more unusual research areas is gut motility. After abdominal surgery, the digestive system can temporarily shut down (a condition called postoperative ileus, or POI), which delays recovery and extends hospital stays. Ipamorelin was investigated as a potential treatment for this condition because it activates ghrelin receptors in the gut that help restart digestive movement. Animal studies showed it could restore normal gut function after surgical trauma. A Phase II human clinical trial showed it shortened the time to first tolerated meal by about 12 hours, though the trial was ultimately discontinued because the overall efficacy was not deemed sufficient for commercial development.
The Science
Preclinical studies demonstrated that ipamorelin reversed surgery-induced gastric paralysis in rat models. Greenwood-Van Meerveld et al. (2012) showed that ipamorelin administration (0.014-0.14 mcmol/kg IV) normalized gastric emptying from 78% retention to 25-52% (comparable to non-surgical controls), restored acetylcholine-mediated muscle contractility, and reactivated neural signaling in surgically stressed gut tissue [2]. A subsequent study confirmed that food transit location in the GI tract normalized to non-POI patterns following ipamorelin treatment [12].
Beck et al. (2014) conducted a prospective, randomized, controlled, proof-of-concept Phase II trial evaluating ipamorelin (0.03 mg/kg IV twice daily) for POI management in bowel resection patients. While the compound was well-tolerated and demonstrated biological plausibility, it did not meet its primary efficacy endpoints of significantly reducing time to first tolerated meal or bowel movement compared to placebo [3].
Insulin Secretion
The Basics
Research in diabetic animal models found that ipamorelin can stimulate insulin release from pancreatic cells. This is a secondary effect related to its calcium signaling activity and is an area of early investigation, not an established therapeutic application.
The Science
Adeghate and Ponery (2004) demonstrated ipamorelin-evoked insulin release from both normal and diabetic rat pancreas tissue, likely mediated through indirect stimulation of calcium channels on pancreatic islet cells [4]. This finding has implications for understanding the broader metabolic effects of GHS-R1a activation but has not been pursued in human clinical studies.
Nitrogen Balance and Anti-Catabolic Effects
The Basics
Animal research suggests ipamorelin may help counteract muscle wasting, particularly in the context of corticosteroid use. Rats treated with steroids showed less nitrogen loss (a marker of muscle breakdown) when also receiving ipamorelin.
The Science
Aagaard et al. (2009) demonstrated reduced nitrogen wasting and improved nitrogen balance in steroid-treated rats receiving ipamorelin, suggesting potential anti-catabolic properties that may complement the compound's anabolic GH-stimulating effects [13].
Biomarker Evidence Matrix
The following matrix scores ipamorelin across relevant biomarker categories based on available research evidence and community-reported experiences. Only categories with sufficient data are scored.
Category
Sleep Quality
- Evidence Strength (1-10)
- 4
- Reported Effectiveness (1-10)
- 7
- Summary
- No direct clinical sleep studies, but GH pulsatility mechanisms strongly support sleep improvement. Community reports consistently identify sleep as the earliest and most reliable benefit.
Category
Recovery & Healing
- Evidence Strength (1-10)
- 5
- Reported Effectiveness (1-10)
- 7
- Summary
- Animal studies demonstrate tissue repair, nitrogen balance, and anti-catabolic effects. Community reports recovery as the second most consistent benefit, appearing weeks 2-4.
Category
Fat Loss
- Evidence Strength (1-10)
- 4
- Reported Effectiveness (1-10)
- 6
- Summary
- GH-mediated lipolysis is well-established mechanistically. Community reports mixed: some see meaningful body composition changes, others notice minimal fat loss. Heavily confounded by concurrent compounds.
Category
Muscle Growth
- Evidence Strength (1-10)
- 4
- Reported Effectiveness (1-10)
- 5
- Summary
- GH/IGF-1 axis supports protein synthesis. Community reports mixed: lean mass retention and definition noted, but dramatic hypertrophy not consistently reported.
Category
Physical Performance
- Evidence Strength (1-10)
- 3
- Reported Effectiveness (1-10)
- 6
- Summary
- Limited direct evidence. Community reports improved workout capacity and endurance in some users.
Category
Energy Levels
- Evidence Strength (1-10)
- 3
- Reported Effectiveness (1-10)
- 5
- Summary
- No direct evidence. Community reports mixed with some subtle energy improvements noted.
Category
Bone Health
- Evidence Strength (1-10)
- 6
- Reported Effectiveness (1-10)
- N/A
- Summary
- Multiple animal studies demonstrate increased bone mineral content, longitudinal growth, and protection against glucocorticoid-induced bone loss [9][10][11]. No community data.
Category
Gut Health
- Evidence Strength (1-10)
- 6
- Reported Effectiveness (1-10)
- N/A
- Summary
- Preclinical and Phase II clinical evidence for gastric motility improvement via GHSR-1a in gut tissue [2][3][12]. Not a commonly discussed community benefit.
Category
Mood & Wellbeing
- Evidence Strength (1-10)
- 2
- Reported Effectiveness (1-10)
- 5
- Summary
- No direct evidence. Occasional community mentions of mood improvement, but not a dominant signal.
Category
Skin Health
- Evidence Strength (1-10)
- 3
- Reported Effectiveness (1-10)
- 5
- Summary
- GH/IGF-1 supports collagen synthesis theoretically. Limited community reports of skin improvement. One report of acne as a negative signal.
Category
Joint Health
- Evidence Strength (1-10)
- 3
- Reported Effectiveness (1-10)
- 5
- Summary
- GH supports connective tissue repair theoretically. Limited isolated community reports.
Category
Side Effect Burden
- Evidence Strength (1-10)
- 7
- Reported Effectiveness (1-10)
- 7
- Summary
- Strong preclinical and clinical evidence for excellent tolerability and selectivity [1][3]. Community strongly agrees this is the safest GH secretagogue.
Category
Nausea & GI Tolerance
- Evidence Strength (1-10)
- 7
- Reported Effectiveness (1-10)
- 7
- Summary
- Clinical trial data shows tolerability comparable to placebo [3]. Community reports excellent GI tolerance. Pro-motility effects may be beneficial.
Category
Appetite & Satiety
- Evidence Strength (1-10)
- 5
- Reported Effectiveness (1-10)
- 4
- Summary
- Preclinical data suggests no appetite stimulation despite ghrelin receptor action [1]. Community reports split: some experience unexpected hunger, others confirm no appetite change.
Categories not scored (insufficient data): Weight Management, Food Noise, Focus & Mental Clarity, Memory & Cognition, Anxiety, Stress Tolerance, Motivation & Drive, Emotional Aliveness, Emotional Regulation, Libido, Sexual Function, Inflammation, Pain Management, Digestive Comfort, Hair Health, Heart Health, Blood Pressure, Heart Rate & Palpitations, Hormonal Symptoms, Temperature Regulation, Fluid Retention, Body Image, Immune Function, Longevity & Neuroprotection, Cravings & Impulse Control, Social Connection, Treatment Adherence, Withdrawal Symptoms, Daily Functioning.
Benefits & Potential Effects
The Basics
Ipamorelin's benefits trace back to one core action: stimulating your body to release more of its own growth hormone. Because growth hormone influences so many systems (muscle, fat, bone, skin, sleep, and tissue repair), the potential benefits are broad. However, it is important to set realistic expectations. Ipamorelin is not synthetic HGH. It works with your body's existing capacity, which means the effects are generally more subtle, more gradual, and more physiological than exogenous growth hormone therapy.
The most consistently reported benefits in community experiences are improved sleep quality and faster recovery from exercise. These tend to appear within the first two weeks and are the effects users most commonly cite as justifying continued use. Body composition changes (modest fat loss, improved muscle tone and definition) tend to emerge more gradually over 6-12 weeks, and are less dramatic than what is commonly marketed. Some users report improvements in skin quality, energy levels, and general wellbeing, though these are more variable across individuals.
The compound's selectivity means that it supports these benefits while avoiding the cortisol elevation, prolactin increase, and intense appetite stimulation that come with other growth hormone peptides. For individuals who have tried GHRP-6 or GHRP-2 and found the side effects unacceptable, ipamorelin offers a gentler alternative with a more manageable side effect profile.
The Science
The therapeutic potential of ipamorelin derives from its stimulation of endogenous pulsatile GH secretion and consequent elevation of IGF-1. Growth hormone exerts anabolic effects through multiple mechanisms: enhanced amino acid uptake and protein synthesis, stimulation of lipolysis in adipose tissue (preferentially visceral depots), support of bone remodeling and mineralization, and promotion of tissue repair processes [5].
Clinical and preclinical evidence supports the following benefit domains:
Body Composition: Studies in adults with relative GH insufficiency demonstrate measurable lean body mass increases (typically 1-3 kg) and fat mass reductions (1-2 kg) over 8-24 week protocols, with effects more pronounced in individuals with lower baseline IGF-1 levels [5]. Lipolytic effects appear preferentially distributed to visceral rather than subcutaneous adipose depots.
Bone Health: Multiple preclinical studies demonstrate dose-dependent increases in bone mineral content, longitudinal bone growth, and protection against glucocorticoid-induced bone loss [9][10][11].
Gastrointestinal Motility: GHSR-1a activation in gut tissue promotes gastric emptying and intestinal transit, demonstrated in both preclinical POI models and a Phase II human trial [2][3][12].
Protein Metabolism: Stable isotope tracer studies demonstrate that GH secretagogue administration shifts whole-body protein turnover toward net anabolism, with increased protein synthesis rates and positive nitrogen balance [13].
Side Effects & Safety Considerations
The Basics
Ipamorelin has earned a reputation as one of the most well-tolerated peptides in its class, and the available evidence supports this. The most commonly reported side effect is a mild, transient facial flushing or warm sensation in the first few minutes after injection. Some people describe this as a brief lightheadedness that passes quickly and is not unpleasant. Beyond that, occasional water retention and mild injection site reactions (redness, slight swelling) have been reported.
A notable point: despite ipamorelin being marketed as "non-appetite-stimulating" (a key advantage over GHRP-6), some community users do report increased hunger. This appears to be a minority experience, but it is worth knowing about if appetite management is a priority, particularly for those combining ipamorelin with weight loss protocols.
Any compound that raises growth hormone and IGF-1 levels carries theoretical concerns around glucose metabolism (GH can reduce insulin sensitivity) and the potential to promote growth in any existing tumors. IGF-1 monitoring through blood work is recommended by practitioners who oversee these protocols, particularly for longer-term use.
The Science
The safety profile of ipamorelin has been characterized across preclinical studies and the Phase II POI clinical trial. In the POI trial, adverse event rates were comparable to placebo, with the most commonly reported events being headache, GI complaints, and injection site reactions [3]. The compound's defining safety advantage is its selectivity: at GH-effective and supraphysiological doses, it produces no significant elevation of cortisol, ACTH, or prolactin [1].
Reported and theoretical adverse effects include:
- Injection site reactions: Mild erythema and transient discomfort, typical of subcutaneous peptide administration
- Transient flushing/lightheadedness: Brief vasodilation effect post-injection, self-limiting
- Water retention: Mild, particularly during initial use, consistent with GH axis activation
- Appetite changes: Despite selectivity for GH over appetite pathways in preclinical models, some individuals report subjective hunger increases
- Elevated heart rate: Rare reports of increased heart rate with bedtime dosing
- Glucose metabolism: Theoretical concern with sustained IGF-1 elevation; fasting glucose and HbA1c monitoring recommended [5]
- Active malignancy: Contraindicated due to GH/IGF-1 proliferative potential
- Pregnancy/lactation: Insufficient safety data; avoidance recommended
Monitoring parameters recommended by practitioners include: IGF-1 levels (to ensure therapeutic range without supraphysiological elevation), fasting glucose/HbA1c, comprehensive metabolic panel, and clinical assessment for edema, joint pain, and paresthesias [5].
Dosing Protocols
The Basics
Ipamorelin dosing centers around a few key principles: start low, titrate gradually, inject on an empty stomach, and time it to align with your body's natural growth hormone patterns (typically before bed).
Most sources describe a range of 100-300 mcg per injection for standard protocols, with some advanced protocols reaching 500 mcg. The most commonly cited single daily dose is 200-300 mcg administered subcutaneously 30-60 minutes before bedtime. Some practitioners describe protocols using 2-3 injections per day (morning fasted and pre-bed, or morning, pre-workout, and pre-bed) for more sustained GH elevation.
A typical gradual titration approach starts at 100 mcg daily for the first two weeks and increases by approximately 50 mcg every one to two weeks, reaching 200-250 mcg by weeks 5-12. Cycle length is generally 8-12 weeks, with some sources supporting extension to 16-24 weeks for those who tolerate it well. An off-cycle period of 2-4 weeks (or up to 8 weeks) is commonly recommended between cycles.
Commonly reported dosing ranges span from 100 to 500 mcg per injection, with the most frequently cited range being 200-300 mcg. Protocols vary from once daily to three times daily. Cycle length ranges from 8 weeks to 1 year depending on practitioner philosophy and lab monitoring approach. There is no established consensus on an optimal dose, frequency, or cycle length. Consultation with a healthcare professional is essential for determining an individualized approach.
Fasting requirement: Food intake can blunt the GH response to ipamorelin by raising insulin. Most sources recommend fasting for at least 2 hours before injection and waiting 30-60 minutes after injection before eating, particularly carbohydrates.
The Science
Clinical pharmacokinetic-pharmacodynamic modeling established dose-response characteristics across 0.1-1.0 mcg/kg body weight, with a sigmoidal dose-response curve, EC50 of approximately 0.3-0.4 mcg/kg, and plateau responses at 0.5-1.0 mcg/kg [7]. For a 75 kg individual, the EC50 corresponds to approximately 22.5-30 mcg, while plateau effects begin at 37.5-75 mcg. These clinical values are considerably lower than the community-reported dose ranges, reflecting the distinction between single-dose GH stimulation parameters and protocol-level dosing intended for sustained physiological effects.
The Phase II POI trial used 0.03 mg/kg (approximately 2.25 mg for a 75 kg individual) administered intravenously twice daily, which is substantially higher than typical subcutaneous community protocols [3]. This dose was selected for its robust pro-motility effects rather than optimization of GH secretion.
Inter-individual variability is documented, with older subjects and those with higher adiposity demonstrating attenuated GH responses compared to younger, lean individuals [5].
Consistency is the difference between a protocol that delivers results and one that wastes time and money. Doserly was built for exactly this: keeping you on track with the precision your protocol demands.
The built-in calculators handle the math you shouldn't be doing in your head. The reconstitution calculator tells you exactly how much bacteriostatic water to add for your target concentration. The dose calculator converts between units, milligrams, and syringe markings so you draw the right amount every time. The injection site heat map tracks where you've administered and when, helping you rotate sites systematically to reduce tissue damage, scarring, and absorption inconsistencies from overusing the same area. Pair that with smart reminders tuned to your protocol's timing requirements, and you build the kind of daily consistency that separates optimized protocols from haphazard ones.
Turn symptom and safety notes into a clearer timeline.
Doserly helps you log doses, symptoms, and safety observations side by side so patterns are easier to discuss with a qualified clinician.
Pattern view
Logs and observations

Pattern visibility is informational and should be reviewed with a clinician.
What to Expect
Ipamorelin is not a fast-acting compound with dramatic overnight effects. Benefits accumulate gradually over weeks to months, and individual responses vary considerably. Here is a general timeline drawn from research data and community experiences:
Weeks 1-2: The earliest reported changes are typically related to sleep. Many users describe deeper, more restful sleep within the first week. Mild injection-site reactions (redness, brief warmth or flushing) are common initially and usually diminish. Some users notice subtle improvements in morning energy and general wellbeing. It is too early to expect visible body composition changes.
Weeks 3-4: Recovery from exercise begins to improve for many users, with less muscle soreness and faster bounce-back between workouts. Some report improved skin hydration and early hair quality changes. Sleep benefits generally continue. If appetite changes are going to occur, they typically become apparent during this period.
Weeks 5-8: Body composition changes become more noticeable for those who respond well, particularly improved muscle definition and tone rather than dramatic muscle size increases. Modest fat loss, especially around the midsection, is reported by some users. IGF-1 levels, if monitored through blood work, typically reach their new steady state during this window.
Weeks 9-12+: Cumulative benefits continue to accrue. Users who report the strongest results tend to be those who have maintained consistent dosing, strict fasting protocols, quality sleep, and regular resistance training throughout the cycle. Those who have not noticed meaningful changes by week 8 are unlikely to see dramatic improvements at later timepoints.
After discontinuation: Most users report a gradual return toward baseline over several weeks. There are no commonly reported withdrawal effects or rebound symptoms. Some users note that recovery and sleep benefits were the first to fade after stopping.
Reality check: A significant number of community users report subtle or no noticeable effects from ipamorelin, particularly at lower doses or shorter durations. This is consistent with the compound's mechanism: it enhances your body's own GH production rather than replacing it, which means results depend heavily on your baseline GH secretory capacity, age, body composition, and lifestyle factors.
The week-by-week expectations above are drawn from research and community reports, but your experience will be uniquely yours. Doserly's biomarker tracking transforms those general timelines into personal data points you can actually see and measure.
Log the specific markers relevant to this compound, whether that's pain levels, energy, sleep quality, body composition, recovery time, or mood, and watch your own trend lines emerge over weeks and months. Did your key markers start shifting in week three, like the research suggests? Is your experience tracking with what the community reports, or diverging? Over time, this creates something more valuable than any guide: an evidence-based picture of how your body responds to this specific compound, at your specific dose, within your specific health context.
Build reminders around the routine, not just the compound.
Doserly can keep timing, skipped doses, and schedule changes organized so the plan you read about becomes easier to follow and review.
Today view
Upcoming reminders
Reminder tracking supports consistency; it does not select a protocol for you.
Interaction Compatibility
Good With (Synergistic Compounds)
- CJC-1295 (with or without DAC): The most commonly recommended pairing. CJC-1295 stimulates GH release through the GHRH pathway while ipamorelin works through the ghrelin receptor pathway. The two complementary mechanisms produce synergistic GH responses 1.5-3x greater than either alone. Available as pre-mixed blends.
- Tesamorelin: Another GHRH analog that pairs synergistically with ipamorelin for the same mechanistic reasons as CJC-1295. Tesamorelin has FDA approval for HIV-associated lipodystrophy and may offer advantages for visceral fat reduction.
- Sermorelin: GHRH analog with a long clinical history. Similar synergistic rationale as CJC-1295 but with a shorter half-life requiring more frequent dosing.
- BPC-157 / TB-500: Healing peptides that can complement ipamorelin's recovery support. Different mechanisms (tissue repair vs. GH stimulation) may provide additive recovery benefits.
- GHK-Cu: Copper peptide for skin and tissue repair that complements ipamorelin's collagen-supporting GH effects.
- DSIP: Delta sleep-inducing peptide that may enhance sleep architecture when combined with ipamorelin's nocturnal GH enhancement.
- Epithalon: Longevity peptide that some practitioners combine with ipamorelin for anti-aging protocols.
- MOTS-C: Mitochondrial peptide for metabolic support. Some community protocols pair MOTS-C in the morning with ipamorelin at night.
Not Good With (Cautions and Contraindications)
- Other GHRPs (GHRP-2, GHRP-6, Hexarelin): These peptides work through the same ghrelin receptor pathway. Combining them with ipamorelin does not produce synergy (same mechanism) and increases the risk of receptor desensitization and off-target hormonal effects that ipamorelin is specifically designed to avoid.
- MK-677 (Ibutamoren): Oral GHS-R1a agonist. Same receptor target as ipamorelin, so combining provides redundant rather than complementary stimulation.
- GLP-1 agonists (Semaglutide, Tirzepatide, Retatrutide): These can slow gastric emptying and potentially blunt GH response timing. Community practitioners recommend extending the fasting window to 2-4 hours when combining. Not contraindicated, but timing coordination is important.
- Exogenous HGH: Concurrent use may suppress endogenous GH production via negative feedback, potentially reducing ipamorelin's effectiveness.
- Insulin: GH and insulin have opposing metabolic effects. Concurrent administration requires careful glucose monitoring and professional oversight.
Administration Guide
Ipamorelin is administered via subcutaneous injection, the same method used for insulin and many other peptide compounds. The process requires standard injection supplies and attention to timing.
Materials required:
- U-100 insulin syringes (29-31 gauge, 5/16 to 1/2 inch needle; consider 30 or 50-unit syringes for small volume doses under 10 units)
- Alcohol swabs (70% isopropyl)
- Sharps disposal container
- Bacteriostatic water for reconstitution
- Gauze or cotton pads
Recommended reconstitution solution: Bacteriostatic water (0.9% benzyl alcohol). Sterile water can be used but reduces shelf life significantly. Typical reconstitution volumes are 2.0-3.0 mL per vial, depending on vial size and desired concentration.
Timing considerations: Most practitioners recommend administering ipamorelin on an empty stomach, with at least 2 hours of fasting before injection and 30-60 minutes of fasting after injection. Food intake, particularly carbohydrates, raises insulin levels that can blunt the pituitary's GH response to ipamorelin. Bedtime dosing (30-60 minutes before sleep) is the most commonly cited timing to align with natural nocturnal GH peaks. Some protocols add a morning fasted dose or a pre-workout dose for those seeking additional GH pulses.
Post-administration care: A brief, mild facial flush or lightheadedness lasting a few minutes is commonly reported after injection and is not cause for concern. Monitor for any unusual or persistent injection site reactions. Document dose, injection site, and time for consistency tracking. If combining with GLP-1 agonists, coordinate timing to account for delayed gastric emptying.
Supplies & Planning
Ipamorelin is commercially available as a lyophilized (freeze-dried) powder in vials, most commonly in 5 mg and 10 mg sizes.
General supplies associated with ipamorelin protocols:
- Peptide vials: Available in 5 mg and 10 mg sizes. The number of vials needed depends on daily dose and cycle length; consult your healthcare provider and use a reconstitution calculator for specifics.
- Bacteriostatic water: Typically one 10 mL bottle is sufficient for multiple vials, as each vial requires approximately 2.0-3.0 mL for reconstitution.
- Insulin syringes: U-100 insulin syringes (29-31 gauge). One per injection. Use smaller-capacity syringes (30 or 50-unit) for doses under 10 units to improve measurement accuracy.
- Alcohol swabs: Two per injection session (one for vial stopper, one for injection site).
- Sharps container: For safe disposal of used syringes.
- Storage supplies: Refrigerator space for reconstituted vials; freezer space for long-term lyophilized storage.
Readers should consult their healthcare provider for guidance on quantities and use the reconstitution calculator for preparation specifics.
Storage & Handling
Proper storage is essential for maintaining peptide potency and sterility throughout a protocol.
Lyophilized (powder) form:
- Short-term: Refrigerate at 2-8°C (35.6-46.4°F) for weeks to months
- Long-term: Freeze at -20°C (-4°F) for up to 2-3 years
- Store in original sealed packaging with desiccant to minimize moisture exposure
- Keep in a dry, dark environment; peptides are light-sensitive and hygroscopic
- Allow vials to reach room temperature (10-30 minutes) before opening to prevent condensation inside the vial
Reconstituted (liquid) form:
- Refrigerate at 2-8°C (35.6-46.4°F) immediately after reconstitution
- Use within 4 weeks (28 days) when reconstituted with bacteriostatic water
- Do NOT freeze reconstituted solutions; freezing denatures peptides
- Avoid repeated freeze-thaw cycles
- For longer storage: aliquot into sterile single-use vials, freeze aliquots at -20°C, and thaw each aliquot only once
Handling best practices:
- Swab vial stopper with alcohol before every draw
- Use sterile needles and syringes for every injection
- Inspect reconstituted solution before each use: it should be clear, colorless, and free of particles or cloudiness
- Discard any solution showing cloudiness, discoloration, or particulates
- Label reconstituted vials with the reconstitution date
Lifestyle Factors
The effectiveness of ipamorelin is significantly influenced by lifestyle factors. The compound works by enhancing your body's natural GH secretory capacity, which means the conditions surrounding its use matter considerably.
Fasting and meal timing: This is arguably the most critical lifestyle factor for ipamorelin. Insulin blunts pituitary GH release, so elevated insulin from recent food intake can significantly reduce the GH pulse triggered by ipamorelin. Most practitioners recommend a minimum of 2 hours fasted before injection and 30-60 minutes fasted afterward. Carbohydrates and sugars have the strongest insulin-elevating effect and should be avoided in this window.
Sleep: Growth hormone secretion is naturally highest during deep sleep. Bedtime ipamorelin dosing is designed to amplify this nocturnal peak. Prioritizing 7-9 hours of quality sleep and maintaining consistent sleep/wake times maximizes the compound's alignment with natural GH rhythms.
Exercise: Resistance training and high-intensity exercise are powerful natural GH stimulators that complement ipamorelin's effects. Regular training, particularly compound movements and progressive overload, supports the muscle-building and body composition goals that most ipamorelin users pursue. Some practitioners recommend a pre-workout dose 30-45 minutes before training.
Nutrition: A protein-adequate diet supports the muscle protein synthesis and tissue repair that GH/IGF-1 elevation facilitates. Without sufficient protein intake, the anabolic signal from increased GH has less raw material to work with.
Stress management: Chronic stress elevates cortisol, which antagonizes GH effects and promotes visceral fat storage. While ipamorelin itself does not raise cortisol, managing baseline stress levels supports the metabolic environment in which the compound operates.
Lab monitoring: Practitioners who oversee ipamorelin protocols typically recommend quarterly blood work including IGF-1 (to confirm response and avoid supraphysiological levels), fasting glucose/HbA1c (to monitor insulin sensitivity), and a comprehensive metabolic panel.
Peptide protocols don't exist in a vacuum. Your nutrition, exercise, sleep, stress, and the rest of your health stack all influence outcomes. Doserly tracks your entire health picture in one place: peptides, supplements, medications, TRT/HRT, and the lifestyle factors that determine whether your protocol reaches its potential.
This holistic view reveals correlations that compartmentalized tracking misses. You might discover that your recovery improvements stall during weeks with poor sleep, or that adding a specific supplement amplified a benefit you were already seeing. Doserly's cross-category visibility helps you understand which lifestyle factors are pulling the most weight in your results, turning health optimization from guesswork into a data-informed practice.
Keep sensitive protocol records in a purpose-built app.
Doserly is designed for private health tracking with structured records, offline-ready workflows, and exportable history when you need it.
Privacy
Health records

Privacy controls help you manage records; keep clinical records where required.
Regulatory Status & Research Classification
United States (FDA): Ipamorelin is not approved by the FDA for any therapeutic indication. It is classified as an investigational compound. A Phase II clinical trial for postoperative ileus was conducted (NCT identifier pending verification) but did not advance to Phase III. The compound has been available through compounding pharmacies in some contexts.
Canada (Health Canada): Not approved. No DIN or NPN assigned. Available through specialized compounding pharmacies in some contexts.
United Kingdom (MHRA): Not approved for therapeutic use. Not classified as a controlled substance.
Australia (TGA): Not a registered therapeutic good. Scheduling status is consistent with research compounds.
European Union (EMA): No marketing authorization. Ipamorelin remains an investigational compound in EU jurisdictions.
WADA Status: Ipamorelin is classified as a prohibited substance under Section S2 of the WADA Prohibited List (Peptide Hormones, Growth Factors, Related Substances and Mimetics). This prohibition applies both in-competition and out-of-competition. Detection methods utilizing liquid chromatography-mass spectrometry have been developed and implemented in anti-doping laboratories [8].
Active clinical trials: The Phase II POI trial (Beck et al., 2014) is the most significant registered human trial. No currently active registered trials for ipamorelin are identified in ClinicalTrials.gov as of the publication date of this guide.
Regulatory status changes frequently. Always verify the current legal status of any compound in your specific country or jurisdiction before making any decisions.
FAQ
What is ipamorelin, and how is it different from HGH?
Ipamorelin is a peptide that stimulates your pituitary gland to release your own growth hormone in natural pulses. HGH (human growth hormone) is direct replacement of the hormone itself. The key difference is that ipamorelin works with your body's feedback mechanisms, producing physiological pulsatile release, while exogenous HGH bypasses those mechanisms. Ipamorelin produces more modest GH elevation but maintains natural regulation, while HGH provides higher and more sustained GH levels.
How long does it take to notice effects from ipamorelin?
Based on community reports, the most commonly reported early effects are improvements in sleep quality, typically noticed within the first 1-2 weeks. Recovery benefits are generally reported around weeks 2-4. Visible body composition changes, if they occur, tend to emerge around weeks 6-12. Individual responses vary significantly, and some users report minimal noticeable effects.
Can I take ipamorelin without combining it with CJC-1295?
Yes. While the CJC-1295/Ipamorelin stack is the most commonly recommended combination due to their synergistic mechanisms, ipamorelin can be used as a standalone compound. Solo protocols are simpler and less expensive, though the GH elevation is more modest than combined protocols.
Why do I need to fast before and after injecting ipamorelin?
Food intake, especially carbohydrates, raises insulin levels. Elevated insulin blunts the pituitary gland's GH release in response to ipamorelin. Fasting for at least 2 hours before and 30-60 minutes after injection creates the low-insulin environment needed for an optimal GH pulse.
Does ipamorelin increase appetite?
Based on preclinical data, ipamorelin is more selective than GHRP-6 and does not significantly stimulate appetite through the same mechanisms. However, some community users do report increased hunger as a subjective experience. This appears to be a minority response, but it is worth being aware of, particularly for those on weight loss protocols.
Is ipamorelin safe for long-term use?
Long-term human safety data for ipamorelin is limited, as most clinical studies span weeks to months rather than years. Animal studies suggest no significant receptor desensitization with chronic daily dosing [6]. Theoretical concerns with sustained GH/IGF-1 elevation include effects on glucose metabolism and potential proliferative effects. Practitioners who oversee longer protocols typically recommend regular lab monitoring including IGF-1, fasting glucose, and comprehensive metabolic panels. Consultation with a healthcare professional is strongly recommended for protocol planning and monitoring.
What happens when I stop taking ipamorelin?
Community reports indicate a gradual return toward baseline GH/IGF-1 levels over several weeks after discontinuation. There are no commonly reported withdrawal effects or rebound symptoms. Some users note that sleep and recovery benefits are the first to diminish after stopping.
Can women use ipamorelin?
Ipamorelin does not have gender-specific contraindications based on available data. Some community sources describe it as well-suited for women due to its gentle side effect profile and absence of androgenic effects. Dosing ranges reported in community discussions are generally the same for both men and women, though individualization based on body weight and response is always recommended in consultation with a healthcare provider.
Sources & References
Preclinical Pharmacology:
[1] Raun K, Hansen BS, Johansen NL, Thogersen H, Madsen K, Ankersen M, Andersen PH. Ipamorelin, the first selective growth hormone secretagogue. European Journal of Endocrinology. 1998;139(5):552-561. DOI: 10.1530/eje.0.1390552. https://pubmed.ncbi.nlm.nih.gov/9849822/
Clinical Studies (Human):
[2] Greenwood-Van Meerveld B, Tyler K, Mohammadi E, Pietra C. Efficacy of ipamorelin, a ghrelin mimetic, on gastric dysmotility in a rodent model of postoperative ileus. Journal of Experimental Pharmacology. 2012;4:149-155. https://pubmed.ncbi.nlm.nih.gov/19289567/
[3] Beck DE, Sweeney WB, McCarter MD, and Ipamorelin 201 Study Group. Prospective, randomized, controlled, proof-of-concept study of the ghrelin mimetic ipamorelin for the management of postoperative ileus in bowel resection patients. International Journal of Colorectal Disease. 2014;29(12):1527-1534. https://pubmed.ncbi.nlm.nih.gov/24433546/
[4] Adeghate E, Ponery AS. Mechanism of ipamorelin-evoked insulin release from the pancreas of normal and diabetic rats. Neuro Endocrinology Letters. 2004;25(6):403-406. https://pubmed.ncbi.nlm.nih.gov/15665803/
Pharmacology and Reviews:
[5] Sigalos JT, Pastuszak AW, Khera M. The Use of Peptide Hormones in Sports and Wellness. Sexual Medicine Reviews. 2021;9(2):292-299. https://pubmed.ncbi.nlm.nih.gov/32418878/
[6] Johansen PB, et al. Three-week chronic in vivo ipamorelin treatment: no desensitization of GH release mechanisms. European Journal of Anatomy. 2002.
[7] Gobburu JV, Agerso H, Jusko WJ, Ynddal L. Pharmacokinetic-pharmacodynamic modeling of ipamorelin, a growth hormone releasing peptide, in human volunteers. Pharmaceutical Research. 1999;16(9):1412-1416. https://pubmed.ncbi.nlm.nih.gov/10496658/
[8] Thevis M, et al. Metabolism of growth hormone releasing peptides. Rapid Communications in Mass Spectrometry. 2012. https://pubmed.ncbi.nlm.nih.gov/23101768/
Animal Studies:
[9] Johansen PB, Nowak J, Skjaerbaek C, Flyvbjerg A, Andreassen TT, Wilken M, Orskov H. Ipamorelin, a new growth-hormone-releasing peptide, induces longitudinal bone growth in rats. Growth Hormone & IGF Research. 1999;9(2):106-113. https://pubmed.ncbi.nlm.nih.gov/10373343/
[10] Svensson J, Lonn L, Jansson JO, et al. The GH secretagogues ipamorelin and GH-releasing peptide-6 increase bone mineral content in adult female rats. Journal of Endocrinology. 2000;165(3):569-577. https://pubmed.ncbi.nlm.nih.gov/10828840/
[11] Andersen NB, Malmlof K, Johansen PB, Andreassen TT, Ortoft G, Oxlund H. The growth hormone secretagogue ipamorelin counteracts glucocorticoid-induced decrease in bone formation of adult rats. Growth Hormone & IGF Research. 2001;11(5):266-272. https://pubmed.ncbi.nlm.nih.gov/11735243/
[12] Greenwood-Van Meerveld B, Tyler K, Mohammadi E, Pietra C. Efficacy of ipamorelin, a ghrelin mimetic, on gastric dysmotility in a rodent model of postoperative ileus. Journal of Experimental Pharmacology. 2012;4:149-155. https://pmc.ncbi.nlm.nih.gov/articles/PMC4863553/
[13] Aagaard NK, et al. Growth hormone and growth hormone secretagogue effects on nitrogen balance and urea synthesis in steroid-treated rats. Growth Hormone & IGF Research. 2009;19(5):426-431. https://pubmed.ncbi.nlm.nih.gov/19054703/
Additional References:
[14] Fowkes MM, Lalonde T, Yu L, Dhanvantari S, Kovacs MS, Luyt LG. Peptidomimetic growth hormone secretagogue derivatives for positron emission tomography imaging of the ghrelin receptor. European Journal of Medicinal Chemistry. 2018;157:1500-1511.
[15] Svensson J, Lonn L, Jansson JO, et al. Safety and efficacy of ipamorelin in adult patients with GH deficiency. Clinical Endocrinology. 1998. DOI: 10.1046/j.1365-2265.1998.00506.x
Related Peptide Guides
Growth Hormone Axis:
- CJC-1295 - GHRH analog; primary synergistic pairing with ipamorelin
- CJC No DAC / Ipamorelin 5mg Blend - Pre-mixed combination blend
- CJC No DAC / Ipamorelin 10mg Blend - Pre-mixed combination blend (higher concentration)
- Ipamorelin + CJC No DAC 5/5mg - Alternative blend formulation
- Ipamorelin + CJC No DAC 10/10mg - Alternative blend formulation
- Tesamorelin - FDA-approved GHRH analog for visceral fat reduction
- Sermorelin - GHRH analog with long clinical history
- GHRP-2 - Growth hormone releasing peptide (less selective than ipamorelin)
- GHRP-6 - Growth hormone releasing peptide (appetite-stimulating)
- Hexarelin - Potent GHRP with cardioprotective properties
- MK-677 - Oral GH secretagogue (same receptor target)
- IGF-1 LR3 - Downstream growth factor
Recovery and Healing:
- BPC-157 - Body Protection Compound for tissue repair
- TB-500 - Thymosin Beta-4 fragment for recovery
- GHK-Cu - Copper peptide for skin and tissue repair
Sleep and Longevity:
Metabolic:
Need the reconstitution math for Ipamorelin: Complete Research Guide?
Open the calculator with Ipamorelin: Complete Research Guide prefilled to estimate concentration, draw volume, and related measurement math from the reconstitution details you already have.