Semaglutide: Complete Research Guide
On this page
Quick Reference Card
Attribute
Also Known As
- Detail
- Ozempic, Wegovy, Rybelsus, GLP-1 receptor agonist, GLP-1RA
Attribute
Administration
- Detail
- Injectable (subcutaneous, once weekly) or Oral (daily tablet)
Attribute
Research Status
- Detail
- FDA-approved: Ozempic (type 2 diabetes, 2017), Wegovy (obesity, 2021), Rybelsus (type 2 diabetes, oral, 2019)
Attribute
Typical Dose Range
- Detail
- 0.25 to 2.4 mg once weekly (subcutaneous); 3, 7, or 14 mg daily (oral)
Attribute
Half-Life
- Detail
- Approximately 7 days (165-184 hours)
Attribute
Cycle Length
- Detail
- Continuous use; no cycling required
Attribute
Storage
- Detail
- Lyophilized: -20C or colder. Reconstituted: 2-8C (35.6-46.4F), use within 28 days. Pre-filled pens: 2-8C until first use, then room temperature up to 56 days.
Overview / What Is Semaglutide?
The Basics
Semaglutide is the medication that brought GLP-1 agonists into the mainstream. Approved in 2017 for type 2 diabetes and then in 2021 for weight management, it remains the most prescribed and most studied drug in its class. In clinical trials, people on the full dose lost an average of about 15% of their body weight over 68 weeks. For someone weighing 220 pounds, that translates to roughly 33 pounds.
The drug works by mimicking a natural hormone your gut releases after eating. This hormone, GLP-1, tells your brain that food has arrived, slows stomach emptying so you feel satisfied longer, and coordinates insulin and blood sugar responses. Semaglutide amplifies and extends this signal from minutes to about a week, making once-weekly dosing possible.
What distinguishes semaglutide from newer competitors like tirzepatide (which targets two receptors) and retatrutide (which targets three) is that it works through a single receptor. This means it relies entirely on appetite suppression and gastric slowing. It cannot directly signal fat cells to burn fuel. All fat loss is indirect, driven by eating less rather than by reprogramming metabolism.
Where semaglutide wins: it has the longest safety track record of any modern incretin drug, the strongest cardiovascular outcomes data, the widest insurance coverage, and is the only GLP-1 agonist available as an oral pill (Rybelsus). Where it falls short relative to newer multi-receptor drugs: lower weight loss ceiling and a less favorable body composition ratio during weight loss.
The Science
Semaglutide is a synthetic analog of human GLP-1 (glucagon-like peptide-1), modified for extended action. It was developed by Novo Nordisk and achieves its prolonged half-life through two key structural modifications: an alpha-aminoisobutyric acid (Aib) substitution at position 2 that confers resistance to dipeptidyl peptidase-4 (DPP-4) degradation, and a C-18 fatty diacid conjugation at position 26 (via an ADO-ADO-glutamic acid spacer) that enables reversible non-covalent binding to serum albumin [1].
These modifications extend the plasma half-life to approximately 7 days (165-184 hours), compared to the 1-2 minute half-life of native GLP-1. The molecule retains 94% sequence homology to native human GLP-1(7-37) [2].
As a selective GLP-1 receptor agonist, semaglutide activates GLP-1R at native potency (1.0x) without activity at the GIP receptor or glucagon receptor. This single-receptor profile explains both its efficacy as an appetite suppressant and its limitations in body composition outcomes compared to multi-receptor agonists [3].
The STEP clinical trial program established semaglutide 2.4 mg as a standard of care in obesity pharmacotherapy. STEP-1 demonstrated 14.9% mean body weight reduction versus 2.4% with placebo over 68 weeks (n=1,961, p<0.001) [4]. The SELECT cardiovascular outcomes trial (n=17,604, median 40 months) demonstrated a 20% reduction in major adverse cardiovascular events (MACE) versus placebo in participants with obesity and established cardiovascular disease without requiring diabetes [5].
Molecular Identity
Property
Common Names
- Detail
- Semaglutide, Ozempic, Wegovy, Rybelsus
Property
Molecular Type
- Detail
- Synthetic peptide (31 amino acids, GLP-1 analog)
Property
Molecular Formula
- Detail
- C187H291N45O59
Property
Molecular Weight
- Detail
- 4,113.64 g/mol
Property
CAS Number
- Detail
- 910463-68-2
Property
PubChem CID
- Detail
- 56843331
Property
DrugBank ID
- Detail
- DB13928
Property
Target Receptor
- Detail
- GLP-1R (glucagon-like peptide-1 receptor)
Property
Amino Acid Sequence
- Detail
- Modified GLP-1(7-37); 31 residues with Aib at position 2, Arg at position 34, Lys-26 conjugated to C-18 fatty diacid
Property
Key Structural Features
- Detail
- Aib at position 2 (DPP-4 resistance); C-18 fatty diacid at Lys-26 (albumin binding); Lys-34 to Arg substitution
Property
Half-Life
- Detail
- ~7 days (165-184 hours)
Property
GLP-1R Homology
- Detail
- 94% structural similarity to native human GLP-1
Property
Solubility
- Detail
- DMSO: 5.0 mg/mL (1.22 mM)
Property
Salt Form
- Detail
- Available as free base or sodium salt; lyophilized white powder
Mechanism of Action
The Basics
Your body naturally produces a hormone called GLP-1 after eating. This hormone serves as a messenger between your gut and brain, signaling that food has arrived and coordinating your body's response. Semaglutide is an enhanced version of this hormone, engineered to last about a week instead of a few minutes.
The drug works through three main channels. First, it quiets hunger signals in the brain. People consistently report not just eating less, but thinking about food less. This reduction in "food noise" (the constant mental chatter about what to eat next) is one of the most remarked-upon effects. Second, it slows stomach emptying, so meals keep you feeling satisfied for longer and blood sugar stays more stable after eating. Third, it improves how your pancreas manages insulin and blood sugar, particularly when glucose is elevated.
One important limitation: GLP-1 receptors are not found on fat cells. This means semaglutide cannot directly tell your body to burn fat. Instead, all fat loss comes from the caloric deficit created by eating less. This is why semaglutide's body composition profile (roughly 60% fat loss, 40% lean tissue loss) is less favorable than newer dual-receptor drugs like tirzepatide, which can directly signal fat tissue through the GIP receptor.
The Science
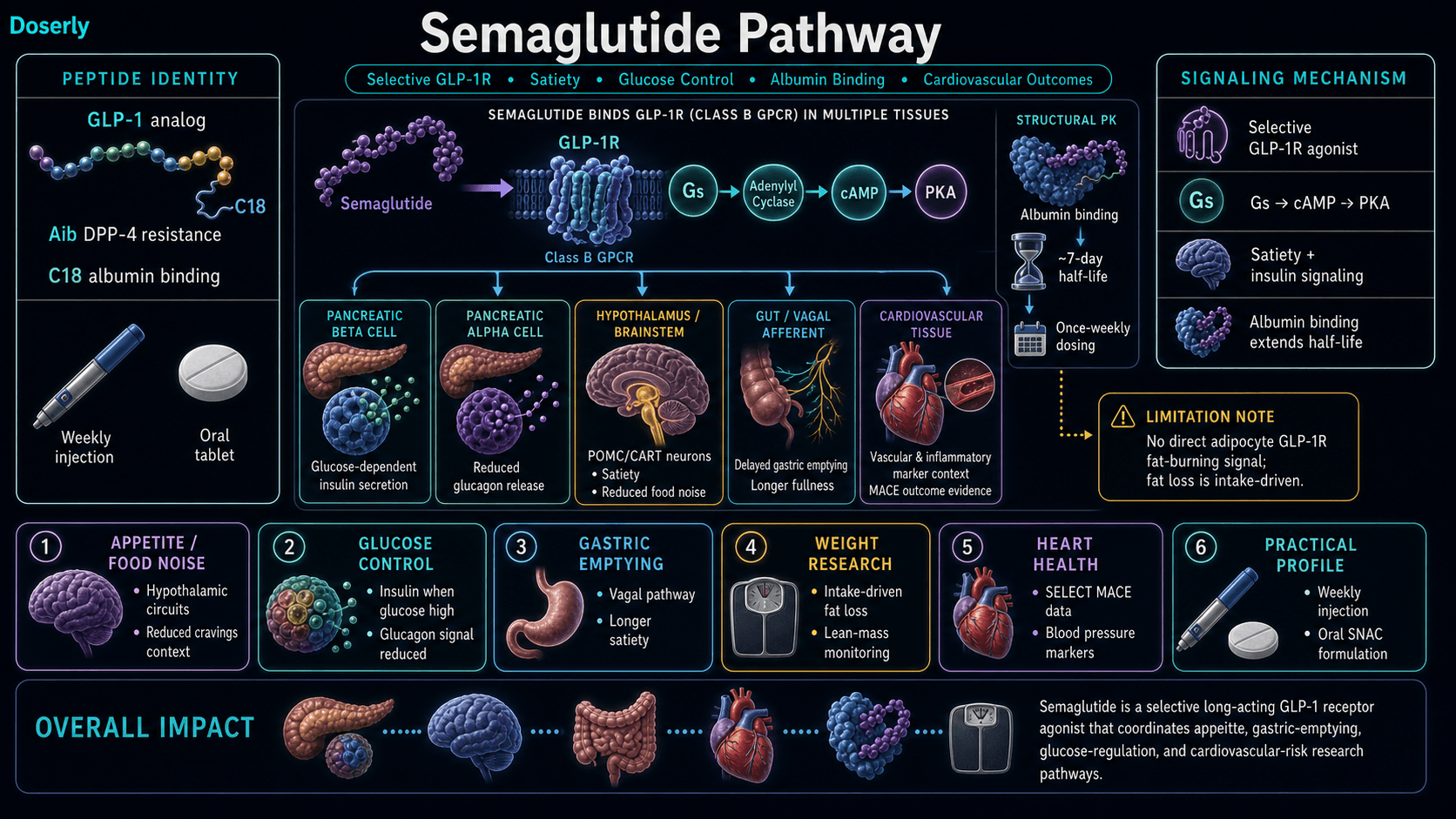
Semaglutide exerts its pharmacological effects through selective agonism of the GLP-1 receptor, a class B G protein-coupled receptor (GPCR) expressed in the pancreas, hypothalamus, brainstem, gastrointestinal tract, and cardiovascular tissues [1][6].
Upon GLP-1R binding, semaglutide activates adenylyl cyclase via Gs alpha subunit coupling, increasing intracellular cyclic AMP (cAMP). This triggers four primary downstream effects:
- Glucose-dependent insulin secretion from pancreatic beta cells, with reduced glucagon release from alpha cells [1]
- Central appetite suppression via activation of hypothalamic POMC/CART neurons in the arcuate nucleus and paraventricular nucleus [6]
- Delayed gastric emptying through vagal afferent signaling, prolonging postprandial satiety [1]
- Improved insulin sensitivity indirectly through weight reduction and decreased ectopic fat deposition [6]
DXA body composition analysis from the STEP-1 substudy revealed a fat-to-lean mass loss ratio of approximately 60:40 in non-diabetic obesity [7]. This ratio is a direct consequence of the absence of GLP-1R expression in adipose tissue. Tirzepatide, which adds GIP receptor agonism with direct signaling to adipocytes via a thermogenic futile calcium cycling mechanism, achieves a 75:25 ratio in comparable populations [8]. Notably, in type 2 diabetes populations, this body composition gap largely disappears due to impaired GIP signaling (the "incretin defect"), with both compounds showing approximately 86:14 ratios in head-to-head comparison [9].
Pathway Visualization Image
Pharmacokinetics
The Basics
Semaglutide stays active in the body for about a week after each injection, which is why once-weekly dosing works. After injection, it reaches peak levels in your blood within 1-3 days, and steady-state concentrations (where levels stabilize from week to week) are typically reached by weeks 4-5 of consistent dosing.
The long duration comes from a clever design feature. A fatty acid chain attached to the peptide grabs onto albumin, a protein that circulates abundantly in your blood. This albumin binding acts like an anchor, preventing the kidneys from clearing the drug quickly and keeping it circulating much longer than the natural hormone it mimics.
Subcutaneous injection provides around 89% bioavailability, meaning most of the injected dose reaches your bloodstream. The oral form (Rybelsus) uses an absorption enhancer called SNAC (salcaprozate sodium) to get across the stomach lining, but oral bioavailability is much lower (approximately 1%), which is why oral doses are measured in milligrams per day rather than milligrams per week.
The Science
Key pharmacokinetic parameters for semaglutide (subcutaneous):
Parameter
Half-life
- Value
- ~168 hours (7 days)
Parameter
Tmax (time to peak)
- Value
- 1-3 days post-injection
Parameter
Time to steady state
- Value
- 4-5 weeks
Parameter
Bioavailability (SC)
- Value
- ~89%
Parameter
Protein binding
- Value
- >99% (primarily albumin)
Parameter
Volume of distribution
- Value
- ~12.5 L
Parameter
Clearance
- Value
- ~0.05 L/h
The extended half-life results from two synergistic modifications: DPP-4 resistance (Aib substitution at position 2) prevents enzymatic degradation, while the C-18 fatty diacid moiety enables reversible non-covalent albumin binding with high affinity (>99% bound) [2]. Metabolism occurs via general proteolysis rather than CYP450-mediated pathways, with the fatty acid side chain undergoing beta-oxidation. Renal clearance of intact semaglutide is minimal [2].
The oral formulation (Rybelsus) employs the absorption enhancer SNAC (salcaprozate sodium) to facilitate gastric epithelial transcellular absorption. Oral bioavailability is approximately 0.4-1%, necessitating substantially higher doses (3-14 mg daily) relative to subcutaneous administration (0.25-2.4 mg weekly) to achieve comparable plasma exposures [10].
Research & Clinical Evidence
Semaglutide and Weight Loss
The Basics
The weight loss evidence for semaglutide is extensive. Across multiple large-scale clinical trials, the drug consistently produces 10-15% average body weight loss at the full 2.4 mg weekly dose. About half of study participants lost 15% or more of their starting weight, and roughly a third reached 20% or beyond. These are averages from structured clinical settings with lifestyle support.
Real-world data from over 18,000 patients tracks closely with trial results. At 3 months on the 2.4 mg dose, average loss is around 5%. By 7 months, most people reach 7-10% total body weight reduction. Non-diabetic individuals tend to lose more than those with type 2 diabetes.
When the drug is stopped, appetite typically returns within 2-4 weeks and weight begins to climb back. The STEP-1 extension study found that participants who stopped semaglutide regained roughly two-thirds of their lost weight within a year, while those who continued maintained their results.
The Science
STEP-1 (n=1,961, 68 weeks): Semaglutide 2.4 mg weekly produced mean body weight reduction of 14.9% vs. 2.4% with placebo (p<0.001). Achievement of clinically meaningful thresholds: ≥5% loss (86.4% vs. 31.5%), ≥10% loss (69.1% vs. 12.0%), ≥15% loss (50.5% vs. 4.9%), ≥20% loss (32.0% vs. 1.7%) [4].
STEP-2 (n=1,210, 68 weeks, T2D population): Semaglutide 2.4 mg achieved 9.6% mean weight loss vs. 3.4% with placebo, with concurrent HbA1c reduction of -1.6% vs. -0.4% [11].
STEP-5 (n=304, 104 weeks): Extended follow-up demonstrated sustained weight loss of approximately 15% at 2 years, with 77% of participants achieving ≥5% loss and significant improvements in waist circumference (-14 cm) and blood pressure [12].
SURMOUNT-5 (head-to-head vs. tirzepatide, n=751, 72 weeks): At maximum tolerated doses, semaglutide produced 13.7% weight loss vs. tirzepatide's 20.2%, a 47% efficacy gap [8].
Semaglutide and Cardiovascular Health
The Basics
Cardiovascular protection is arguably semaglutide's strongest advantage over newer competitors. The SELECT trial, one of the largest cardiovascular outcome studies ever conducted with a weight loss medication, followed over 17,600 people with obesity and heart disease for an average of 40 months. The results showed a 20% reduction in heart attacks, strokes, and cardiovascular death compared to placebo.
This is superiority data against placebo, meaning it proved semaglutide was actively protective, not just safe. Neither tirzepatide nor retatrutide has achieved this standard yet. For people whose primary concern is heart health rather than maximum weight loss, semaglutide currently has the strongest evidence base.
The Science
SELECT trial (n=17,604, median 40 months follow-up): Semaglutide 2.4 mg demonstrated a 20% reduction in three-point MACE (cardiovascular death, nonfatal myocardial infarction, nonfatal stroke) vs. placebo (HR 0.80, 95% CI 0.72-0.90, p<0.001) in participants with overweight/obesity and established cardiovascular disease without T2D [5].
SUSTAIN-6 (n=3,297, 104 weeks, T2D population): Earlier cardiovascular outcomes data showed a 26% reduction in composite MACE in type 2 diabetes patients [13].
Semaglutide and Type 2 Diabetes
The Basics
Semaglutide was first approved for managing blood sugar in type 2 diabetes. At the diabetes dose (typically 1 mg weekly), it improves HbA1c by approximately 1.5-1.9 percentage points and produces about 6% weight loss over a year. The blood sugar control comes from a combination of enhanced insulin release when glucose is high, reduced glucagon production, and the weight loss itself improving insulin sensitivity.
The Science
SUSTAIN-8 (52 weeks, T2D): Semaglutide 1 mg weekly demonstrated HbA1c reductions of 1.5-1.9% and approximately 6% body weight reduction [14]. At the higher 2.4 mg dose in diabetic populations (STEP-2), weight loss reaches approximately 10% with HbA1c reduction of 1.6% [11].
The diminished weight loss in T2D populations (10% vs. 15% in non-diabetic) follows the pattern observed across all incretin therapies, though semaglutide's gap is less dramatic than tirzepatide's because semaglutide does not depend on GIP signaling, which is impaired in T2D [9].
Biomarker Evidence Matrix
Categories are scored only where meaningful data exists. Evidence Strength reflects clinical/research data quality. Reported Effectiveness reflects community sentiment data.
Category
Fat Loss
- Evidence Strength
- 9/10
- Reported Effectiveness
- 9/10
- Summary
- Strong RCT data (STEP program): 14.9% mean weight loss at 2.4mg over 68 weeks. Community reports consistently confirm substantial fat reduction.
Category
Weight Management
- Evidence Strength
- 8/10
- Reported Effectiveness
- 7/10
- Summary
- Effective during active use; STEP-5 confirms 2-year maintenance. Community reports weight regain upon stopping (two-thirds regained within 1 year).
Category
Appetite & Satiety
- Evidence Strength
- 9/10
- Reported Effectiveness
- 9/10
- Summary
- Defining mechanism of action. Clinical and community data overwhelmingly confirm dramatic appetite suppression across doses.
Category
Food Noise
- Evidence Strength
- 6/10
- Reported Effectiveness
- 9/10
- Summary
- Limited formal clinical endpoints, but community reports are among the most emotionally intense of any category. Reduction in intrusive food thoughts is near-universal in user reports.
Category
Energy Levels
- Evidence Strength
- 4/10
- Reported Effectiveness
- 5/10
- Summary
- Mixed. Fatigue common during titration (5-10% of users). Some report improved energy after weight loss. Net effect neutral to mildly negative.
Category
Sleep Quality
- Evidence Strength
- 3/10
- Reported Effectiveness
- 6/10
- Summary
- Limited direct evidence. Sleep apnea resolution after weight loss is documented. Not a primary outcome measure.
Category
Mood & Wellbeing
- Evidence Strength
- 4/10
- Reported Effectiveness
- 7/10
- Summary
- No dedicated mood RCTs for semaglutide. Community reports range from "depression completely gone" to emotional flattening. Confounded with weight loss.
Category
Joint Health
- Evidence Strength
- 5/10
- Reported Effectiveness
- 7/10
- Summary
- Indirect benefit from weight loss reducing mechanical load. Consistent community reports of improved joint pain. STEP-3 OA sub-study data pending.
Category
Inflammation
- Evidence Strength
- 5/10
- Reported Effectiveness
- 7/10
- Summary
- GLP-1 agonists demonstrate anti-inflammatory properties in preclinical models. Community reports reduced inflammation markers, fibromyalgia improvement.
Category
Gut Health
- Evidence Strength
- 3/10
- Reported Effectiveness
- 4/10
- Summary
- Slowed gastric emptying is disruptive to normal GI function. Rare reports of IBS symptom improvement.
Category
Digestive Comfort
- Evidence Strength
- 7/10
- Reported Effectiveness
- 3/10
- Summary
- Well-documented GI side effect profile: constipation 15%, diarrhea 15%, bloating common. Improves with time for most but intolerable for some.
Category
Nausea & GI Tolerance
- Evidence Strength
- 8/10
- Reported Effectiveness
- 3/10
- Summary
- Nausea reported by 33-44% in trials. Most common reason for discontinuation. Dose-dependent, typically improves over 2-4 weeks with slow titration.
Category
Hair Health
- Evidence Strength
- 3/10
- Reported Effectiveness
- 3/10
- Summary
- Hair thinning associated with rapid weight loss and caloric deficit, not semaglutide specifically. Temporary for most.
Category
Heart Health
- Evidence Strength
- 9/10
- Reported Effectiveness
- 8/10
- Summary
- SELECT trial: 20% MACE reduction vs. placebo. Strongest CV outcomes data of any incretin. Community reports confirm BP and metabolic improvements.
Category
Blood Pressure
- Evidence Strength
- 8/10
- Reported Effectiveness
- 8/10
- Summary
- STEP trials demonstrated significant BP reductions. Community reports hypertension resolution after weight loss.
Category
Cravings & Impulse Control
- Evidence Strength
- 4/10
- Reported Effectiveness
- 8/10
- Summary
- Emerging clinical investigation (alcohol, nicotine). Strong community signal: reduced alcohol desire, binge eating cessation, improved impulse control.
Category
Side Effect Burden
- Evidence Strength
- 8/10
- Reported Effectiveness
- 4/10
- Summary
- Well-characterized GI-dominant side effect profile. 63% of Drugs.com reviewers rate positively overall despite side effects.
Category
Treatment Adherence
- Evidence Strength
- 7/10
- Reported Effectiveness
- 7/10
- Summary
- Once-weekly dosing praised for convenience. Primary adherence barriers are cost and GI side effects during titration.
Category
Withdrawal Symptoms
- Evidence Strength
- 5/10
- Reported Effectiveness
- 3/10
- Summary
- Not traditional withdrawal, but appetite rebound and weight regain upon stopping are consistent. STEP-1 extension data confirms regain.
Benefits & Potential Effects
The Basics
Semaglutide's benefits center on three areas: weight loss, blood sugar management, and cardiovascular protection.
For weight loss, the drug reduces appetite and food preoccupation, making it naturally easier to eat less without the constant battle against hunger. Most people notice appetite changes within the first week or two, with steady weight loss becoming apparent from about week four onward. The full dose produces average losses of 10-15% of body weight over about a year.
Beyond the scale, the metabolic improvements can be significant. Blood pressure often normalizes. Blood sugar and HbA1c levels improve. Markers of inflammation may decrease. Joint pain often eases as the mechanical load on joints drops. Many users report that the psychological relief from food noise elimination is at least as valuable as the physical weight loss.
One of the more surprising community-reported benefits is reduced cravings for alcohol and other reward-seeking behaviors. While clinical research into these effects is still early, the signal from patient reports is consistent enough that formal studies are now underway.
The Science
Primary documented benefits:
- Weight reduction: 14.9% mean body weight loss at 2.4 mg over 68 weeks (STEP-1) [4]. Sustained at 104 weeks (STEP-5) [12].
- Glycemic control: HbA1c reduction of 1.5-1.9% at 1 mg; up to 1.6% at 2.4 mg in T2D [11][14].
- Cardiovascular risk reduction: 20% MACE reduction in SELECT (HR 0.80, p<0.001) [5]. 26% MACE reduction in SUSTAIN-6 (T2D) [13].
- Blood pressure improvement: Significant reductions in systolic and diastolic BP observed across STEP trials [4].
- Metabolic improvements: Improved lipid profiles, reduced waist circumference (-14 cm, STEP-5), improved fasting glucose [12].
Emerging areas under investigation:
- Addiction modulation: Preclinical evidence suggests GLP-1R agonism modulates central GABA neurotransmission, with translational implications for alcohol and substance use disorders [15]. Formal clinical trials are underway.
- Neuroprotection: Investigational use in Alzheimer's disease based on central GLP-1R expression in hippocampal and cortical regions [6].
- Non-alcoholic steatohepatitis (NASH): GLP-1R agonists demonstrate hepatoprotective effects in early clinical studies [6].
Side Effects & Safety Considerations
The Basics
The most common side effects are gastrointestinal: nausea, constipation, diarrhea, vomiting, and abdominal discomfort. These affect a significant number of people (roughly 30-40% experience nausea at some point) but are typically worst during the first few weeks or after a dose increase, and most people find they settle down with time.
The key to managing GI side effects is patience with titration. The standard schedule increases the dose every 4 weeks, and many experienced users recommend extending each step to 6 or even 8 weeks if side effects are bothersome. Eating smaller meals, prioritizing protein over fatty foods, staying well-hydrated, and timing injections in the evening are commonly reported strategies.
Less common but important effects include fatigue (affecting roughly 5-10% of users), headaches in the first few weeks, acid reflux, and temporary hair thinning related to rapid weight loss rather than the drug itself.
Rare but serious concerns include pancreatitis (less than 1%), gallbladder problems (1-3%, driven by rapid weight loss rather than the drug directly), and a theoretical thyroid cancer risk based on rodent studies. No confirmed human thyroid cancer cases have been linked to semaglutide, but it is contraindicated for people with a personal or family history of medullary thyroid carcinoma or MEN2 syndrome.
The Science
Common adverse events (STEP-1 incidence):
Side Effect
Nausea
- Incidence
- 44.2%
- Typical Duration
- 2-4 weeks, improves with adaptation
Side Effect
Diarrhea
- Incidence
- 30.0%
- Typical Duration
- 1-2 weeks
Side Effect
Vomiting
- Incidence
- 24.8%
- Typical Duration
- 2-3 weeks
Side Effect
Constipation
- Incidence
- 24.0%
- Typical Duration
- May persist; responds to fiber and hydration
Side Effect
Abdominal pain
- Incidence
- 19.6%
- Typical Duration
- 1-2 weeks
Side Effect
Headache
- Incidence
- ~6.6%
- Typical Duration
- 1-2 weeks
Side Effect
Fatigue
- Incidence
- ~5.4%
- Typical Duration
- Variable
Serious adverse events:
- Pancreatitis: Incidence <1%. Discontinue if severe abdominal pain occurs. Monitor lipase/amylase if symptomatic [1][4].
- Gallbladder disease: 1-3% incidence, primarily gallstones related to rapid weight loss. Risk increases with greater magnitude of weight reduction [16].
- Thyroid C-cell tumors: Observed in rodents at clinically irrelevant doses. No confirmed human cases. Post hoc analyses have not confirmed the association. Contraindicated in MEN2 or personal/family history of medullary thyroid carcinoma [1].
- Acute kidney injury: Rare, typically secondary to dehydration from GI fluid losses [4].
- Non-arteritic anterior ischemic optic neuropathy (NAION): Very rare case reports of irreversible vision loss; causality not established [17].
Contraindications:
- Personal or family history of medullary thyroid carcinoma or MEN2 syndrome
- Pregnancy (discontinue at least 2 months before planned conception)
- Severe gastroparesis or active severe gastrointestinal disease
- History of pancreatitis (use with caution)
The side effects and contraindications above give you a map of what to watch for. Doserly turns that map into a daily practice. Log the specific biomarkers and symptoms associated with this compound's known risk profile, and the app builds a timeline of how your body is responding across your cycle.
Trending in the wrong direction on a key marker? Noticing a pattern that started two weeks into your protocol? Doserly connects the dots between your protocol timeline and your logged data, making it easier to spot emerging issues early and have informed, data-backed conversations with your healthcare provider about what's working and what needs attention.
Keep side effects, flags, and follow-up notes visible.
Doserly helps you document safety observations, side effects, medication changes, and follow-up questions so important context is not scattered.
Safety log
Flags and notes

Safety notes are not emergency guidance; seek medical help when appropriate.
Dosing Protocols
The Basics
Semaglutide uses a gradual dose escalation schedule, starting low and increasing every four weeks. This titration exists to manage GI side effects; rushing it is the most common mistake people make. Not everyone needs or benefits from reaching the highest dose. Many find adequate appetite control and weight loss at intermediate steps.
The standard injectable titration moves through five steps: 0.25 mg for the first four weeks, then 0.5 mg, then 1.0 mg, then 1.7 mg, and finally 2.4 mg at maintenance. Each step lasts at least four weeks, with many practitioners recommending longer stays at each level if side effects are present. Some people find their effective dose at 0.5 or 1.0 mg and stay there indefinitely.
For the oral form (Rybelsus), daily doses follow their own schedule: 3 mg for 30 days, then 7 mg, with an option to increase to 14 mg. The oral tablet must be taken on an empty stomach with no more than 4 ounces of water, at least 30 minutes before any food or other medication.
Once at a maintenance dose, semaglutide is used continuously without cycling. Stopping typically leads to appetite return and weight regain within weeks to months.
The Science
Standard subcutaneous titration (FDA-approved schedule):
Phase
Titration 1
- Weekly Dose
- 0.25 mg
- Duration
- 4 weeks
- Purpose
- Establish tolerance
Phase
Titration 2
- Weekly Dose
- 0.50 mg
- Duration
- 4 weeks
- Purpose
- Early appetite control
Phase
Titration 3
- Weekly Dose
- 1.0 mg
- Duration
- 4+ weeks
- Purpose
- Therapeutic range entry
Phase
Titration 4
- Weekly Dose
- 1.7 mg
- Duration
- 4+ weeks
- Purpose
- Approach maintenance (Wegovy step)
Phase
Maintenance
- Weekly Dose
- 2.4 mg
- Duration
- Ongoing
- Purpose
- Full obesity-indication dose
Reconstitution (research-grade vials):
Vial Size
5 mg
- BAC Water
- 2.0 mL
- Concentration
- 2.5 mg/mL
- 0.25 mg Dose
- 10 units (0.10 mL)
Vial Size
10 mg
- BAC Water
- 3.0 mL
- Concentration
- 3.33 mg/mL
- 0.25 mg Dose
- 7.5 units (0.075 mL)
Vial Size
20 mg
- BAC Water
- 3.0 mL
- Concentration
- 6.67 mg/mL
- 0.25 mg Dose
- 4 units (0.04 mL)
Dosing frequency is once weekly for subcutaneous injection, administered on the same day each week at any time of day, with or without food. Missed doses may be administered within 5 days of the scheduled day; if more than 5 days have elapsed, skip to the next scheduled dose [2].
Consistency is the difference between a protocol that delivers results and one that wastes time and money. Doserly was built for exactly this: keeping you on track with the precision your protocol demands.
The built-in calculators handle the math you shouldn't be doing in your head. The reconstitution calculator tells you exactly how much bacteriostatic water to add for your target concentration. The dose calculator converts between units, milligrams, and syringe markings so you draw the right amount every time. The injection site heat map tracks where you've administered and when, helping you rotate sites systematically to reduce tissue damage, scarring, and absorption inconsistencies from overusing the same area. Pair that with smart reminders tuned to your protocol's timing requirements, and you build the kind of daily consistency that separates optimized protocols from haphazard ones.
Build reminders around the routine, not just the compound.
Doserly can keep timing, skipped doses, and schedule changes organized so the plan you read about becomes easier to follow and review.
Today view
Upcoming reminders

Reminder tracking supports consistency; it does not select a protocol for you.
What to Expect
The following timeline reflects commonly reported experiences from clinical trials and community reports. Individual responses vary significantly based on dose, starting weight, metabolic health, and adherence to lifestyle modifications.
Weeks 1-4 (0.25 mg):
Appetite changes are typically the first noticeable effect, often within the first few days. Meals feel more satisfying with smaller portions. Food noise (constant mental preoccupation with food) may begin to quiet. GI side effects, if they occur, are usually mild at this dose. Some people experience fatigue or mild headaches. Weight loss at this stage is modest (1-3 pounds), partially water weight.
Weeks 5-8 (0.5 mg):
Appetite suppression becomes more pronounced. Many people notice a clear shift in their relationship with food: less snacking, smaller portions feeling adequate, reduced cravings. GI side effects may temporarily increase with the dose step. Weight loss becomes more consistent. Some users report reduced interest in alcohol.
Weeks 9-16 (1.0-1.7 mg):
This is typically where steady, visible weight loss accelerates. Energy levels may begin improving as weight drops. Blood pressure and blood sugar markers often start showing measurable improvement. GI side effects generally stabilize or resolve for most people. Body changes become visible to others.
Weeks 17+ (2.4 mg maintenance):
Weight loss continues at a slower but steady pace. Average total loss of 10-15% body weight is typically reached between months 6 and 12. Metabolic markers (HbA1c, lipids, blood pressure) continue improving. Long-term adherence and lifestyle habits become the primary determinants of ongoing results.
Plateau management:
Weight loss stalls are common and expected. Most practitioners recommend evaluating diet, exercise, and sleep quality before considering a dose increase. Plateaus lasting 2-3 weeks are normal fluctuations; plateaus beyond 4-6 weeks at an effective dose may warrant clinical reassessment.
Interaction Compatibility
Good With (Synergistic)
- NAD+: May help mitigate energy crashes and promote fat oxidation during GLP-1 therapy.
- MOTS-C: Mitochondrial peptide that supports metabolic homeostasis and may promote fat-as-fuel metabolism alongside GLP-1-mediated caloric deficit.
- AOD-9604: Growth hormone fragment that may provide marginal additional lipolytic support for stubborn fat areas, though clinical effect is modest.
- Tesamorelin: GHRH analog that supports GH-mediated lean mass preservation during rapid weight loss. Commonly discussed as a foundation for body composition optimization during GLP-1 therapy.
- BPC-157: Gastric-origin peptide with gut-healing properties that some practitioners explore alongside GLP-1 therapy for GI tolerance. Evidence is preclinical.
Not Good With (Caution Required)
- Other GLP-1 receptor agonists (tirzepatide, retatrutide, survodutide, orforglipron, cagrilintide): Do not combine multiple incretin therapies. Additive GI side effects and potential for hypoglycemia.
- Insulin or sulfonylureas: Increased hypoglycemia risk when combined. Requires careful dose adjustment and monitoring.
- Oral contraceptives and narrow-therapeutic-index medications: Slowed gastric emptying may alter absorption kinetics. Timing adjustments may be needed.
- Thyroid medications (levothyroxine): Delayed gastric emptying may reduce absorption. Separate dosing by at least 30 minutes and monitor thyroid function.
Administration Guide
Materials typically required:
- Pre-filled pen (Ozempic/Wegovy) OR reconstituted vial with U-100 insulin syringes (29-31 gauge)
- Alcohol swabs
- Sharps container for used needles
Reconstitution (vial formulation):
Bacteriostatic water is the standard reconstitution solution. Inject slowly down the vial wall, swirl gently (never shake), and refrigerate immediately after preparation.
Timing considerations:
Semaglutide may be administered at any time of day, with or without food. Many users prefer evening administration to sleep through any initial GI effects. Consistency of day and approximate time is more important than the specific time chosen. Injections should remain at least 48 hours apart if the day needs to change.
Post-administration care:
Allow the injection site to rest; do not massage. Monitor for injection site reactions (redness, swelling), which are generally mild and transient. Stay well-hydrated, especially in the hours following injection. Report persistent vomiting (unable to keep fluids for 24+ hours) or severe abdominal pain to a healthcare provider immediately.
Supplies & Planning
Common materials associated with semaglutide use:
- Pre-filled pens: Ozempic pens (0.25 mg, 0.5 mg, 1 mg, 2 mg) or Wegovy pens (0.25 mg through 2.4 mg) come ready to use with built-in needles
- Research vials: Available in 5 mg, 10 mg, and 20 mg sizes. Require reconstitution with bacteriostatic water
- Insulin syringes: U-100, 29-31 gauge, 1 mL capacity (for vial formulations)
- Bacteriostatic water: 10 mL bottles; approximately 2-3 mL used per vial depending on vial size
- Alcohol swabs: For cleaning vial stoppers and injection sites
- Sharps container: FDA-approved disposal container for used needles and syringes
Specific quantities depend on prescribed dose, titration schedule, and planned protocol duration. Consult with a healthcare provider for individualized planning and use the reconstitution calculator for preparation math.
Storage & Handling
Pre-filled pens (Ozempic/Wegovy):
- Before first use: Refrigerate at 2-8C (36-46F). Good until expiration date.
- After first use: May be kept at room temperature (up to 30C/86F) for up to 56 days.
- Never freeze.
- Protect from direct heat and light.
Lyophilized powder (research vials):
- Optimal long-term storage: -20C (-4F) or colder; stable for up to 2-3 years.
- Short-term storage: Refrigeration at 2-8C is acceptable for weeks to months.
- Keep sealed with desiccant to minimize moisture exposure.
- Allow vials to reach room temperature (10-30 minutes) before opening to prevent condensation.
Reconstituted solution:
- Refrigerate immediately at 2-8C after preparation.
- Use within 28 days.
- Do not freeze reconstituted solutions.
- Inspect for discoloration, cloudiness, or particulate matter before each use. Discard if any abnormalities are observed.
- The benzyl alcohol in bacteriostatic water provides antimicrobial preservation, but solutions should still be discarded after the 28-day window.
Lifestyle Factors
Semaglutide's effects are significantly influenced by lifestyle choices. The drug creates an opportunity for change, but the magnitude and sustainability of results depend heavily on what accompanies it.
Protein intake: This is the single most important dietary factor during GLP-1 therapy. The caloric deficit created by appetite suppression puts lean mass at risk. Most practitioners and researchers recommend 1.0-1.6 g of protein per kilogram of body weight (or per pound of goal weight) distributed across 4-5 meals. Eating protein first at each meal, before fullness from slowed gastric emptying sets in, helps hit targets when appetite is suppressed.
Resistance training: Without structured resistance exercise, approximately 40% of weight lost on semaglutide is lean tissue. Adding resistance training 2-4 times per week provides a stimulus for muscle preservation. Combined with adequate protein, this can meaningfully shift the body composition ratio.
Aerobic exercise: At least 150 minutes per week of moderate activity supports metabolic health, cardiovascular fitness, and the benefits semaglutide provides. Walking 8,000+ steps daily is a commonly recommended starting point.
Hydration: Staying well-hydrated (8-10 glasses of water daily, more during physical activity) is important for general health and specifically helps manage GI side effects like constipation and nausea.
Sleep: 7-9 hours of quality sleep per night supports metabolic health, reduces cortisol-driven hunger cues, and optimizes the body's response to the drug. Poor sleep undermines weight loss independently of medication use.
Stress management: Chronic stress elevates cortisol, which promotes abdominal fat storage and increases appetite. Stress management practices complement the appetite-suppressing effects of semaglutide.
Alcohol: Most users report significantly reduced alcohol tolerance while on semaglutide. Slowed gastric emptying means alcohol stays in the system longer, and reduced food intake means a less-buffered stomach. Starting with much less than usual and gauging response is commonly advised.
Peptide protocols don't exist in a vacuum. Your nutrition, exercise, sleep, stress, and the rest of your health stack all influence outcomes. Doserly tracks your entire health picture in one place: peptides, supplements, medications, TRT/HRT, and the lifestyle factors that determine whether your protocol reaches its potential.
This holistic view reveals correlations that compartmentalized tracking misses. You might discover that your recovery improvements stall during weeks with poor sleep, or that adding a specific supplement amplified a benefit you were already seeing. Doserly's cross-category visibility helps you understand which lifestyle factors are pulling the most weight in your results, turning health optimization from guesswork into a data-informed practice.
Keep sensitive protocol records in a purpose-built app.
Doserly is designed for private health tracking with structured records, offline-ready workflows, and exportable history when you need it.
Privacy
Health records

Privacy controls help you manage records; keep clinical records where required.
Regulatory Status & Research Classification
United States (FDA):
- Ozempic (0.5 mg, 1 mg, 2 mg pens): Approved December 2017 for type 2 diabetes mellitus
- Rybelsus (3, 7, 14 mg tablets): Approved September 2019 for type 2 diabetes (first oral GLP-1 agonist)
- Wegovy (0.25-2.4 mg pens): Approved June 2021 for chronic weight management in adults with obesity (BMI ≥30) or overweight (BMI ≥27) with at least one weight-related comorbidity
- Compounded semaglutide is not FDA-approved
- Active clinical trials: SELECT (completed), STEP program (multiple trials completed), ongoing investigations in NASH, Alzheimer's, addiction
European Union (EMA):
- Ozempic: Authorized February 2018
- Rybelsus: Authorized April 2020
- Wegovy: Authorized January 2022
United Kingdom (MHRA):
- Ozempic, Rybelsus, and Wegovy all authorized for the same indications as above
Canada (Health Canada):
- Ozempic: Approved January 2018
- Rybelsus: Approved 2020
- Wegovy: Approved November 2021
Australia (TGA):
- Ozempic: Registered. Listed on the PBS for type 2 diabetes
- Wegovy: TGA registration obtained 2023
WADA status: Not prohibited. Semaglutide is not on the World Anti-Doping Agency prohibited list.
Regulatory status changes frequently. Always verify the current legal status of any compound in your specific country or jurisdiction before making any decisions.
FAQ
How much weight can I expect to lose on semaglutide?
Based on the STEP-1 clinical trial (the pivotal study), participants on the full 2.4 mg weekly dose lost an average of about 15% of their starting body weight over 68 weeks. Real-world results vary depending on adherence, lifestyle factors, starting weight, and individual biology. About half of trial participants lost 15% or more, and roughly a third lost 20% or more.
Is semaglutide the same as Ozempic and Wegovy?
Ozempic, Wegovy, and Rybelsus all contain semaglutide as the active ingredient. The difference is in dosing, packaging, and FDA-approved indications. Ozempic is approved for type 2 diabetes (max dose 2 mg), Wegovy is approved for weight management (max dose 2.4 mg), and Rybelsus is an oral formulation for type 2 diabetes (max dose 14 mg daily).
What are the most common side effects?
Gastrointestinal issues are the most frequently reported: nausea (affecting approximately a third of users), constipation, diarrhea, and vomiting. These are typically most noticeable during dose increases and tend to improve over 2-4 weeks as the body adapts. Slow titration, smaller meals, and adequate hydration are the most commonly cited management strategies.
Does semaglutide need to be cycled?
Available data and standard clinical practice indicate that semaglutide is designed for continuous, long-term use without cycling. Stopping the drug typically leads to appetite return within 2-4 weeks and significant weight regain within 6-12 months according to extension trial data.
Can semaglutide help with alcohol or other cravings?
Emerging clinical and community evidence suggests GLP-1 receptor agonists may modulate reward-seeking behavior beyond food. Community reports of reduced alcohol desire are consistent and relatively common. Formal clinical trials investigating semaglutide's effects on alcohol use disorder are currently underway, though no approved indication exists for this use.
What happens if I miss a dose?
According to prescribing information, if fewer than 5 days have passed since the missed dose, it should be administered as soon as possible. If more than 5 days have passed, the dose should be skipped and the next dose taken on the regular schedule. Doses should remain at least 48 hours apart.
What is "food noise" and does semaglutide help?
Food noise refers to persistent, intrusive thoughts about food: planning meals, fighting cravings, thinking about snacks in the next room. Community reports overwhelmingly describe significant reduction or elimination of food noise as one of the most life-changing effects of semaglutide, often noticed within the first week of treatment.
How do I manage nausea on semaglutide?
Commonly reported strategies include extending the time at each dose level before increasing, eating smaller and more frequent meals, prioritizing protein and avoiding fatty or greasy foods, staying well-hydrated, taking the injection in the evening, and using ginger supplements. Healthcare providers may also prescribe anti-nausea medications for severe cases.
Sources & References
[1] Dhillon S. "Semaglutide: First Global Approval." Drugs. 2018;78(2):275-284. PMID: 29363040.
[2] Mayo Clinic. "Semaglutide (Subcutaneous Route): Proper Use." Available at: https://www.mayoclinic.org/drugs-supplements/semaglutide-subcutaneous-route/proper-use/drg-20406730
[3] Coskun T, et al. "LY3437943, a novel triple glucagon, GIP, and GLP-1 receptor agonist for glycemic control and weight loss." Cell Metab. 2022;34(9):1234-1247. PMID: 36070752. (Comparative receptor pharmacology context.)
[4] Wilding JPH, et al. "Once-Weekly Semaglutide in Adults with Overweight or Obesity." N Engl J Med. 2021;384(11):989-1002. PMID: 33567185.
[5] Lincoff AM, Brown-Frandsen K, et al. "Semaglutide and Cardiovascular Outcomes in Obesity without Diabetes." N Engl J Med. 2023;389(24):2221-2232. PMID: 37952131.
[6] NCBI Bookshelf. "Semaglutide." StatPearls. Available at: https://www.ncbi.nlm.nih.gov/books/NBK576406/
[7] STEP-1 DXA body-composition substudy. Published in PMC as supplementary analysis to STEP-1.
[8] Aronne LJ, et al. "Tirzepatide vs Semaglutide Once Weekly in Patients with Obesity." N Engl J Med. 2024. (SURMOUNT-5 trial.)
[9] Tirzepatide vs Semaglutide Clamp Study. Head-to-head body composition comparison in T2D population, 28 weeks.
[10] EMA Assessment Report: Rybelsus (semaglutide oral tablets). European Medicines Agency, 2020.
[11] Davies M, et al. "Semaglutide 2.4 mg once a week in adults with overweight or obesity, and type 2 diabetes (STEP 2)." Lancet. 2021;397(10278):971-984.
[12] Garvey WT, et al. "Two-year effects of semaglutide in adults with overweight or obesity: the STEP 5 trial." Nat Med. 2022;28(10):2083-2091.
[13] Marso SP, et al. "Semaglutide and Cardiovascular Outcomes in Patients with Type 2 Diabetes." N Engl J Med. 2016;375(19):1834-1844. PMID: 27633186. (SUSTAIN-6.)
[14] Lingvay I, et al. "Superior HbA1c reduction with semaglutide versus canagliflozin." SUSTAIN-8 trial. Published in Diabetes Obes Metab. 2019.
[15] Sirohi S, et al. "The glucagon-like peptide-1 (GLP-1) analogue semaglutide reduces alcohol drinking and modulates central GABA neurotransmission." JCI Insight. 2023. PMID: 37192005.
[16] Faillie JL. "GLP-1 receptor agonists and gallbladder/biliary disease risk: Meta-analysis." JAMA Intern Med. Published data on gallstone incidence with GLP-1 therapy.
[17] FDA Safety Communication on GLP-1 receptor agonists and NAION risk. Post-marketing surveillance report.
Related Peptide Guides
- Tirzepatide — Dual GLP-1/GIP agonist with stronger weight loss and body composition data. The most direct comparison to semaglutide.
- Retatrutide — Investigational triple GLP-1/GIP/glucagon agonist with the highest weight loss data to date.
- Orforglipron — Non-peptide oral GLP-1 agonist in development, a potential next-generation oral alternative.
- Survodutide — Dual GLP-1/glucagon agonist with strong liver fat reduction data.
- Cagrilintide — Amylin analog explored in combination with semaglutide (CagriSema).
- Mazdutide — Dual GLP-1/glucagon agonist in development.
- NAD+ — Cellular energy support commonly discussed alongside GLP-1 therapy.
- MOTS-C — Mitochondrial-derived peptide for metabolic support.
- AOD-9604 — Growth hormone fragment for targeted fat loss.
- Tesamorelin — GHRH analog for lean mass preservation during weight loss.
- BPC-157 — Gastric peptide explored for GI support during GLP-1 therapy.
- Tesofensine — Triple monoamine reuptake inhibitor for weight loss; alternative mechanism of action.
Need the reconstitution math for Semaglutide: Complete Research Guide?
Open the calculator with Semaglutide: Complete Research Guide prefilled to estimate concentration, draw volume, and related measurement math from the reconstitution details you already have.