Retatrutide: Complete Research Guide
On this page
Quick Reference Card
Attribute
Also Known As
- Detail
- LY3437943, LY-3437943, Triple GLP-1/GIP/glucagon receptor agonist, Incretin triple agonist
Attribute
Administration
- Detail
- Injectable (subcutaneous, once weekly)
Attribute
Research Status
- Detail
- Investigational. Phase 3 clinical trials (TRIUMPH program) ongoing. Not FDA-approved for any indication.
Attribute
Typical Dose Range
- Detail
- 1-12 mg once weekly (gradual titration over 12-24 weeks)
Attribute
Half-Life
- Detail
- Approximately 6 days (~144 hours)
Attribute
Cycle Length
- Detail
- Continuous use; clinical trials ran 36-68 weeks
Attribute
Storage
- Detail
- Lyophilized: -20C or colder (stable up to 24 months). Reconstituted: 2-8C, use within 4 weeks.
Overview / What Is Retatrutide?
The Basics
Retatrutide is an investigational weight loss peptide developed by Eli Lilly that has generated significant attention for producing the largest average weight loss of any obesity medication studied to date. In clinical trials, participants on the highest dose lost an average of 24.2% of their body weight over 48 weeks (Phase 2) and 28.7% over 68 weeks (Phase 3). For someone weighing 250 pounds, that translates to roughly 60-70 pounds lost in about a year.
What makes retatrutide different from existing weight loss drugs is that it works on three metabolic pathways simultaneously instead of one or two. Semaglutide (Ozempic, Wegovy) targets one pathway. Tirzepatide (Mounjaro, Zepbound) targets two. Retatrutide targets all three: appetite suppression, metabolic efficiency, and direct fat burning from the liver. This triple action is why the weight loss numbers surpass anything previously seen in clinical trials.
The compound is given as a once-weekly injection and is currently being evaluated in the TRIUMPH Phase 3 trial program for obesity, obstructive sleep apnea, and knee osteoarthritis. FDA approval is not expected before 2027.
The Science
Retatrutide (LY3437943) is a 39-amino acid synthetic peptide engineered as a balanced triagonist with activity at three metabolic receptors: the glucagon-like peptide-1 receptor (GLP-1R), glucose-dependent insulinotropic polypeptide receptor (GIPR), and glucagon receptor (GCGR) [1]. It was discovered by Eli Lilly and first described in preclinical characterization by Coskun et al. in Cell Metabolism (2022) [2].
The peptide features a C20 fatty acid (eicosanoic acid) modification conjugated to lysine-16 via an AEEA spacer and gamma-glutamate linker, enabling albumin binding that extends the pharmacokinetic half-life to approximately 6 days [2]. Additional modifications include 2-aminoisobutyric acid (Aib) substitutions at positions 2 and 20 for DPP-4 resistance, and 2-methylleucine at position 13 for enhanced receptor selectivity.
Receptor potency profiling reveals that retatrutide is most potent at GIPR (EC50 0.0643 nM), with moderate GLP-1R activity (EC50 0.775 nM) and lower GCGR activity (EC50 5.79 nM) [2]. Relative to native hormone potencies, this translates to approximately 2x native GIP activity, 0.5x native GLP-1 activity, and 0.2x native glucagon activity. This receptor balance was specifically designed to overcome the "incretin defect" observed in type 2 diabetes, where impaired GIP signaling blunts the efficacy of dual GLP-1/GIP agonists like tirzepatide [1][2].
The Phase 2 dose-ranging trial (N=338) demonstrated mean body weight reductions of 24.2% at the 12 mg dose over 48 weeks, with 100% of participants on 8-12 mg achieving at least 5% weight loss [3]. Phase 3 TRIUMPH-4 topline results (December 2025) confirmed 28.7% average weight loss at 12 mg over 68 weeks [4].
Molecular Identity
Property
Common Names
- Detail
- Retatrutide, LY3437943
Property
Molecular Type
- Detail
- Synthetic peptide (39 amino acids)
Property
Molecular Formula
- Detail
- C221H342N46O68 (free base)
Property
Molecular Weight
- Detail
- 4731.33 g/mol (free base); 4845.35 g/mol (TFA salt)
Property
CAS Number
- Detail
- 2381089-83-2
Property
PubChem CID
- Detail
- 171390338
Property
FDA UNII
- Detail
- NOP2Y096GV
Property
Target Receptors
- Detail
- GLP-1R, GIPR, GCGR
Property
Key Structural Features
- Detail
- C20 diacid lipid conjugation at Lys-16 via AEEA/gamma-Glu linker; Aib at positions 2 and 20; alpha-methylleucine at position 13; C-terminal serinamide
Property
Solubility
- Detail
- Water: 5 mg/mL; DMSO: 50 mg/mL; PBS pH 7.2: 1-10 mg/mL
Property
Salt Form
- Detail
- Available as free base or trifluoroacetate (TFA) salt; white to off-white lyophilized powder
Mechanism of Action
The Basics
Your body has three key hormonal systems that control how you process food and manage energy. Retatrutide activates all three at once, which is why it produces stronger effects than drugs that only target one or two.
The first system is GLP-1, a hormone your gut releases after eating. It tells your brain you are full, slows down digestion so you stay satisfied longer, and helps your pancreas release the right amount of insulin. Semaglutide works entirely through this one pathway. Retatrutide activates it at about half the intensity of semaglutide, which provides meaningful appetite control with somewhat less nausea.
The second system is GIP, another gut hormone that improves how your body handles nutrients, particularly how well insulin works and how fat cells function. Tirzepatide added this pathway on top of GLP-1, and it helped explain why its weight loss exceeded semaglutide. Retatrutide pushes GIP activation to twice the level of tirzepatide, specifically because GIP signaling becomes impaired in people with type 2 diabetes. The stronger signal was engineered to push through that impairment.
The third system, and the one unique to retatrutide, is glucagon. While GLP-1 and GIP reduce how much you eat, glucagon tells your liver to burn stored fat for energy. Think of it as adding a furnace to the equation: GLP-1 and GIP close the input valve (less food in), while glucagon opens the output valve (more fat burned). The combination attacks obesity from both sides simultaneously.
The trade-off with glucagon activation is that it can increase heart rate slightly and is associated with benign heart rhythm changes in some people. This is why cardiac monitoring is emphasized more with retatrutide than with other GLP-1 drugs.
The Science
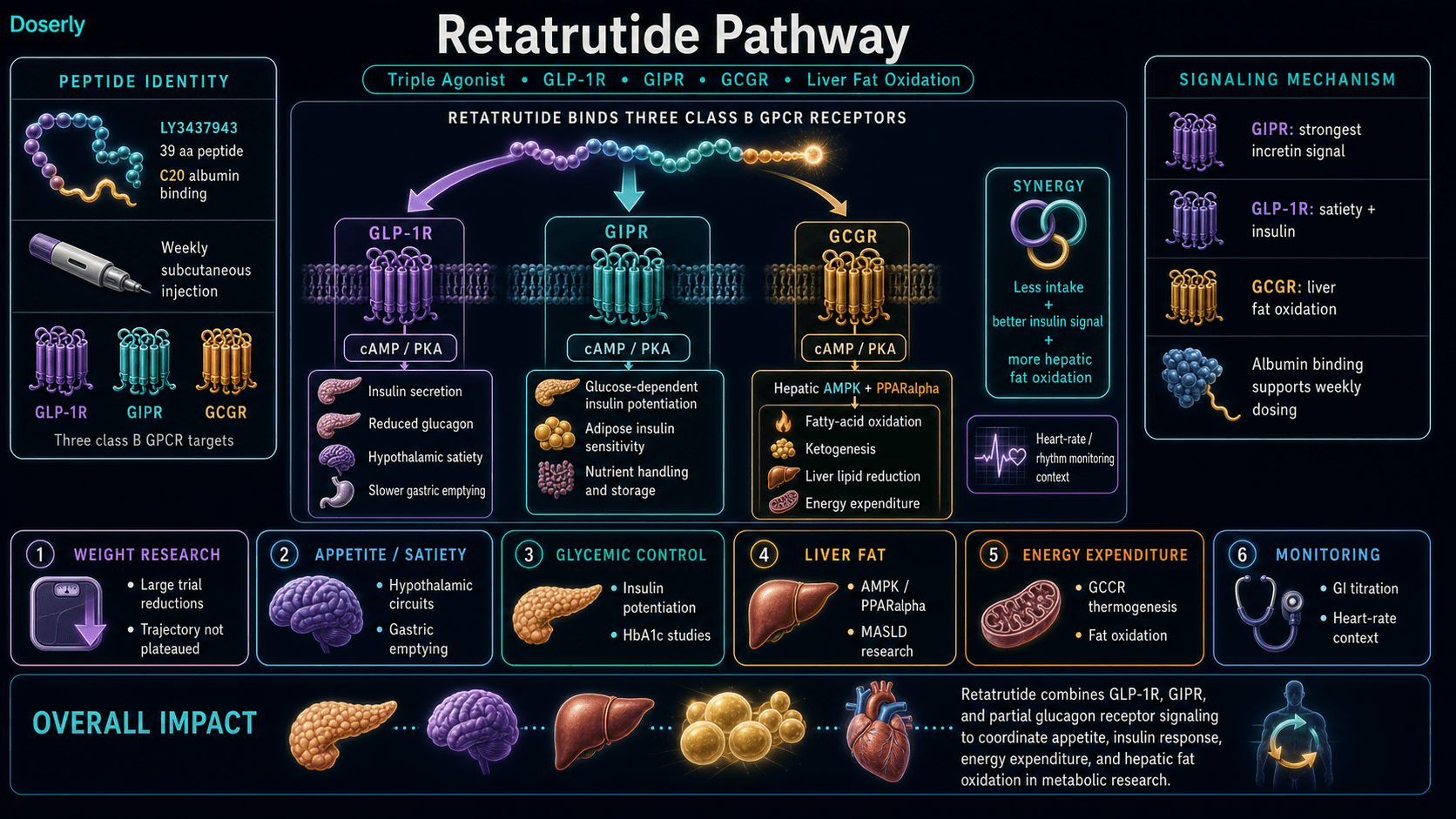
Retatrutide exerts its metabolic effects through simultaneous agonism of three G protein-coupled receptors:
GLP-1R agonism (0.5x native potency): Activation of GLP-1 receptors on pancreatic beta cells triggers cAMP/PKA pathway-mediated glucose-dependent insulin secretion, while suppressing glucagon release from alpha cells [1]. Central nervous system effects include activation of hypothalamic satiety circuits via direct action on paraventricular and arcuate nucleus neurons, contributing to reduced caloric intake [5]. Peripheral effects include delayed gastric emptying through vagal afferent pathways [1].
GIPR agonism (2.0x native potency): Retatrutide exhibits the strongest GIP signal of any approved or investigational incretin therapy [2]. GIPR activation synergistically potentiates glucose-dependent insulin secretion, improves adipose tissue insulin sensitivity, and modulates adipose tissue metabolism through enhanced lipid uptake and storage in appropriate depots [6]. The 2x native potency was specifically engineered to overcome the "incretin defect" characteristic of type 2 diabetes, where impaired GIP receptor signaling blunts the weight-loss advantages of dual GLP-1/GIP agonists [2].
GCGR agonism (0.2x native potency): Partial glucagon receptor activation, unique among obesity therapeutics, stimulates hepatic glycogenolysis, ketogenesis, and lipid oxidation through AMPK and PPARalpha pathway activation [2][7]. The partial agonism (approximately 20% of native glucagon activity) provides sufficient thermogenic and lipolytic drive to increase basal metabolic rate without inducing the hyperglycemia associated with full glucagon receptor activation [7]. This mechanism directly drives liver fat oxidation, explaining the dramatic hepatic steatosis reduction (approximately 86% in Phase 2 MASLD cohorts) that exceeds anything achievable through weight loss alone [8].
The net physiological result is synergistic: GLP-1 and GIP coordinate to reduce caloric intake and improve insulin sensitivity, while glucagon increases energy expenditure and fat oxidation. This three-pronged approach produces greater weight loss and metabolic improvement than any single or dual-agonist therapy [1][3].
Pathway Visualization Image
Pharmacokinetics
The Basics
Retatrutide is designed as a long-acting peptide that stays active in your body for about 6 days after each injection. This is why it only needs to be given once per week. After injection, it binds to a protein called albumin in your bloodstream, which acts as a carrier that slowly releases the peptide over several days. This sustained release helps maintain consistent drug levels throughout the week.
It takes approximately 3-4 weeks of regular weekly dosing to reach steady-state levels, meaning the amount in your body stabilizes at a consistent level. Because of this slow buildup, the effects of retatrutide accumulate gradually over time, which is one reason why clinical trials use a titration approach (starting low and slowly increasing the dose over weeks).
After being released from albumin, retatrutide is primarily cleared through the liver without involvement of the cytochrome P450 enzyme system. This is important because it means retatrutide is less likely to interact with other medications that are processed through liver enzymes.
The Science
Key pharmacokinetic parameters for retatrutide based on Phase 1 and Phase 2 clinical data [2][9]:
- Route of administration: Subcutaneous injection
- Half-life (t1/2): Approximately 6 days (144 hours)
- Time to steady state: Approximately 3.9 weeks with regular weekly dosing
- Mechanism of extended half-life: C20 fatty diacid modification enables reversible albumin binding, creating a circulating depot that resists renal clearance due to the large molecular weight of the albumin-peptide complex (approximately 69 kDa)
- Metabolism: Primarily hepatic clearance through proteolytic degradation; no cytochrome P450 involvement
- Dose proportionality: Exposure increases proportionally across the 1-12 mg dose range in Phase 2 studies [3]
- Bioavailability: Approximately 100% from subcutaneous depot (peptide is fully absorbed from the injection site)
The prolonged half-life differentiates retatrutide from earlier peptide therapeutics and supports once-weekly dosing. Similar albumin-binding strategies are employed by semaglutide (C18 fatty acid) and tirzepatide (C20 fatty acid), though retatrutide's specific linker chemistry (AEEA spacer with gamma-glutamate) differs from both [2].
Research & Clinical Evidence
Obesity (Phase 2 Trial)
The Basics
The study that put retatrutide on the map was a Phase 2 clinical trial published in the New England Journal of Medicine in June 2023. It enrolled 338 adults with obesity (BMI 30 or higher) or overweight with at least one weight-related health condition, and followed them for 48 weeks. Importantly, people with diabetes were excluded from this trial.
The results were striking. At the highest dose (12 mg weekly), participants lost an average of 24.2% of their body weight, roughly 58 pounds. At 8 mg, the loss was 22.8%. Even at 4 mg, participants lost 17% or more. By contrast, the placebo group lost only about 2%.
What particularly stands out is the response rate: 100% of participants on 8-12 mg lost at least 5% of their body weight, and 83% on 12 mg lost at least 15%. These numbers exceed anything seen with semaglutide (roughly 15% average) or tirzepatide (roughly 21% average) in their respective trials.
The Science
The Phase 2 dose-ranging trial (NCT04881760) was a double-blind, randomized, placebo-controlled study of 338 adults with BMI >=30 or BMI 27-30 with comorbidities (excluding diabetes) [3]. Participants were randomized to retatrutide at 1, 4, 8, or 12 mg weekly or placebo, with 4 mg and 8 mg groups further divided by starting dose (2 mg vs. 4 mg).
Primary endpoint: percent change in body weight from baseline to 24 weeks. Key efficacy results at 48 weeks:
Dose
Placebo
- Mean weight loss (48 wk)
- -2.1%
- Achieved >=5% loss
- 27%
- Achieved >=15% loss
- 4%
Dose
1 mg
- Mean weight loss (48 wk)
- -8.7%
- Achieved >=5% loss
- 64%
- Achieved >=15% loss
- 14%
Dose
4 mg
- Mean weight loss (48 wk)
- -16.3 to -17.8%
- Achieved >=5% loss
- 87-91%
- Achieved >=15% loss
- 55-63%
Dose
8 mg
- Mean weight loss (48 wk)
- -22.1 to -22.8%
- Achieved >=5% loss
- 100%
- Achieved >=15% loss
- 75-83%
Dose
12 mg
- Mean weight loss (48 wk)
- -24.2%
- Achieved >=5% loss
- 100%
- Achieved >=15% loss
- 83%
The weight loss trajectory had not plateaued at 48 weeks, suggesting continued efficacy with longer treatment duration [3]. Phase 3 TRIUMPH-4 data subsequently confirmed 28.7% weight loss at 12 mg over 68 weeks [4].
Type 2 Diabetes (Phase 2 Trial)
The Basics
A separate Phase 2 trial tested retatrutide specifically in 281 adults with type 2 diabetes. Over 36 weeks, the highest dose group achieved approximately 17% weight loss and dramatic improvements in blood sugar control, with HbA1c dropping by about 2 percentage points. Approximately 82% of participants on higher doses reached an HbA1c below 6.5%, which is essentially a normal blood sugar level.
These results are lower than the obesity trial (17% vs. 24%) because type 2 diabetes impairs the GIP signaling pathway that retatrutide relies on. Every incretin drug shows reduced weight loss in diabetic populations, but retatrutide's gap was narrower than expected, suggesting the stronger GIP signal and the glucagon pathway may partially compensate for this impairment.
The Science
The Phase 2 trial in type 2 diabetes (Rosenstock et al., Lancet 2023) enrolled 281 adults and evaluated retatrutide at 0.5-12 mg weekly versus placebo and dulaglutide over 36 weeks [6]. At the 12 mg dose, HbA1c was reduced by -2.02 percentage points versus -0.01% for placebo. Weight loss at 12 mg reached 16.94%, substantially exceeding dulaglutide's 2.02%.
Body composition data from the DXA substudy (Lancet Diabetes & Endocrinology, 2025, N=189) showed a fat-to-lean loss ratio of approximately 63:37, with absolute fat mass reductions of up to 26% at the 8 mg dose [10]. While this ratio is less favorable than tirzepatide's 75:25 in non-diabetic obesity trials, the comparison is confounded by the different populations (T2D vs. non-diabetic), different durations (36 vs. 72 weeks), and the known effect of the incretin defect on GIP-mediated body composition advantages [10].
Liver Fat and MASLD
The Basics
Perhaps the most impressive data for retatrutide involves liver fat. In a substudy of participants with metabolic dysfunction-associated steatotic liver disease (MASLD, formerly called fatty liver disease), retatrutide reduced liver fat by approximately 86%. To put that in context, semaglutide reduces liver fat by about 30%, and tirzepatide by about 47%. The glucagon receptor component drives this difference because it directly tells the liver to burn stored fat, rather than relying on the indirect effects of overall weight loss.
This is significant because fatty liver disease affects roughly 25-30% of adults globally and is a growing driver of liver cirrhosis and liver cancer. A treatment that could reverse the condition this dramatically would address a massive unmet medical need.
The Science
The Phase 2 MASLD substudy (Nature Medicine, 2024) demonstrated approximately 86% reduction in hepatic fat fraction in participants receiving retatrutide at higher doses [8]. This substantially exceeds reductions observed with semaglutide (~30% in Phase 2 NAFLD trials) and tirzepatide (~47% in the SYNERGY-NASH Phase 2 study).
The mechanistic basis for this advantage is retatrutide's glucagon receptor agonism. GCGR activation stimulates hepatic fatty acid oxidation through AMPK and PPARalpha pathways, enhances ketogenesis, and reduces de novo lipogenesis [7][8]. These direct hepatic effects operate independently of and additively to the weight-loss-mediated improvements in liver fat that all incretin therapies provide.
Resolution of hepatic steatosis was observed in approximately 85% of participants in the higher dose groups [8]. The TRIUMPH Phase 3 program includes dedicated MASLD endpoints that will provide larger-scale confirmation.
Phase 3 Results (TRIUMPH Program)
The Basics
In December 2025, Eli Lilly released topline results from the TRIUMPH-4 Phase 3 trial. The numbers exceeded even the strong Phase 2 showing: participants on the 12 mg dose lost an average of 28.7% of their body weight over 68 weeks, roughly 71 pounds for a 250-pound person. The 9 mg dose produced 26.4% loss. Beyond weight, the TRIUMPH program is also evaluating retatrutide for obstructive sleep apnea (where excess weight is a primary driver) and knee osteoarthritis (where the Phase 3 data showed 75.8% knee pain reduction) [4][11].
The Science
TRIUMPH-4 (NCT05929066) is the pivotal Phase 3 obesity trial. Topline results at 68 weeks showed mean body weight reduction of 28.7% at 12 mg and 26.4% at 9 mg [4]. Full publication of the data, including safety, body composition, and cardiometabolic endpoints, is pending.
Additional TRIUMPH program components include:
- TRIUMPH-3: Retatrutide in type 2 diabetes with obesity
- TRIUMPH-5: Retatrutide for obstructive sleep apnea
- TRIUMPH-6: Retatrutide for knee osteoarthritis
- NCT06383390: Effect on cardiovascular and kidney outcomes [11]
Biomarker Evidence Matrix
Category
Fat Loss
- Evidence Strength
- 10/10
- Reported Effectiveness
- 9/10
- Summary
- Phase 2 and Phase 3 RCTs demonstrate 24-29% average weight loss. Strongest clinical evidence in obesity pharmacotherapy.
Category
Weight Management
- Evidence Strength
- 10/10
- Reported Effectiveness
- 9/10
- Summary
- 100% of 8-12mg participants achieved >=5% weight loss. Phase 3 data confirms sustained trajectory through 68 weeks.
Category
Appetite & Satiety
- Evidence Strength
- 9/10
- Reported Effectiveness
- 8/10
- Summary
- GLP-1-mediated appetite suppression well-documented in RCTs. 80%+ report decreased appetite.
Category
Food Noise
- Evidence Strength
- 6/10
- Reported Effectiveness
- 8/10
- Summary
- Consistent with GLP-1 class effects. Community reports strong but direct RCT evidence for food noise as a discrete outcome is limited.
Category
Energy Levels
- Evidence Strength
- 5/10
- Reported Effectiveness
- 6/10
- Summary
- Glucagon receptor activation theoretically increases energy expenditure. Mixed reports: improved energy from metabolic effects vs. fatigue from caloric deficit.
Category
Nausea & GI Tolerance
- Evidence Strength
- 9/10
- Reported Effectiveness
- 3/10
- Summary
- GI side effects thoroughly documented in RCTs (nausea 18-45%, diarrhea 15-33%). Community reports confirm significant burden during titration.
Category
Digestive Comfort
- Evidence Strength
- 8/10
- Reported Effectiveness
- 3/10
- Summary
- Bloating, reflux, constipation well-documented during dose escalation. Improves over time for most.
Category
Heart Rate & Palpitations
- Evidence Strength
- 8/10
- Reported Effectiveness
- 3/10
- Summary
- Dose-dependent HR increases (+2-7 bpm) and benign arrhythmias (4-14% vs. 2-3% placebo) documented in Phase 2. Unique to retatrutide among incretins.
Category
Heart Health
- Evidence Strength
- 7/10
- Reported Effectiveness
- 6/10
- Summary
- Cardiometabolic improvements (BP, lipids, visceral fat) countered by cardiac signal. Long-term CV outcome trial ongoing.
Category
Blood Pressure
- Evidence Strength
- 8/10
- Reported Effectiveness
- 7/10
- Summary
- Significant BP reductions in Phase 2; 41-71% of higher-dose patients discontinued BP medications.
Category
Cravings & Impulse Control
- Evidence Strength
- 5/10
- Reported Effectiveness
- 7/10
- Summary
- GLP-1 class effect on reward pathways well-established. Retatrutide-specific data limited. Community reports positive.
Category
Muscle Growth
- Evidence Strength
- 7/10
- Reported Effectiveness
- 5/10
- Summary
- DXA data shows 63:37 fat:lean ratio in T2D. No non-diabetic body composition data yet. Active mitigation (resistance training, protein) needed.
Category
Side Effect Burden
- Evidence Strength
- 9/10
- Reported Effectiveness
- 4/10
- Summary
- Thoroughly documented. GI effects dominate but are manageable with slow titration. 6-8% discontinuation in Phase 2.
Category
Treatment Adherence
- Evidence Strength
- 7/10
- Reported Effectiveness
- 6/10
- Summary
- Once-weekly dosing is convenient. 12-18% discontinuation in Phase 3 suggests moderate adherence challenges.
Category
Gut Health
- Evidence Strength
- 4/10
- Reported Effectiveness
- 4/10
- Summary
- Limited data. GLP-1 class affects gut motility. Gallbladder stress is a class concern.
Category
Physical Performance
- Evidence Strength
- 4/10
- Reported Effectiveness
- 5/10
- Summary
- Insufficient direct evidence. Metabolic rate increase may support performance, but caloric deficit during aggressive weight loss may impair it.
Category
Mood & Wellbeing
- Evidence Strength
- 4/10
- Reported Effectiveness
- 6/10
- Summary
- Indirect evidence from weight loss benefits. No retatrutide-specific mood studies.
Category
Body Image
- Evidence Strength
- 3/10
- Reported Effectiveness
- 7/10
- Summary
- Inferred from substantial weight loss outcomes. Concerns about loose skin with rapid loss.
Categories scored: 18
Categories with community data: 18
Categories not scored (insufficient data): Sleep Quality, Focus & Mental Clarity, Memory & Cognition, Anxiety, Stress Tolerance, Motivation & Drive, Emotional Aliveness, Emotional Regulation, Libido, Sexual Function, Joint Health, Inflammation, Pain Management, Recovery & Healing, Skin Health, Hair Health, Hormonal Symptoms, Temperature Regulation, Fluid Retention, Immune Function, Bone Health, Longevity & Neuroprotection, Social Connection, Withdrawal Symptoms, Daily Functioning
Benefits & Potential Effects
The Basics
The primary benefit of retatrutide is substantial weight loss that surpasses any currently available medication. In clinical trials, the average person lost roughly a quarter of their body weight, with some individuals losing 30% or more. The weight loss comes with a cascade of metabolic improvements: better blood sugar control, lower blood pressure, improved cholesterol levels, and dramatic reductions in liver fat.
Beyond the headline weight loss numbers, several specific benefits stand out. For people with pre-diabetes, 72% of trial participants reverted to normal blood sugar levels. For those taking blood pressure medications, up to 71% in higher-dose groups were able to stop at least one medication. Liver fat, measured directly through imaging, was reduced by approximately 86% in patients with fatty liver disease.
The glucagon component provides a benefit that other GLP-1 drugs lack: it actively increases metabolic rate, meaning your body burns more calories even at rest. This "burn from both sides" effect (eating less AND burning more) is why the weight loss numbers exceed what semaglutide and tirzepatide achieve.
It is important to note that retatrutide remains investigational. These benefits have been observed in controlled clinical trial settings and may not translate identically to real-world use.
The Science
Documented clinical benefits from Phase 2 and Phase 3 data include:
Weight and body composition:
- Mean body weight reduction of 24.2% at 48 weeks (Phase 2, 12 mg) [3] and 28.7% at 68 weeks (Phase 3, 12 mg) [4]
- 100% responder rate for >=5% weight loss at 8-12 mg [3]
- Fat mass reduction up to 26% (DXA, 8 mg, T2D substudy) [10]
Glycemic control:
- HbA1c reduction of up to 2.02 percentage points (T2D trial, 12 mg) [6]
- 82% of T2D participants reached HbA1c <=6.5% [6]
- 72% reversion from pre-diabetes to normoglycemia (obesity trial) [3]
Hepatic effects:
- Approximately 86% reduction in hepatic fat fraction (MASLD cohort) [8]
- Resolution of hepatic steatosis in approximately 85% of participants [8]
Cardiometabolic:
- Significant reductions in systolic and diastolic blood pressure [3]
- Improvements in LDL cholesterol, triglycerides, and waist circumference [3]
- 41-71% of participants on higher doses discontinued at least one antihypertensive medication [3]
Renal:
- Improvement in kidney parameters in participants with T2D and/or obesity [6]
- Dedicated cardiovascular and kidney outcomes trial initiated (NCT06383390) [11]
Side Effects & Safety Considerations
The Basics
The side effects of retatrutide follow a pattern similar to other GLP-1 drugs, with gastrointestinal issues being the most common. Nausea, diarrhea, vomiting, and constipation are reported most frequently, particularly during the early weeks when the dose is being increased. These effects are dose-dependent: starting at lower doses and titrating slowly significantly reduces their severity.
What is important to understand is that the starting dose and how quickly you escalate matter enormously. In the Phase 2 trial, participants who started at 4 mg and quickly escalated to 8 mg experienced nausea at roughly 60%, while those who started at 2 mg and escalated more gradually reported nausea at only 17%. This three-fold difference from the same target dose illustrates why slow titration is consistently emphasized by clinicians and experienced community members.
Retatrutide has one safety concern that sets it apart from semaglutide and tirzepatide: a dose-dependent increase in resting heart rate. At lower doses (1-4 mg), the increase is modest at 2-3 beats per minute. At the highest dose (12 mg), it can reach 6-7 bpm. Benign arrhythmias (palpitations, skipped beats) have been observed in 4-14% of trial participants versus 2-3% on placebo. These effects typically appear early, peak, and then partially attenuate over time. No serious cardiac events dominated the published data, but cardiac monitoring is considered essential, particularly for anyone with pre-existing heart conditions.
Other class-related concerns include gallbladder effects, a small risk of pancreatitis, and the consequences of rapid weight loss (nutritional deficiencies, muscle loss, loose skin). These risks are amplified with retatrutide due to its potency.
The Science
Phase 2 adverse event data (48 weeks, all doses combined) [3][12]:
Gastrointestinal (most common):
Side Effect
Nausea
- 4 mg
- 18-27%
- 8 mg
- 17-39%
- 12 mg
- 45%
- Placebo
- 11%
Side Effect
Diarrhea
- 4 mg
- 12-15%
- 8 mg
- 20-23%
- 12 mg
- 15-33%
- Placebo
- 8-11%
Side Effect
Vomiting
- 4 mg
- 8-12%
- 8 mg
- 10-16%
- 12 mg
- 17-19%
- Placebo
- 1-4%
Side Effect
Constipation
- 4 mg
- 10-11%
- 8 mg
- 11-12%
- 12 mg
- 16%
- Placebo
- 3-4%
GI events were primarily mild-to-moderate in severity, concentrated during dose-escalation phases, and resolved with continued treatment [3]. Severe GI adverse events were reported in 6% of the 12 mg group [3]. Starting-dose dependency was pronounced: the 8 mg group starting at 2 mg reported 17% nausea, while the 8 mg group starting at 4 mg reported approximately 60% [3].
Cardiac effects (unique to retatrutide):
- Dose-dependent resting heart rate increase: +2-3 bpm at 1-4 mg, up to +6-7 bpm at 12 mg [1]
- Benign arrhythmias: 4-14% versus 2-3% placebo [1]
- Heart rate increases appeared early, peaked around 24 weeks, then partially attenuated [12]
- No dominant serious cardiac events in published Phase 2 data [3]
- TRIUMPH Phase 3 topline data reported dysesthesia in 8.8% (9 mg) and 20.9% (12 mg) [4]
Other:
- Pancreatitis: reported in 2% of the highest dose group [3]
- Discontinuation due to adverse events: approximately 6-8% across dose groups (Phase 2), 12-18% (Phase 3) [3][4]
- No severe hypoglycemia or serious treatment-related adverse events in Phase 2 [3][6]
The side effects and contraindications above give you a map of what to watch for. Doserly turns that map into a daily practice. Log the specific biomarkers and symptoms associated with this compound's known risk profile, and the app builds a timeline of how your body is responding across your cycle.
Trending in the wrong direction on a key marker? Noticing a pattern that started two weeks into your protocol? Doserly connects the dots between your protocol timeline and your logged data, making it easier to spot emerging issues early and have informed, data-backed conversations with your healthcare provider about what's working and what needs attention.
Keep side effects, flags, and follow-up notes visible.
Doserly helps you document safety observations, side effects, medication changes, and follow-up questions so important context is not scattered.
Safety log
Flags and notes

Safety notes are not emergency guidance; seek medical help when appropriate.
Dosing Protocols
The Basics
Retatrutide is administered as a once-weekly subcutaneous injection. The approach used in clinical trials involves starting at a low dose and gradually increasing it over several months. This titration strategy is critical because it dramatically reduces the gastrointestinal side effects that occur when the body first encounters the drug.
Based on clinical trial protocols, commonly reported dose ranges fall into three general categories:
Conservative approach: Starting at 1-2 mg weekly for weeks 1-4, increasing to 4 mg for weeks 5-8, then 6 mg for weeks 9-12, reaching 8 mg for maintenance. This approach prioritizes tolerability and is associated with lower side effect rates.
Standard approach: Starting at 2 mg for weeks 1-4, increasing to 4 mg (weeks 5-8), 8 mg (weeks 9-12), with an option to maintain at 8 mg or escalate to 12 mg. This mirrors the dose bands used in the Phase 2 trial.
Some community members report using even lower starting doses (0.25-0.5 mg) with slower escalation over longer periods (2-week or monthly increments) to minimize GI discomfort. This ultra-conservative approach is not directly studied in clinical trials but reflects a preference for gradual receptor adaptation.
The 8 mg and 12 mg dose levels produced similar weight loss results in the Phase 2 trial (22.8% vs. 24.2%), a difference of only 1.4 percentage points. This is worth considering because higher doses carry more side effects, particularly the cardiac signal, without a proportional increase in efficacy.
Retatrutide does not require cycling. Clinical trial participants used it continuously for 36-68 weeks. However, post-treatment weight regain has been observed with GLP-1 class drugs, so some form of maintenance dosing may eventually be needed.
The Science
Dosing parameters derived from Phase 2 trial protocol (Jastreboff et al., NEJM 2023) [3]:
Phase
Initiation
- Weeks
- 1-4
- Dose Range
- 1-2 mg
- Notes
- GI and cardiac baseline assessment
Phase
Titration
- Weeks
- 5-12
- Dose Range
- 4-6 mg
- Notes
- 2-4 mg increments every 4 weeks
Phase
Target
- Weeks
- 13-24
- Dose Range
- 8 mg
- Notes
- Significant weight loss, liver fat reduction
Phase
Maintenance
- Weeks
- 25-48+
- Dose Range
- 8-12 mg
- Notes
- Sustained efficacy; 12 mg for maximum effect
Dose-response analysis showed a clear relationship between dose and weight loss, though the incremental benefit diminished at higher doses: 1 mg (8.7%), 4 mg (17%), 8 mg (22.5%), 12 mg (24.2%) [3]. The clinical significance of the 1.7% difference between 8 mg and 12 mg must be weighed against the increased cardiac effects and GI burden at 12 mg.
All doses <=10 mg can be drawn from a single reconstituted 10 mg vial (at 10.0 mg/mL concentration). Doses exceeding 10 mg require preparation from multiple vials, with volumes >1.0 mL split into two separate injections at different sites for optimal absorption [12].
Consistency is the difference between a protocol that delivers results and one that wastes time and money. Doserly was built for exactly this: keeping you on track with the precision your protocol demands.
The built-in calculators handle the math you shouldn't be doing in your head. The reconstitution calculator tells you exactly how much bacteriostatic water to add for your target concentration. The dose calculator converts between units, milligrams, and syringe markings so you draw the right amount every time. The injection site heat map tracks where you've administered and when, helping you rotate sites systematically to reduce tissue damage, scarring, and absorption inconsistencies from overusing the same area. Pair that with smart reminders tuned to your protocol's timing requirements, and you build the kind of daily consistency that separates optimized protocols from haphazard ones.
Build reminders around the routine, not just the compound.
Doserly can keep timing, skipped doses, and schedule changes organized so the plan you read about becomes easier to follow and review.
Today view
Upcoming reminders

Reminder tracking supports consistency; it does not select a protocol for you.
What to Expect
Timelines below are based on clinical trial data and community reports. Individual experiences vary significantly based on dose, titration speed, and individual physiology.
Weeks 1-4 (Initiation Phase):
Most people begin at a low dose (1-2 mg) during this period. Scale results are typically modest, with 2-4% body weight loss that is primarily water weight as the body adjusts to altered gastric motility and fluid balance. GI side effects (nausea, fullness, reduced appetite) are most noticeable during the first 1-2 weeks after each dose increase but tend to diminish with each subsequent dose. Appetite suppression begins during this phase for most people, though some report minimal change until dose escalation.
Weeks 5-12 (Building Phase):
As the dose increases to 4-6 mg, meaningful fat loss begins. Cumulative weight loss typically reaches 8-15% by week 12. Appetite suppression becomes more pronounced, and many report significant reductions in food noise and cravings. GI side effects may briefly return with each dose increase but generally are less severe than the initial experience. Energy levels may fluctuate as the body adapts to the caloric deficit.
Weeks 12-24 (Acceleration Phase):
At 8 mg, this is typically the period of most visible change. Weight loss accelerates, and cumulative loss approaches 15-20%. Liver fat reductions become significant. Blood pressure and metabolic markers begin to show measurable improvement. Community members frequently report this as the phase where others start noticing physical changes. GI side effects have generally stabilized or resolved for most people by this point.
Weeks 24-48 (Sustained Effect):
On a stable maintenance dose (8-12 mg), weight loss continues at a steady pace. The Phase 2 trial showed the curve had not fully plateaued at 48 weeks, reaching 22-24% average loss. Cardiometabolic improvements consolidate: blood pressure, cholesterol, and blood sugar markers show their full effect. For those with fatty liver disease, liver fat continues to decline.
Weeks 48-68+ (Extended Phase):
Phase 3 data extends the trajectory to 28.7% at 68 weeks, confirming that benefits continue with sustained treatment. Whether and how to transition to a maintenance dose (potentially lower) is an active area of research.
Common early adjustments: Community members report that eating smaller, more frequent meals, avoiding high-fat foods, staying well-hydrated, and keeping ginger or anti-nausea medication available significantly ease the transition during the first 8-12 weeks.
The week-by-week expectations above are drawn from research and community reports, but your experience will be uniquely yours. Doserly's biomarker tracking transforms those general timelines into personal data points you can actually see and measure.
Log the specific markers relevant to this compound, whether that's pain levels, energy, sleep quality, body composition, recovery time, or mood, and watch your own trend lines emerge over weeks and months. Did your key markers start shifting in week three, like the research suggests? Is your experience tracking with what the community reports, or diverging? Over time, this creates something more valuable than any guide: an evidence-based picture of how your body responds to this specific compound, at your specific dose, within your specific health context.
Turn symptom and safety notes into a clearer timeline.
Doserly helps you log doses, symptoms, and safety observations side by side so patterns are easier to discuss with a qualified clinician.
Pattern view
Logs and observations
Pattern visibility is informational and should be reviewed with a clinician.
Interaction Compatibility
Potentially Synergistic Compounds
- NAD+: Community and educational sources recommend NAD+ supplementation to support beta-oxidation pathways and prevent energy crashes during caloric deficit. The rationale is that retatrutide's glucagon activation increases fat oxidation demand, which is NAD+-dependent.
- MOTS-C: Mitochondrial peptide that supports fat-as-fuel metabolism and exercise capacity. May complement retatrutide's metabolic effects.
- AOD-9604: Fragment of human growth hormone that targets stubborn fat deposits. Sometimes combined for enhanced localized fat loss.
- Tesamorelin: Growth hormone releasing hormone analog that supports lean mass preservation. Frequently recommended as a foundation for maintaining muscle during aggressive weight loss.
- Ipamorelin: Growth hormone secretagogue for lean mass preservation and recovery support.
- SS-31: Mitochondrial peptide that may support cellular energy production during metabolic stress from caloric restriction.
- Tesofensine: Monoamine reuptake inhibitor that some sources mention as a bridge compound during transitions between GLP-1 drugs.
Not Recommended to Combine With
- Semaglutide: Overlapping GLP-1 receptor agonism creates redundant appetite suppression with compounded GI side effects. No additive benefit.
- Tirzepatide: Overlapping GLP-1 and GIP receptor agonism. Retatrutide already provides both pathways at different potencies.
- Cagrilintide: Amylin analog with appetite-suppressive effects. Potential for excessive appetite suppression and GI burden when combined with a triple agonist.
- Mazdutide: Dual GLP-1/glucagon agonist with overlapping mechanisms.
- Survodutide: Dual GLP-1/glucagon agonist with overlapping mechanisms.
Caution
- Orforglipron: Non-peptide GLP-1 agonist. Same mechanism overlap concerns as semaglutide.
- IGF-1 LR3: Some community sources suggest low-dose retatrutide with IGF-1 LR3 for lean bulking, but the metabolic profiles may conflict.
Administration Guide
Retatrutide is administered via subcutaneous injection once weekly. Based on clinical trial protocols and community practice:
Materials typically required:
- U-100 insulin syringes (1 mL capacity, 29-31 gauge, 5/16" to 1/2" needle)
- Alcohol swabs (70% isopropyl)
- Bacteriostatic water for reconstitution
- Sharps disposal container
Reconstitution solution: Bacteriostatic water (0.9% benzyl alcohol) is the standard reconstitution medium. Common reconstitution volumes are 1.0 mL per 10 mg vial (yielding 10.0 mg/mL) for convenient measurement on insulin syringes where 1 unit equals approximately 100 mcg. Some sources report using 2.0-3.0 mL for larger vials (20-30 mg) to maintain similar concentrations.
Timing considerations: Retatrutide can be administered at any consistent time and day of the week. Some community members prefer evening administration to sleep through any initial nausea. Maintaining the same day each week supports consistent blood levels. No specific fasting or food requirements.
Post-administration care: Monitor for injection site reactions (redness, swelling). During the titration phase, monitor for GI symptoms and keep anti-nausea options available. Track resting heart rate, particularly when escalating to higher doses. Document dose, date, injection site, and any symptoms for reference.
For volumes exceeding 1.0 mL, split the dose into two separate injections at different anatomical sites to ensure proper absorption.
Supplies & Planning
General materials associated with retatrutide protocols:
Peptide vials: Retatrutide is commonly available in 5 mg, 10 mg, 20 mg, and 30 mg vial sizes as a lyophilized powder. Vial selection depends on target dose and duration.
Syringes: U-100 insulin syringes (1 mL capacity) with 29-31 gauge needles. For doses under 10 units, consider 30-unit or 50-unit capacity syringes for improved measurement accuracy.
Reconstitution supplies: Bacteriostatic water (10 mL bottles), separate drawing needles (18-20 gauge) for reconstitution, and alcohol swabs for vial stoppers and injection sites.
Storage containers: Lyophilized vials require freezer storage. Reconstituted vials require refrigeration. An opaque container or foil wrapping protects reconstituted vials from light.
Monitoring equipment: A home blood pressure monitor and pulse oximeter or heart rate tracker are recommended given retatrutide's cardiac effects. A food scale and body composition measurement tools support tracking progress.
Readers should consult their healthcare provider for specific quantities based on their individual protocol. The reconstitution calculator at doserly.com/calculator can help determine preparation volumes for specific vial sizes and target concentrations.
Storage & Handling
Lyophilized (powder) form:
- Optimal long-term storage: -20C (-4F) or colder, stable for up to 24 months
- Short-term storage: Refrigeration at 2-8C (35.6-46.4F) for weeks to months
- Room temperature: Acceptable for brief periods (days) during shipping or preparation, but not recommended for extended storage
- Keep in original sealed packaging with desiccant to minimize moisture exposure
- Store in a dry, dark environment; peptides are hygroscopic and light-sensitive
Reconstituted (liquid) form:
- Refrigerate immediately at 2-8C (35.6-46.4F)
- Use within 4 weeks (28 days) when reconstituted with bacteriostatic water
- Do NOT freeze reconstituted solutions; freezing denatures peptides
- If longer storage is needed: aliquot into sterile single-use vials, freeze at -20C, thaw each aliquot only once
- Allow vials to reach room temperature before opening to prevent condensation inside the vial
Handling best practices:
- Swab vial stopper with alcohol before each draw
- Use a new sterile syringe for each injection
- Inspect reconstituted solution before each use: should be clear and colorless with no cloudiness, particles, or discoloration
- Label vials with reconstitution date
- Dispose of reconstituted vials after 28 days regardless of remaining volume
Lifestyle Factors
Optimizing outcomes with retatrutide involves more than the injection itself. Clinical trial protocols and community experience consistently point to several complementary practices:
Nutrition: A high-protein diet (commonly cited at 1-2 grams per pound of body weight) is widely recommended to preserve lean muscle mass during aggressive weight loss. Nutrient-dense whole foods are preferred over protein supplements to avoid micronutrient deficiencies. Smaller, more frequent meals help manage GI side effects, particularly during dose escalation. Adequate fiber intake supports gut regularity.
Exercise: Resistance training (2-3 times per week) is considered important for maintaining muscle and bone density during weight loss. This is particularly relevant given retatrutide's glucagon component, which is inherently catabolic. Regular aerobic activity (walking, cycling, swimming) maximizes the metabolic rate benefits from glucagon activation. Community sources emphasize that exercise is not optional when using potent weight loss compounds.
Hydration: Adequate water intake (commonly cited at 4-6 liters per day) is important to support kidney function, manage dehydration risk from GI side effects, and support metabolic processes. Monitor for signs of dehydration, especially during episodes of diarrhea or vomiting.
Sleep: Prioritize 7-9 hours of quality sleep. Sleep deprivation impairs insulin sensitivity and hunger hormone regulation, which can counteract the metabolic benefits of retatrutide. Adequate rest supports recovery and hormonal balance.
Monitoring: Regular lab work is recommended, including complete blood count, comprehensive metabolic panel, HbA1c, and lipid panel. For those with liver concerns, liver elastography or ultrasound imaging provides direct assessment of fatty liver progression. Track body weight, waist circumference, and if possible, body composition to ensure fat loss rather than muscle loss. Resting heart rate tracking is particularly important given the cardiac signal.
Mental health: Rapid weight loss can affect body image, social dynamics, and eating patterns. Some community members report emotional adjustment as their relationship with food changes dramatically. Those with a history of eating disorders should work closely with a mental health professional throughout their protocol.
Regulatory Status & Research Classification
United States (FDA):
Retatrutide is classified as an investigational new drug. It has not received FDA approval for any indication as of March 2026. Eli Lilly's Phase 3 TRIUMPH program is actively enrolling across multiple indications:
- TRIUMPH-4: Obesity (NCT05929066)
- TRIUMPH-3: Type 2 diabetes with obesity
- TRIUMPH-5: Obstructive sleep apnea
- TRIUMPH-6: Knee osteoarthritis
- NCT06383390: Cardiovascular and kidney outcomes
Based on the TRIUMPH-4 topline results released in December 2025, an FDA submission is anticipated in 2026, with a potential approval decision in 2027.
Canada (Health Canada):
No regulatory application has been filed. Status will likely follow FDA action.
United Kingdom (MHRA):
No regulatory application has been filed. Retatrutide is not available through the NHS or private prescriptions.
Australia (TGA):
No regulatory application has been filed. Not listed on the Australian Register of Therapeutic Goods.
European Union (EMA):
No marketing authorization application has been filed. Regulatory submission is expected to follow the FDA timeline.
WADA Status:
Peptide hormones including GLP-1 receptor agonists are listed under section S2 (Peptide Hormones, Growth Factors, Related Substances, and Mimetics) of the WADA Prohibited List. Athletes subject to anti-doping testing should verify current status before any use.
Active clinical trials: Multiple trials are registered on ClinicalTrials.gov under the TRIUMPH program. Full listings are available by searching "retatrutide" or "LY3437943" on clinicaltrials.gov.
Regulatory status changes frequently. Always verify the current legal status of any compound in your specific country or jurisdiction before making any decisions.
FAQ
What is retatrutide and how is it different from semaglutide or tirzepatide?
Retatrutide is an investigational triple-receptor agonist that targets GLP-1, GIP, and glucagon receptors simultaneously. Semaglutide targets only GLP-1, and tirzepatide targets GLP-1 and GIP. The addition of the glucagon receptor is what distinguishes retatrutide; it directly tells the liver to burn stored fat, increasing energy expenditure beyond what appetite suppression alone can achieve. This triple mechanism is why retatrutide produces greater average weight loss in clinical trials (24-29%) compared to semaglutide (15%) and tirzepatide (21-22%).
How much weight can you lose on retatrutide?
Based on available clinical trial data, participants on the highest dose (12 mg weekly) lost an average of 24.2% of body weight over 48 weeks in Phase 2 and 28.7% over 68 weeks in Phase 3. For a 250-pound person, that translates to roughly 60-70 pounds. Individual results vary significantly based on starting weight, dose, adherence, diet, exercise, and metabolic factors.
What are the most common side effects?
Gastrointestinal effects are the most frequently reported: nausea (18-45% depending on dose), diarrhea (15-33%), vomiting (8-17%), and constipation (10-16%). These are dose-dependent, most pronounced during dose escalation, and typically improve within 4-8 weeks. Retatrutide also causes dose-dependent heart rate increases (2-7 bpm) and benign arrhythmias in some participants, which is unique among GLP-1 class drugs.
Is retatrutide FDA-approved?
No. As of March 2026, retatrutide is in Phase 3 clinical trials (TRIUMPH program). Based on topline results released in December 2025, an FDA submission is anticipated in 2026, with a potential approval decision in 2027. It is not available through pharmacies or by prescription.
Does retatrutide need to be cycled?
Based on available clinical trial data, retatrutide was used continuously for 36-68 weeks without cycling. Like other GLP-1 agonists, its effects depend on ongoing use; weight regain has been observed upon discontinuation with related compounds. Long-term maintenance strategies are an active area of investigation.
Can retatrutide reduce liver fat?
Yes, this is one of retatrutide's most distinctive benefits. In Phase 2 MASLD substudy data, liver fat was reduced by approximately 86%, with resolution of hepatic steatosis in approximately 85% of participants on higher doses. This substantially exceeds the liver fat reductions observed with semaglutide (~30%) and tirzepatide (~47%). The glucagon receptor component drives direct hepatic fat oxidation.
Does retatrutide affect heart rate?
Yes. Clinical trial data documents a dose-dependent increase in resting heart rate of approximately 2-3 bpm at lower doses (1-4 mg) and up to 6-7 bpm at the highest dose (12 mg). Benign arrhythmias were reported in 4-14% of participants versus 2-3% on placebo. This cardiac signal is unique to retatrutide among the GLP-1 drug class and is attributed to the glucagon receptor component. Monitoring is recommended.
How should retatrutide be stored?
As a lyophilized powder, store at -20C or colder for up to 24 months. After reconstitution with bacteriostatic water, refrigerate at 2-8C and use within 4 weeks. Never freeze reconstituted peptide solutions.
Sources & References
Clinical Trials:
[1] Coskun T, Urva S, Roell WC, et al. "LY3437943, a novel triple GLP-1/GIP/glucagon receptor agonist for glycemic control and weight loss: From discovery to clinical proof of concept." Cell Metabolism. 2022;34(9):1234-1247.e9. DOI: 10.1016/j.cmet.2022.07.002
[2] Coskun T, et al. Retatrutide (LY3437943) receptor pharmacology and preclinical characterization. Cell Metabolism. 2022. DOI: 10.1016/j.cmet.2022.07.002
[3] Jastreboff AM, Kaplan LM, Frias JP, et al. "Triple-Hormone-Receptor Agonist Retatrutide for Obesity: A Phase 2 Trial." New England Journal of Medicine. 2023;389(6):514-526. DOI: 10.1056/NEJMoa2301972. PMID: 37366315
[4] Eli Lilly. TRIUMPH-4 Phase 3 topline results. December 2025. ClinicalTrials.gov: NCT05929066.
Diabetes Trials:
[5] Holst JJ. "The physiology of glucagon-like peptide 1." Physiological Reviews. 2007;87(4):1409-1439.
[6] Rosenstock J, Frias JP, Jastreboff AM, et al. "Retatrutide, a GIP, GLP-1 and Glucagon Receptor Agonist, for People with Type 2 Diabetes: A Randomised, Double-Blind, Placebo and Active-Controlled, Parallel-Group, Phase 2 Trial." Lancet. 2023;402(10401):529-544. DOI: 10.1016/S0140-6736(23)01053-X. PMID: 37385280
Mechanism and Pharmacology:
[7] Finan B, et al. "A rationally designed monomeric peptide triagonist corrects obesity and diabetes in rodents." Nature Medicine. 2015;21(1):27-36.
[8] Loomba R, et al. "Retatrutide and Metabolic Dysfunction-Associated Steatotic Liver Disease." Nature Medicine. 2024. DOI: 10.1038/s41591-024-03018-2. PMC: 11271400
[9] Urva S, et al. "LY3437943, a novel triple GLP-1/GIP/glucagon receptor agonist in patients with type 2 diabetes: a phase 1b, multicentre, double-blind, placebo-controlled, randomised, multiple-ascending-dose trial." Lancet. 2022. DOI: 10.1016/S0140-6736(22)02033-5
Body Composition:
[10] DXA body composition substudy of retatrutide in type 2 diabetes. Lancet Diabetes & Endocrinology. 2025. PMID: 40609566
Additional:
[11] ClinicalTrials.gov. "Effect of Retatrutide on Cardiovascular and Kidney Outcomes." NCT06383390.
[12] Hamza M, et al. "Triple agonism based therapies for obesity." Current Obesity Reports. 2025.
Meta-Analyses:
[13] "Efficacy and Safety of Glucagon-Like Peptide-1 Receptor Agonists: A Systematic Review and Meta-Analysis." PubMed: 39761578.
[14] "Efficacy and Safety of once-weekly subcutaneous retatrutide on weight and metabolic markers: a systematic review and meta-analysis." PubMed: 38843460.
Related Peptide Guides
- Semaglutide - GLP-1 receptor agonist; the established benchmark for incretin-based weight loss
- Tirzepatide - Dual GLP-1/GIP agonist; the current clinical standard for severe obesity
- Mazdutide - Dual GLP-1/glucagon agonist; shares the glucagon mechanism with retatrutide
- Survodutide - Dual GLP-1/glucagon agonist; another triple-mechanism comparator
- Orforglipron - Non-peptide oral GLP-1 agonist; represents the oral alternative approach
- Cagrilintide - Amylin analog; complementary appetite suppression mechanism
- NAD+ - Frequently recommended as a support compound for fat oxidation during GLP-1 therapy
- MOTS-C - Mitochondrial peptide for metabolic support
- AOD-9604 - Growth hormone fragment for fat loss
- Tesamorelin - GHRH analog for lean mass preservation during weight loss
- Ipamorelin - Growth hormone secretagogue commonly combined with metabolic protocols
- Tesofensine - Monoamine reuptake inhibitor mentioned in transition protocols
- IGF-1 LR3 - Growth factor sometimes discussed in lean bulking contexts
- SS-31 - Mitochondrial peptide for cellular energy support
Need the reconstitution math for Retatrutide: Complete Research Guide?
Open the calculator with Retatrutide: Complete Research Guide prefilled to estimate concentration, draw volume, and related measurement math from the reconstitution details you already have.