Follistatin-344: Complete Research Guide
On this page
Quick Reference Card
Attribute
Also Known As
- Detail
- FS-344, FST-344, FS344, Follistatin isoform 344, Activin-Binding Protein, FSH-Suppressing Protein
Attribute
Administration
- Detail
- Injectable (subcutaneous, intramuscular)
Attribute
Research Status
- Detail
- Research compound. Not FDA-approved for any human therapeutic use. Prohibited by WADA since 2019.
Attribute
Typical Dose Range
- Detail
- 100-200 mcg/day subcutaneous (anecdotal; no established clinical standard)
Attribute
Half-Life
- Detail
- ~90 minutes to 2 hours
Attribute
Cycle Length
- Detail
- 10-30 days on, 3-4 weeks off
Attribute
Storage
- Detail
- Lyophilized: -20°C; Reconstituted: 2-8°C, use within 7 days
Overview / What Is Follistatin-344?
The Basics
Your muscles have a built-in governor that limits how big they can get. This governor is a protein called myostatin, and it constantly tells your muscles "that's enough, stop growing." Follistatin-344 is the body's natural tool for silencing that governor. It binds to myostatin and neutralizes it before the signal can reach your muscle cells, effectively removing the cap on muscle growth.
Follistatin-344 is a glycoprotein, a large protein molecule decorated with sugar chains, that your body already produces. The "344" refers to the number of amino acids in the precursor form. Once processed, the mature circulating form (called FS-315) carries a distinctive acidic tail that keeps it circulating in the bloodstream rather than binding to tissue surfaces. This makes FS-315 the systemic, whole-body version of follistatin, as opposed to FS-288 which sticks to specific tissues.
The excitement around this compound comes from animal studies showing dramatic results: mice with elevated follistatin levels developed two to three times their normal muscle mass [1][2]. Primate studies showed sustained muscle growth lasting over 15 months from a single gene therapy treatment [3]. But there is an important caveat. Nearly all of these impressive results come from gene therapy experiments, where the body continuously produces follistatin for months or years. The injectable peptide form has a half-life of roughly 90 minutes, and its effects in humans remain largely anecdotal. The gap between what gene therapy achieves and what short-term peptide injections deliver is one of the widest in the peptide space.
The Science
Follistatin (FST) is a secreted glycoprotein encoded by the FST gene on chromosome 5q11.2. Through alternative mRNA splicing, the gene produces multiple isoforms, with FS-344 representing the full-length 344-amino acid preprotein. Following signal peptide cleavage, the mature circulating form is a 315-amino acid polypeptide designated FS-315 [1][4].
FS-315 functions as a high-affinity antagonist of multiple TGF-beta superfamily members, most notably myostatin (GDF-8) and activin A/B. The protein contains three follistatin domains (FSD1-3) and a distinctive 27-amino acid C-terminal acidic tail (44% acidic residues) that masks heparan sulfate proteoglycan binding sites. This structural feature prevents cell-surface sequestration and permits systemic distribution, distinguishing FS-315 from the tissue-associated FS-288 isoform [4][5].
The primary mechanism of action involves stoichiometric binding to myostatin, preventing its interaction with activin receptor type IIB (ActRIIB) on skeletal muscle cells. By blocking ActRIIB-mediated Smad2/3 signaling, follistatin removes the endogenous brake on muscle protein synthesis and satellite cell proliferation [1][2]. Follistatin additionally neutralizes activin A, providing a dual anti-catabolic effect that outperforms single-target myostatin inhibitors. Studies in follistatin transgenic mice with concurrent myostatin deletion showed approximately four-fold muscle mass increase, demonstrating that follistatin blocks growth-limiting signals beyond myostatin alone [2].
Molecular Identity
Attribute
Common Names
- Detail
- Follistatin-344, FS-344, FST-344, FS344, Activin-Binding Protein
Attribute
Amino Acid Chain
- Detail
- 344 amino acids (precursor); 315 amino acids (mature circulating form, FS-315)
Attribute
Molecular Weight
- Detail
- ~37,800 Da (FS-315 mature form); ~39 kDa glycosylated recombinant
Attribute
Type
- Detail
- Monomeric glycoprotein
Attribute
CAS Number
- Detail
- 80449-31-6
Attribute
UniProt
- Detail
- P19883 (human FST gene product; encompasses FS288, FS303, FS315, FS344 isoforms)
Attribute
PDB
- Detail
- 2P6A (FS315-Activin A complex)
Attribute
NCBI Gene
- Detail
- Gene ID 10468 (human FST gene)
Attribute
Key Structural Features
- Detail
- Three follistatin domains (FSD1-3); ~36 cysteines forming disulfide bonds; N-linked and O-linked glycosylation; 27-amino acid acidic C-terminal tail unique to FS-344 lineage
Attribute
Post-translational Processing
- Detail
- Signal peptide cleavage generates FS-315; further C-terminal cleavage may produce FS-303 intermediate
Attribute
Solubility
- Detail
- PBS or sterile water
Mechanism of Action
The Basics
Think of muscle growth like a car with both an accelerator and a speed limiter. Most muscle-building approaches work by pressing harder on the accelerator: more testosterone, more growth hormone, more protein. Follistatin takes a different approach entirely. It removes the speed limiter.
That limiter is myostatin, a protein your body constantly produces to tell muscles "stop growing." Every human has it, and it serves an evolutionary purpose: unlimited muscle growth would demand enormous caloric resources. But for people trying to build muscle, myostatin is the ceiling you hit no matter how perfectly you train and eat.
Follistatin intercepts myostatin before it can reach muscle cells, binding to it and rendering it inactive. But follistatin does not stop there. It also neutralizes activin A and activin B, two additional proteins in the same family that suppress muscle growth. This multi-target approach is why follistatin outperforms compounds that only block myostatin [2].
There is a third mechanism: satellite cell activation. Satellite cells are your muscle's stem cells, responsible for building new muscle fibers and repairing damaged ones. Myostatin normally keeps satellite cells dormant. When follistatin removes that suppression, satellite cells become free to proliferate and differentiate, potentially leading to the creation of entirely new muscle fibers rather than just enlarging existing ones [6].
The Science
Follistatin's mechanism of action centers on antagonism of TGF-beta superfamily ligands through direct protein-protein interaction.
Myostatin neutralization: Follistatin binds myostatin (GDF-8) with high affinity (Kd ~0.5-5 nM), forming an irreversible complex that prevents myostatin from engaging ActRIIB receptors on skeletal muscle cells [1][2]. This blocks downstream Smad2/3 phosphorylation and nuclear translocation, removing the transcriptional program that suppresses myofibrillar protein synthesis and limits muscle fiber hypertrophy.
Activin A/B blockade: Follistatin neutralizes activin A and activin B through the same binding mechanism, disrupting an additional arm of TGF-beta superfamily signaling that independently constrains muscle mass. In mice with both myostatin deletion and follistatin overexpression, muscle mass reached approximately four times normal, indicating that activin blockade contributes substantially beyond myostatin inhibition alone [2].
Satellite cell activation: Myostatin maintains muscle satellite cells in a quiescent state through Smad-mediated suppression of MyoD and other myogenic regulatory factors. Follistatin's neutralization of myostatin releases satellite cells from this quiescent state, enabling proliferation and differentiation [6]. Notably, when satellite cell function was ablated through irradiation, follistatin still produced approximately 20% muscle growth through hypertrophy alone, demonstrating that satellite cell-independent mechanisms also contribute [6].
Isoform-specific distribution: The FS-315 isoform (derived from FS-344 processing) circulates systemically due to its acidic C-terminal tail masking heparin-binding sites. This contrasts with FS-288, which binds cell-surface heparan sulfate proteoglycans and remains tissue-associated. The systemic distribution of FS-315 enables whole-body myostatin neutralization [4][5].
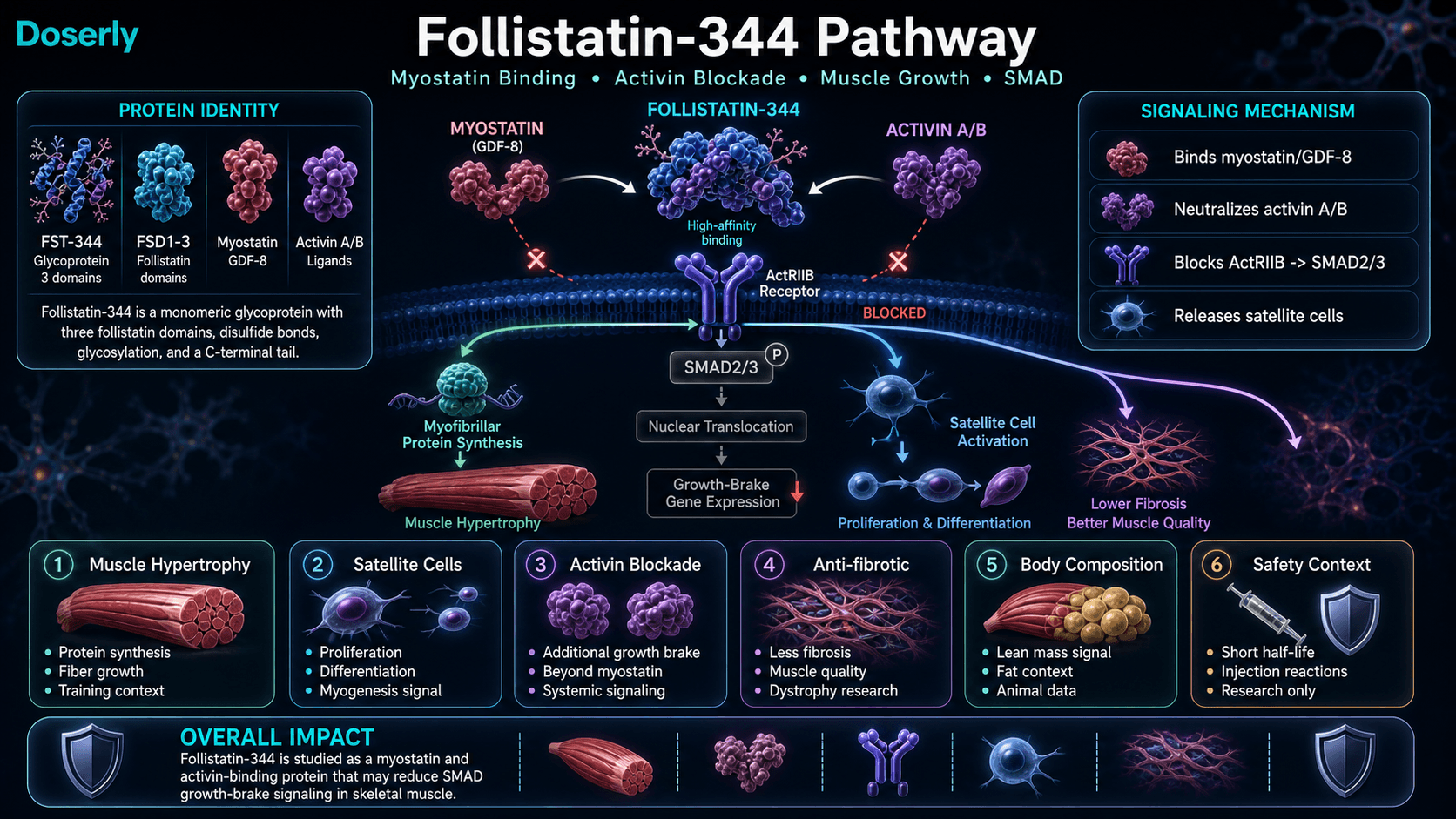
Pathway Visualization Image
Pharmacokinetics
The Basics
Follistatin-344 clears out of the body quickly. After injection, the protein reaches peak blood levels within about 9 minutes and has a half-life of roughly 90 minutes to 2 hours. This means that within 7 to 8 hours, the peptide is essentially cleared from your system.
This short half-life is one of the key limitations of the injectable form. Gene therapy studies, where the body produces follistatin continuously for months, show dramatic muscle growth. But a daily injection that keeps levels elevated for only a few hours may not provide sufficient exposure to meaningfully suppress myostatin throughout the day. This pharmacokinetic reality is why some researchers are developing engineered follistatin variants with improved half-life, with one variant achieving approximately 100-fold improvement [7].
The protein is administered either subcutaneously or intramuscularly, with subcutaneous injection into abdominal fat being the more common approach. Due to its large molecular size (~38 kDa), follistatin cannot be absorbed orally (digestive enzymes destroy it) and is too large for nasal or transdermal delivery.
The Science
Pharmacokinetic characterization of native follistatin relies primarily on preclinical models, as comprehensive human PK studies of the injectable peptide form have not been published.
Absorption: Following subcutaneous administration, peak plasma concentration (Tmax) occurs at approximately 9 minutes [7]. The rapid absorption reflects the protein's hydrophilic nature and moderate molecular size relative to the large pore system of subcutaneous capillaries.
Half-life: Plasma elimination half-life is approximately 1.5 to 2 hours, with receptor-mediated clearance contributing to the rapid elimination [7]. Steady-state with regular dosing would theoretically be achieved at approximately 7.5 to 9 hours.
Distribution: As a glycoprotein of approximately 37-40 kDa, volume of distribution is limited by size. The FS-315 isoform circulates systemically rather than being sequestered on cell surfaces, a property conferred by the acidic C-terminal tail [4].
Pharmacodynamic persistence: While plasma concentrations decline rapidly, downstream biological effects (satellite cell activation, shifts in protein synthesis/degradation balance) may persist beyond the pharmacokinetic window. In gene therapy studies, a single AAV-follistatin delivery produced measurable muscle hypertrophy lasting 15 or more months in primates [3].
Engineered variants: Datta-Mannan et al. (2013) reported that an engineered follistatin-Fc fusion variant achieved approximately 100-fold improvement in half-life and approximately 1,600-fold improvement in exposure compared to native follistatin, addressing the poor PK profile that limits clinical utility of the unmodified protein [7].
Research & Clinical Evidence
Muscular Dystrophy and Muscle Wasting
The Basics
The most rigorous evidence for follistatin comes from gene therapy trials for muscular dystrophy. In these studies, doctors deliver the genetic instructions for follistatin directly into muscle tissue using a modified virus (AAV), causing those muscles to produce follistatin continuously.
In a Phase I/IIa trial for Becker muscular dystrophy, six patients received AAV-follistatin gene therapy into their leg muscles. Over one year, some patients improved their walking distance by up to 125 meters on a 6-minute walk test. Their muscle fibers grew larger (from approximately 40 to 59 micrometers in diameter), and muscle fibrosis decreased by 35-43% [8]. A separate gene therapy trial for sporadic inclusion body myositis (IBM), another muscle-wasting disease, showed the treatment stabilized muscle function in patients who would otherwise be expected to decline [9].
These results are genuinely encouraging for people with muscle-wasting diseases. However, they specifically demonstrate what happens when the body produces follistatin continuously via gene therapy, not what happens from short-term peptide injections.
The Science
Primate gene therapy (2009): AAV1-FS344 injection at 1x10^13 vector genomes in cynomolgus macaques produced a 15% increase in muscle circumference by 8 weeks, persisting beyond 15 months. Muscle fiber diameter increased from 65.5 to 87.7 micrometers (p < 0.05). No adverse effects were observed on cardiac function, reproductive organs, or other organ systems [3].
Phase I/IIa Becker muscular dystrophy (2015): Six BMD patients received intramuscular AAV1.CMV.FS344. Results at 12 months included improvements in the 6-minute walk test (up to +125 meters), increased muscle fiber diameter (40 to 59 micrometers), and 35-43% reduction in endomysial fibrosis. No serious adverse events were reported [8][10].
Mouse models (2001, 2008): Follistatin transgenic mice demonstrated 194-327% muscle mass increase across multiple muscle groups. Effects persisted over 2 years without gross health abnormalities. The Lee and McPherron (2001) study established the foundational myostatin-follistatin biology showing 2-3x muscle mass in follistatin overexpressing animals [1][2].
Fat Loss (Preclinical)
The Basics
An interesting secondary finding from animal studies is that follistatin may reduce body fat in addition to building muscle. When researchers delivered follistatin instructions via nanoparticles (tiny fat bubbles rather than viruses), the treated mice built muscle and, somewhat unexpectedly, lost significant body fat. This dual effect occurs because follistatin blocks not only myostatin (which limits muscle) but also activin A (which appears to promote fat accumulation) [11].
This is still early-stage preclinical data, and the fat loss effects have not been studied in humans using the injectable peptide form.
The Science
Lipid nanoparticle-mediated delivery of FS-344 mRNA in murine models produced hepatic expression of follistatin for approximately 3 days per treatment. Animals demonstrated concurrent increases in lean mass and reductions in adipose tissue, attributed to simultaneous myostatin and activin A inhibition [11]. The dual-action "more muscle, less fat" phenotype positions FS-344-based therapies as candidates for sarcopenic obesity research, though translation to human injectable protocols remains speculative.
Biomarker Evidence Matrix
Category
Muscle Growth
- Evidence Strength
- 7/10
- Reported Effectiveness
- 4/10
- Summary
- Strong animal and gene therapy evidence (2-3x muscle mass in mice [1][2], 15% increase in primates [3], human gene therapy improvements [8]). Community reports of injectable peptide are mixed, with most users describing effects as subtle or absent.
Category
Recovery & Healing
- Evidence Strength
- 4/10
- Reported Effectiveness
- 4/10
- Summary
- Theoretical benefit from satellite cell activation and tissue remodeling. Limited direct evidence. Community reports are inconsistent, with confounding from stacking with BPC-157/TB-500.
Category
Fat Loss
- Evidence Strength
- 4/10
- Reported Effectiveness
- N/A
- Summary
- Preclinical nanoparticle delivery study showed fat reduction in mice [11]. No human data. No community discussion of fat loss from injectable FST-344.
Category
Physical Performance
- Evidence Strength
- 3/10
- Reported Effectiveness
- 3/10
- Summary
- No direct performance studies. Theoretical benefit from increased muscle mass. Community reports do not describe notable performance improvements from short peptide cycles.
Category
Joint Health
- Evidence Strength
- 2/10
- Reported Effectiveness
- 3/10
- Summary
- No evidence supporting joint health benefits. Community data suggests joint stress may be a concern if rapid muscle growth outpaces connective tissue adaptation.
Category
Hair Health
- Evidence Strength
- 2/10
- Reported Effectiveness
- N/A
- Summary
- Mentioned in one source as a research area but no published studies or community reports supporting hair growth from FST-344.
Category
Side Effect Burden
- Evidence Strength
- 5/10
- Reported Effectiveness
- 5/10
- Summary
- Gene therapy trials show good safety profile [3][8]. Injectable peptide community reports note injection site reactions (welts, lumps) as the primary concern. Long-term effects of exogenous peptide administration unknown.
Categories with community data: 5
Categories not scored (insufficient data): Weight Management, Appetite & Satiety, Food Noise, Energy Levels, Sleep Quality, Focus & Mental Clarity, Memory & Cognition, Mood & Wellbeing, Anxiety, Stress Tolerance, Motivation & Drive, Emotional Aliveness, Emotional Regulation, Libido, Sexual Function, Inflammation, Pain Management, Gut Health, Digestive Comfort, Nausea & GI Tolerance, Skin Health, Heart Health, Blood Pressure, Heart Rate & Palpitations, Hormonal Symptoms, Temperature Regulation, Fluid Retention, Body Image, Immune Function, Bone Health, Longevity & Neuroprotection, Cravings & Impulse Control, Social Connection, Treatment Adherence, Withdrawal Symptoms, Daily Functioning
Benefits & Potential Effects
The Basics
Follistatin-344's primary appeal is muscle growth through myostatin inhibition. By neutralizing the protein that limits how much muscle your body can build, follistatin creates the conditions for growth beyond what training and nutrition alone can achieve. In animal studies, this effect is dramatic: double or triple the normal muscle mass. In human anecdotal reports, the effect appears much more modest, with users describing subtle improvements in muscle fullness, better training response, or slight gains in lagging body parts.
Beyond muscle, follistatin shows potential in a few other areas. The most clinically relevant is muscular dystrophy treatment, where gene therapy trials have shown genuine improvement in muscle function and reduced fibrosis [8][9]. There is also preclinical evidence suggesting body fat reduction as a secondary effect of activin A neutralization [11]. Some sources mention potential for hair growth improvement, though published data supporting this application is absent.
It is important to set realistic expectations. The dramatic results from gene therapy studies, where the body produces follistatin continuously for months, do not translate directly to short-cycle injectable peptide protocols. The injectable form's 90-minute half-life means each dose provides only brief exposure, and most community members report that results from typical 10-15 day cycles are underwhelming compared to the theoretical promise.
The Science
Muscle hypertrophy: Gene therapy models consistently demonstrate significant skeletal muscle hypertrophy. Transgenic mice show 194-327% increase in muscle mass [2]. Primate studies with AAV1-FS344 produced a 15% increase in muscle circumference sustained for 15+ months, with fiber diameter increasing from 65.5 to 87.7 micrometers [3]. Phase I/IIa human gene therapy trials in BMD patients showed fiber diameter increase from 40 to 59 micrometers and 35-43% reduction in fibrosis [8].
Anti-fibrotic effects: Follistatin reduces muscle fibrosis by 35-43% in human gene therapy trials, improving the quality and function of muscle tissue in addition to increasing mass [8].
Body composition: Nanoparticle-mediated FS-344 mRNA delivery produced concurrent increases in lean mass and decreases in adipose tissue in murine models, through dual inhibition of myostatin and activin A [11].
Satellite cell proliferation: By removing myostatin-mediated suppression, follistatin activates satellite cell proliferation and differentiation, potentially enabling myogenesis (new fiber formation) in addition to hypertrophy (fiber enlargement) [6].
Side Effects & Safety Considerations
The Basics
Most safety data for follistatin comes from gene therapy trials rather than injectable peptide use, which makes the safety profile of the injectable form less well-characterized.
In gene therapy trials, the compound has shown a surprisingly clean safety profile. Primate studies lasting 15 months showed no adverse effects on heart function, reproductive organs, or other organ systems [3]. Human gene therapy trials reported no serious adverse events over 12 months [8].
For the injectable peptide, community reports highlight injection site reactions as the primary concern. Multiple users independently report warm welts, redness, and lumps at injection sites that can last several days. Some users find these reactions manageable with icing before and after injection, while others discontinue due to persistent reactions.
Theoretical concerns include potential effects on reproductive function (follistatin neutralizes activin, which regulates FSH and reproductive signaling), minor increases in LDL cholesterol (approximately 8 mg/dL reported in one context), and long-term risks of chronic TGF-beta inhibition including potential effects on bone density and organ fibrosis. One report noted central serous chorioretinopathy (a vision condition) at a dose 10 times the typical range.
Any vision changes during use should prompt immediate discontinuation and medical evaluation.
The Science
Gene therapy safety: AAV1-FS344 gene therapy in cynomolgus macaques showed no cardiac hypertrophy, no reproductive organ effects, and no abnormalities across comprehensive organ panel assessment over 15 months [3]. Phase I/IIa human trials in BMD patients reported no serious adverse events, with echocardiographic monitoring confirming no pathological cardiac effects [8][10].
Reproductive considerations: Follistatin neutralizes activin A and B, which are key regulators of FSH secretion from the anterior pituitary. Theoretical FSH suppression could affect reproductive function in both sexes. However, the primate gene therapy study specifically evaluated reproductive organs and found no adverse effects [3]. The short half-life of injectable peptide may limit systemic reproductive effects compared to sustained gene therapy expression.
Injection site reactions: Community reports consistently describe localized inflammatory responses at subcutaneous injection sites, including erythema, warmth, and subcutaneous nodules lasting 2-5 days. These reactions likely reflect an immune response to the recombinant protein and may indicate product purity variability.
Cardiovascular considerations: Rapid muscle mass increases from potent myostatin inhibition theoretically stress the cardiovascular system. This concern led to the discontinuation of ACE-031 (a soluble ActRIIB decoy receptor) after vascular adverse events in clinical trials, though follistatin's mechanism of action differs from receptor decoy approaches [5].
Contraindications based on available data: Cardiovascular disease (theoretical cardiac strain from rapid muscle growth), active cancer (complex TGF-beta effects on tumor biology), pregnancy and breastfeeding (activin role in reproductive physiology), and liver or kidney impairment [5].
Side effect profiles are most useful when you can compare them against your own experience in real time. Doserly lets you log symptoms, severity, and timing alongside your dosing data, creating a side-by-side view of your protocol and your body's response.
This kind of systematic tracking catches things that memory alone misses. A subtle mood shift that began three days after a dose increase. Sleep disruption that correlates with evening administration. These patterns become visible when the data is laid out on a timeline, and they give your healthcare provider actionable information rather than vague concerns. Early detection of emerging side effects means earlier intervention.
Keep side effects, flags, and follow-up notes visible.
Doserly helps you document safety observations, side effects, medication changes, and follow-up questions so important context is not scattered.
Safety log
Flags and notes

Safety notes are not emergency guidance; seek medical help when appropriate.
Dosing Protocols
The Basics
There is no established clinical dosing standard for injectable follistatin-344. All dosing information comes from community reports and practitioner anecdotes rather than controlled trials.
The most commonly cited dose across community sources is 100 mcg per day administered subcutaneously. Some sources report an upper range of 200 mcg per day. Cycles are typically short, ranging from 10 to 30 days, followed by a washout period of 3 to 4 weeks.
One source describes a "blast protocol" of 100 mcg daily for 10 days, while standard research protocols are cited at 100 mcg every other day. One practitioner-sourced report describes a substantially different approach: 2.5 mg per week (split across injections) for 12 weeks, which represents approximately 350 mcg per day, well above the commonly cited range.
The short half-life of approximately 90 minutes raises questions about whether daily dosing provides sufficient exposure for meaningful myostatin suppression throughout the day. Some community members report feeling that short 10-15 day cycles are insufficient to produce noticeable results.
Given the lack of established protocols, consultation with a qualified healthcare provider is essential for anyone considering this compound.
The Science
No dose-finding studies or controlled clinical trials of injectable follistatin-344 have been published. All dosing data is derived from anecdotal community protocols and extrapolation from gene therapy trial parameters.
Community-reported protocols:
- Standard: 100 mcg subcutaneous daily, 10-30 day cycles with 3-4 week washout
- Blast: 100 mcg subcutaneous daily for 10 consecutive days
- EOD (every other day): 100 mcg subcutaneous, extended cycles
Reconstitution: 1.0 mL bacteriostatic water or sterile water per vial. The protein should be swirled gently rather than shaken, as vigorous agitation can denature glycoproteins.
Timing: No established optimal timing. Some sources suggest post-workout administration for exercise-mimetic research contexts. Others suggest morning administration. The short half-life means timing relative to training may have limited practical significance.
Gene therapy reference: Human gene therapy trials used AAV1.CMV.FS344 delivered intramuscularly at doses of 1x10^12 to 6x10^13 vector genomes. These protocols achieve sustained local follistatin expression and are not directly comparable to systemic peptide injection [8][10].
The dosing protocols above involve numbers that matter: specific microgram amounts, reconstitution ratios, and timing windows. Getting any of these wrong compounds across every subsequent dose from that vial.
Doserly's dose and reconstitution calculators eliminate the guesswork. Enter your vial size, peptide amount, and target dose, and get the exact bacteriostatic water volume, units per tick mark, and doses per vial. The injection site tracker maps your administration history as a visual heat map across your body, flagging areas that need rest and suggesting rotation patterns. Combined with dose reminders that include compound name, amount, and route, every aspect of your daily protocol is handled with the precision it requires.
Build reminders around the routine, not just the compound.
Doserly can keep timing, skipped doses, and schedule changes organized so the plan you read about becomes easier to follow and review.
Today view
Upcoming reminders

Reminder tracking supports consistency; it does not select a protocol for you.
What to Expect
Week-by-week expectations for injectable follistatin-344 are poorly established due to the lack of clinical data and the wide variation in community reports. The following timeline represents a synthesis of available anecdotal information and should be treated with significant skepticism.
Week 1-2: Most users report no noticeable changes during this period. Some experience injection site reactions (welts, soreness, redness) that may or may not diminish over time. One user reported muscle soreness at the injection site similar to post-workout DOMS.
Week 2-4: A small number of users describe subtle improvements in muscle fullness or training response during this window. However, many users report completing their 10-15 day cycle with no discernible effects.
Week 4-8 (for extended protocols): One practitioner-sourced report describes measurable increases in lean mass and improved recovery between training sessions during this window, but this was associated with substantially higher doses (2.5 mg/week) than typical community protocols.
Week 8-12+: Extended protocols are rarely reported in community data. The few available reports suggest gradual, modest improvements in lean mass for users who are already training consistently with optimized nutrition. One historical report estimated 7-9 pounds of skeletal muscle gain over a full 12-week cycle in an experienced lifter near their genetic ceiling.
Important context: The most dramatic follistatin results in the literature (15% muscle circumference increase, 194-327% muscle mass increase) come from gene therapy providing sustained expression over many months. These outcomes should not be expected from short-cycle injectable peptide protocols. Community sentiment leans strongly toward "subtle at best" for the injectable form.
Interaction Compatibility
Potentially Complementary
- BPC-157: Different mechanisms; BPC-157's healing and angiogenic properties may complement follistatin's growth-promoting effects. No interaction data available. Some community members stack these compounds.
- TB-500: Both promote tissue regeneration through different pathways. TB-500's satellite cell mobilization via actin sequestration is mechanistically distinct from follistatin's myostatin inhibition. No interaction studies exist. Community protocols sometimes include TB-500 at low doses alongside follistatin for recovery support.
- IGF-1 LR3: Theoretical synergy as both promote anabolic signaling through different pathways. No interaction studies available.
- CJC-1295 + Ipamorelin: Growth hormone secretagogue combinations may complement myostatin inhibition by promoting anabolic signaling through the GH/IGF-1 axis. No safety data for the combination.
Use with Caution
- HGH: Both are anabolic. Combined use risks excessive growth factor stimulation. Monitor closely if combining.
- Testosterone/Androgens: Different pathways but additive anabolic effects. No human data on the combination.
Avoid Combining
- ACE-031: Both target myostatin signaling. ACE-031 (soluble ActRIIB decoy receptor) was discontinued after vascular adverse events in clinical trials. Stacking myostatin inhibitors provides no demonstrated benefit and increases off-target risk.
- Other myostatin inhibitors: Combining multiple compounds targeting the same pathway offers no additional benefit and increases the potential for adverse effects.
Administration Guide
Materials required:
- Follistatin-344 lyophilized powder vial
- Bacteriostatic water (or sterile water for injection)
- Insulin syringes (29-31 gauge, 0.5-1 mL)
- Alcohol prep pads
- Sharps disposal container
Recommended reconstitution solution: Bacteriostatic water is preferred for multi-dose vials, as its preservative (benzyl alcohol) inhibits bacterial growth. Sterile water may be used for single-use preparation. Add water slowly down the side of the vial and swirl gently. Do not shake, as vigorous agitation can denature the glycoprotein. The solution should be clear; discard if cloudy or discolored.
Timing considerations: No optimal timing has been established. Some protocols suggest post-workout administration, while others suggest morning injection. Given the short half-life (~90 minutes), the timing relative to training or meals is unlikely to have a large impact on overall efficacy.
Post-administration care: Monitor injection sites for reactions. Warm welts, redness, and lumps are commonly reported and typically resolve within 2-5 days. Icing the injection site for 10 minutes before and after administration may reduce reaction severity. Report any vision changes, signs of hormonal disruption, or unusual swelling to a healthcare provider immediately.
Supplies & Planning
Supply
Follistatin-344 Vials
- Details
- Typically supplied as 1 mg lyophilized powder per vial
Supply
Bacteriostatic Water
- Details
- Standard reconstitution diluent; 0.9% benzyl alcohol preservative
Supply
Insulin Syringes
- Details
- U-100, 29-31 gauge, 0.5 mL or 1 mL capacity
Supply
Alcohol Prep Pads
- Details
- 70% isopropyl alcohol for site and vial stopper preparation
Supply
Sharps Container
- Details
- For safe disposal of used syringes
Supply
Ice Packs
- Details
- Optional; some users ice injection sites to reduce reactions
Note on cost: Follistatin-344 is among the most expensive research peptides. Community members report costs of approximately $125-155 per 1 mg vial. A 15-day cycle at 100 mcg/day requires approximately 1.5 vials. Extended protocols (8-12 weeks) can cost $650-1,200 or more. The cost-to-benefit ratio is a significant consideration given the modest and inconsistent results reported by most community users.
Product authenticity concern: Multiple community sources warn that follistatin-344 is frequently counterfeited due to the expensive and technically demanding manufacturing process. Third-party certificates of analysis (COAs) from independent labs are strongly recommended.
Consult a healthcare provider and use a reconstitution calculator for preparation specifics.
Storage & Handling
Lyophilized powder:
- Long-term storage: -20°C (-4°F) or below, ideally -80°C for storage beyond several months
- Short-term: 2-8°C (35.6-46.4°F) for weeks to months
- Keep in original sealed packaging with desiccant to minimize moisture exposure
- Protect from light
- Allow vials to reach room temperature (10-30 minutes) before opening to prevent condensation
Reconstituted solution:
- Store at 2-8°C (35.6-46.4°F) immediately after reconstitution
- Use within 7 days when reconstituted with bacteriostatic water
- Do NOT freeze reconstituted solutions, as freezing denatures the glycoprotein
- Inspect before each use for clarity; discard if cloudy, discolored, or containing particulates
- As a large glycoprotein (~38 kDa), follistatin requires gentler handling than smaller peptides
Critical notes:
- Avoid freeze-thaw cycles, which cause irreversible protein degradation
- Do not shake vials at any stage
- Label vials with reconstitution date
Lifestyle Factors
The lifestyle context around follistatin-344 is arguably more important than for most peptides, because the compound's mechanism removes a growth brake rather than providing a growth signal. Without the stimulus of proper training and adequate nutrition, removing that brake achieves very little.
Nutrition: A calorie-surplus, high-protein diet is essential for capitalizing on myostatin inhibition. The increased capacity for muscle protein synthesis means protein demands are elevated. Most sources recommend prioritizing protein intake and ensuring total caloric intake supports growth. Using follistatin during a caloric deficit undercuts its primary mechanism.
Training: Heavy resistance training with progressive overload provides the mechanical stimulus that myostatin inhibition amplifies. Without structured training, satellite cell activation and increased protein synthesis have nothing to build upon. Periodization across muscle groups may be particularly important given community observations that follistatin appears to promote growth preferentially in lagging body parts.
Sleep: 7-9 hours of quality sleep supports the tissue repair and anabolic signaling processes that follistatin facilitates. Growth hormone release during deep sleep may complement myostatin inhibition.
Joint and connective tissue support: Rapid muscle growth that outpaces connective tissue adaptation can increase injury risk. Consider joint-support supplementation and monitor for signs of tendon or ligament strain during use.
Monitoring: Given the theoretical concerns about FSH suppression and cholesterol changes, baseline and follow-up blood work (including hormone panel, lipids, and liver/kidney function) is prudent for anyone using this compound.
The lifestyle factors above, nutrition, exercise, sleep, stress management, are not just nice-to-haves alongside a peptide protocol. They're force multipliers. Doserly lets you track these inputs alongside your compounds, building a complete picture of what your body is receiving and how it's responding.
When everything lives in one dashboard, patterns emerge. You can see whether training days correlate with better biomarker trends, whether your sleep scores predict next-day recovery quality, or whether stress spikes derail your progress in measurable ways. This kind of integrated tracking turns the lifestyle recommendations in this section from abstract advice into actionable, personalized insight.
Keep sensitive protocol records in a purpose-built app.
Doserly is designed for private health tracking with structured records, offline-ready workflows, and exportable history when you need it.
Privacy
Health records

Privacy controls help you manage records; keep clinical records where required.
Regulatory Status & Research Classification
United States (FDA): Follistatin-344 is not approved by the FDA for any human therapeutic use. It is classified as a research compound. Gene therapy variants (AAV-follistatin) have been investigated in Phase I/II clinical trials for muscular dystrophy under IND applications [8][9][10].
Canada (Health Canada): Not approved. No DIN or NPN classification.
United Kingdom (MHRA): Not approved for therapeutic use.
Australia (TGA): Not scheduled for approved therapeutic use.
European Union (EMA): No marketing authorization.
WADA Status: Follistatin is explicitly prohibited under WADA's list of gene doping substances and methods. Specifically prohibited since 2019. Anti-doping agencies have developed detection methods for follistatin gene doping in athletes. Use by competitive athletes in WADA-governed sports results in anti-doping violations.
Active clinical trials: Gene therapy approaches using AAV-follistatin vectors have been investigated in registered clinical trials:
- Phase I/II for Becker muscular dystrophy (Mendell et al.) [8][10]
- Phase I/IIa for sporadic inclusion body myositis [9]
These trials use gene therapy delivery, not injectable peptide protocols.
Regulatory note: Regulatory status changes frequently. Always verify the current legal status of any compound in your specific country or jurisdiction before making any decisions.
FAQ
What is follistatin-344 and how does it work?
Follistatin-344 is a naturally occurring glycoprotein that neutralizes myostatin and activin A, two proteins in the TGF-beta superfamily that suppress muscle growth. By binding and blocking these growth limiters, follistatin removes the body's natural cap on muscle development, allowing for increased muscle protein synthesis and satellite cell activation.
Is follistatin-344 the same as the follistatin used in gene therapy studies?
The same protein is involved, but the delivery method differs significantly. Gene therapy uses viral vectors (AAV) to deliver the genetic instructions for follistatin, causing the body to produce the protein continuously for months or years. Injectable peptide protocols deliver the protein directly, but it has a half-life of only about 90 minutes and requires repeated dosing. The dramatic results from gene therapy studies should not be extrapolated to injectable peptide use.
What dosing protocols are commonly reported for injectable follistatin-344?
Based on available community sources, commonly reported ranges include 100-200 mcg per day via subcutaneous injection, typically administered in short cycles of 10-30 days followed by a 3-4 week washout. There is no clinically established dosing standard. Anyone considering use should consult with a qualified healthcare provider.
How long does it take to see results from follistatin-344?
Community reports vary widely. Some users report subtle improvements in muscle fullness or training response within 2-4 weeks, while many others report completing entire cycles with no noticeable effects. Gene therapy studies showed measurable changes by week 8. Setting realistic expectations is important, as the injectable peptide form appears to produce much more modest effects than the gene therapy approach.
What are the main side effects of follistatin-344?
The most commonly reported side effect from community sources is injection site reactions, including warm welts, redness, and lumps lasting several days. Theoretical concerns include FSH suppression (affecting reproductive function), minor LDL cholesterol elevation, and potential effects on bone density with chronic TGF-beta inhibition. Gene therapy safety data over 15 months in primates showed no cardiac, reproductive, or organ abnormalities.
Is follistatin-344 legal?
Follistatin-344 is not approved by the FDA or equivalent regulatory bodies for human therapeutic use. It is sold as a research compound. It is explicitly prohibited by WADA for competitive athletes. Legal status varies by jurisdiction, and verification of local regulations is essential.
Why is follistatin-344 so expensive?
The manufacturing process for recombinant follistatin is technically demanding due to the protein's size (~38 kDa), complex folding (requiring multiple disulfide bonds), and glycosylation requirements. This complexity drives production costs. Community sources also warn that the high price point makes counterfeiting prevalent, and third-party testing is recommended.
Can follistatin-344 be taken orally?
No. As a large glycoprotein, follistatin is degraded by digestive enzymes and cannot survive gastrointestinal transit. It must be administered by injection, with subcutaneous being the most commonly reported route.
Sources & References
- Lee SJ, McPherron AC. "Regulation of myostatin activity and muscle growth." Proceedings of the National Academy of Sciences. 2001. DOI: 10.1073/pnas.181511198. Foundational study establishing myostatin-follistatin biology; follistatin transgenic mice showed 2-3x muscle mass.
- Lee SJ. "Quadrupling muscle mass in mice by targeting TGF-beta signaling pathways." PNAS. 2007. DOI: 10.1073/pnas.0709144105. Demonstrated that follistatin overexpression combined with myostatin deletion produces approximately 4x muscle mass, indicating follistatin blocks growth limiters beyond myostatin.
- Kota J, Handy CR, Haidet AM, et al. "Follistatin gene delivery enhances muscle growth and strength in nonhuman primates." Science Translational Medicine. 2009. DOI: 10.1126/scitranslmed.3000112. AAV1-FS344 in macaques: 15% circumference increase at 8 weeks, sustained 15+ months, no cardiac or reproductive adverse effects.
- Sidis Y, Mukherjee A, Keutmann H, et al. "Biological activity of follistatin isoforms and follistatin-like-3 is dependent on differential cell surface binding and specificity for activin, myostatin, and bone morphogenetic proteins." Endocrinology. 2006. Established the structural basis for FS-315 vs FS-288 isoform distribution and binding specificity.
- Lee SJ, Reed LA, Davies MV, et al. "Regulation of muscle growth by multiple ligands signaling through activin type II receptors." PNAS. 2005. Comprehensive review of myostatin inhibition approaches and rationale for FS-315 circulating form.
- Lee SJ, Huynh TV, Lee YS, et al. "Role of satellite cells versus myofibers in muscle hypertrophy induced by inhibition of the myostatin/activin signaling pathway." PNAS. 2012. DOI: 10.1073/pnas.1206410109. Demonstrated dual mechanism: satellite cell activation plus myofiber hypertrophy from follistatin.
- Datta-Mannan A, Yaden B, Engwall M, et al. "An engineered human follistatin variant: insights into the pharmacokinetic and pharmacodynamic relationships of a novel molecule with broad therapeutic potential." Journal of Pharmacology and Experimental Therapeutics. 2013. PubMed: 23946385. Engineered FS variant with ~100-fold improved half-life and ~1600-fold improved exposure.
- Mendell JR, Sahenk Z, Malik V, et al. "A phase 1/2a follistatin gene therapy trial for Becker muscular dystrophy." Molecular Therapy. 2015. DOI: 10.1038/mt.2014.200. PubMed: 25358252. Phase I/IIa human trial: 6-MWT improvements up to +125m, fiber diameter increase, 35-43% fibrosis reduction.
- Mendell JR, et al. "Follistatin gene therapy for sporadic inclusion body myositis improves functional outcomes." Molecular Therapy. 2017. PMC: PMC5383643. Human gene therapy trial for IBM showing functional stabilization.
- Al-Zaidy SA, Sahenk Z, Rodino-Klapac LR, et al. "Follistatin gene therapy improves ambulation in Becker muscular dystrophy." Journal of Neuromuscular Diseases. 2015. PubMed: 25135111. Additional Phase I/II gene therapy results for BMD.
- Loomis KH, Bachelder EM, Ainslie KM, et al. "Increasing lean muscle mass via nanoparticle-mediated delivery of follistatin mRNA." Molecular Therapy - Nucleic Acids. 2018. PMC: PMC6276093. Lipid nanoparticle FS-344 mRNA delivery: concurrent lean mass increase and fat reduction in mice.
Related Peptide Guides
- BPC-157 — Healing and tissue repair peptide, commonly stacked with follistatin for recovery support
- TB-500 — Tissue repair through actin sequestration, complementary mechanism to myostatin inhibition
- IGF-1 LR3 — Insulin-like growth factor with anabolic properties, theoretical synergy with myostatin inhibition
- PEG-MGF — Mechano-growth factor, promotes satellite cell activation through a different pathway
- CJC-1295 — Growth hormone releasing hormone analog, supports anabolic signaling via GH/IGF-1 axis
- Ipamorelin — Selective growth hormone secretagogue, commonly paired with CJC-1295
- MK-677 — Oral growth hormone secretagogue, alternative approach to anabolic signaling
- HCG — Hormonal support, relevant for monitoring reproductive effects during myostatin inhibitor use
- GHK-Cu — Tissue repair and anti-aging peptide with complementary regenerative mechanisms
Need the reconstitution math for Follistatin-344: Complete Research Guide?
Open the calculator with Follistatin-344: Complete Research Guide prefilled to estimate concentration, draw volume, and related measurement math from the reconstitution details you already have.