Sermorelin: Complete Research Guide
On this page
Quick Reference Card
Attribute
Also Known As
- Detail
- GRF(1-29), GHRH(1-29), Geref (discontinued brand name), Growth Hormone-Releasing Factor Fragment 1-29
Attribute
Administration
- Detail
- Injectable (subcutaneous), once daily at bedtime
Attribute
Research Status
- Detail
- Previously FDA-approved (1997, Geref) for pediatric GH deficiency. Commercially withdrawn 2008 (business reasons, not safety). Available through compounding pharmacies with prescription.
Attribute
Typical Dose Range
- Detail
- 200-500 mcg subcutaneously, once daily at bedtime
Attribute
Half-Life
- Detail
- 10-20 minutes (plasma elimination); downstream GH effects persist approximately 3 hours
Attribute
Cycle Length
- Detail
- 8-12 weeks on, 2-4 weeks off (practitioner-derived; some use 5 days on, 2 days off continuously)
Attribute
Storage
- Detail
- Lyophilized: 2-8C (refrigerate), protect from light. Reconstituted: 2-8C, use within 10-14 days with bacteriostatic water.
Overview / What Is Sermorelin?
The Basics
Sermorelin is the active core of your body's natural growth hormone-releasing hormone (GHRH), consisting of the first 29 amino acids of the full 44-amino acid hormone. Think of GHRH as a signal your brain sends to the pituitary gland every few hours, telling it to release a pulse of growth hormone. Sermorelin is the smallest piece of that signal that still works, reproduced synthetically so it can be administered as an injection.
What makes sermorelin different from injecting growth hormone directly is that it works with your body's existing control system rather than bypassing it. When you inject growth hormone, your blood levels rise regardless of what your body needs. When you inject sermorelin, it asks your pituitary to release growth hormone on its own terms. Your body's natural brake system (a hormone called somatostatin) stays active, which means your system can still regulate how much growth hormone actually enters your bloodstream. This built-in safety mechanism is why practitioners who prioritize a physiological approach often gravitate toward sermorelin.
Sermorelin has the longest clinical track record of any growth hormone secretagogue. It earned FDA approval in 1997 under the brand name Geref for diagnosing and treating growth hormone deficiency in children. The manufacturer withdrew it from the market in 2008, but that withdrawal had nothing to do with safety. It was a business decision driven by the economics of competing against established recombinant human growth hormone products. That history gives sermorelin the most defensible legal position of any GH secretagogue currently available through compounding pharmacies.
The Science
Sermorelin (GRF 1-29 NH2) is a synthetic 29-amino acid peptide representing the biologically active N-terminal fragment of human growth hormone-releasing hormone. The compound binds to GHRH receptors (GHRHR) on somatotroph cells in the anterior pituitary gland with a dissociation constant (Kd) in the low nanomolar range (2-5 nM), indicating high-affinity interaction [1][2].
Upon receptor binding, sermorelin activates the Gs protein-coupled adenylyl cyclase pathway, increasing intracellular cyclic AMP (cAMP) concentrations. This triggers protein kinase A (PKA) phosphorylation of cAMP response element-binding protein (CREB), enhancing GH gene transcription. Simultaneously, PKA promotes release of stored GH from dense-core secretory granules, producing both increased GH synthesis and acute secretion [2][3].
Critically, sermorelin-stimulated GH release remains subject to physiological negative feedback regulation. Rising GH and IGF-1 levels trigger hypothalamic somatostatin release, which tonically inhibits further pituitary GH secretion. This feedback loop preserves the pulsatile GH secretion pattern characteristic of normal physiology and limits the risk of supraphysiological GH elevation [3][4]. This represents a fundamental mechanistic distinction from exogenous recombinant human growth hormone (rhGH) administration, which bypasses pituitary regulation entirely.
The compound demonstrates clean selectivity at therapeutic doses, with no significant elevation of cortisol, ACTH, or prolactin [3]. This distinguishes it from ghrelin-receptor agonists (GHRP-2, GHRP-6, hexarelin), which can affect multiple hormonal axes.
Molecular Identity
Property
Amino Acid Sequence
- Detail
- Tyr-Ala-Asp-Ala-Ile-Phe-Thr-Asn-Ser-Tyr-Arg-Lys-Val-Leu-Gly-Gln-Leu-Ser-Ala-Arg-Lys-Leu-Leu-Gln-Asp-Ile-Met-Ser-Arg-NH2
Property
Molecular Formula
- Detail
- C149H246N44O42S
Property
Molecular Weight
- Detail
- 3,357.93 Da (free base); 3,417.99 Da (acetate salt)
Property
CAS Number
- Detail
- 86168-78-7 (free base); 114466-38-5 (acetate salt)
Property
PubChem CID
- Detail
- 16132413
Property
DrugBank ID
- Detail
- DB00010
Property
FDA UNII
- Detail
- 89243S03TE
Property
Peptide Length
- Detail
- 29 amino acids
Property
Structure Type
- Detail
- Linear peptide with C-terminal amidation (-NH2)
Property
Target Receptor
- Detail
- GHRH-R (Growth Hormone-Releasing Hormone Receptor)
Property
Salt Form
- Detail
- Typically supplied as acetate salt
Property
Appearance
- Detail
- White to off-white lyophilized powder
Mechanism of Action
The Basics
Your pituitary gland, a small structure at the base of your brain, functions like a hormone factory. One of its most important products is growth hormone (GH), which it releases in pulses throughout the day and night, with the largest pulse occurring during deep sleep.
Two opposing signals control this factory. The "go" signal is GHRH (growth hormone-releasing hormone), produced in the hypothalamus. The "stop" signal is somatostatin, also from the hypothalamus. Sermorelin mimics the "go" signal. It knocks on the same door that your natural GHRH knocks on, triggering the pituitary to release a pulse of growth hormone.
The important distinction is what happens next. When you inject growth hormone directly, you are dumping the finished product into your bloodstream and the factory's opinion is irrelevant. When you use sermorelin, the factory is doing the work. If your body senses that growth hormone levels are already high enough, somatostatin applies the brakes and the pituitary responds less, regardless of how much sermorelin is present. This self-regulating feature makes it substantially more difficult to achieve dangerously elevated GH levels compared to direct GH injection.
Once released, growth hormone travels to the liver and triggers production of insulin-like growth factor 1 (IGF-1). IGF-1 is the molecule that carries out most of the downstream effects people associate with growth hormone: tissue repair, muscle protein synthesis, fat metabolism, and cellular renewal.
The Science
Sermorelin activates the growth hormone-releasing hormone receptor (GHRHR), a class B (secretin-like) G protein-coupled receptor expressed on anterior pituitary somatotrophs. The receptor comprises 423 amino acids organized in a seven-transmembrane domain architecture with a large N-terminal extracellular domain (~120 residues) containing the primary ligand binding determinants [2].
The signaling cascade proceeds through well-characterized steps:
- GHRHR activation and Gs coupling: Sermorelin binding induces conformational changes that promote GDP-GTP exchange on the Gs alpha subunit, activating membrane-bound adenylyl cyclase [2][3].
- cAMP/PKA signaling: Elevated intracellular cAMP activates protein kinase A, which phosphorylates multiple downstream targets including CREB. Phosphorylated CREB binds to cAMP response elements in the GH gene promoter, enhancing transcription [2].
- GH vesicle exocytosis: PKA simultaneously phosphorylates proteins involved in secretory vesicle trafficking, promoting release of stored GH from dense-core granules [2].
- Preserved feedback regulation: Unlike exogenous rhGH, sermorelin-stimulated GH release remains subject to somatostatin-mediated inhibition. Rising GH and hepatic IGF-1 provide negative feedback at both hypothalamic (enhanced somatostatin release, suppressed GHRH release) and pituitary (direct somatotroph inhibition) levels [3][4].
- Pulsatile preservation: The interplay between stimulatory GHRH and inhibitory somatostatin maintains pulsatile GH secretion patterns (approximately every 3-5 hours), which is functionally significant because continuous GH exposure downregulates GH receptors, whereas pulsatile secretion maintains receptor sensitivity [3].
Mutations in GHRHR that impair ligand binding account for approximately 10% of hereditary GH deficiency cases, underscoring the receptor's critical role in normal somatotroph function [2].
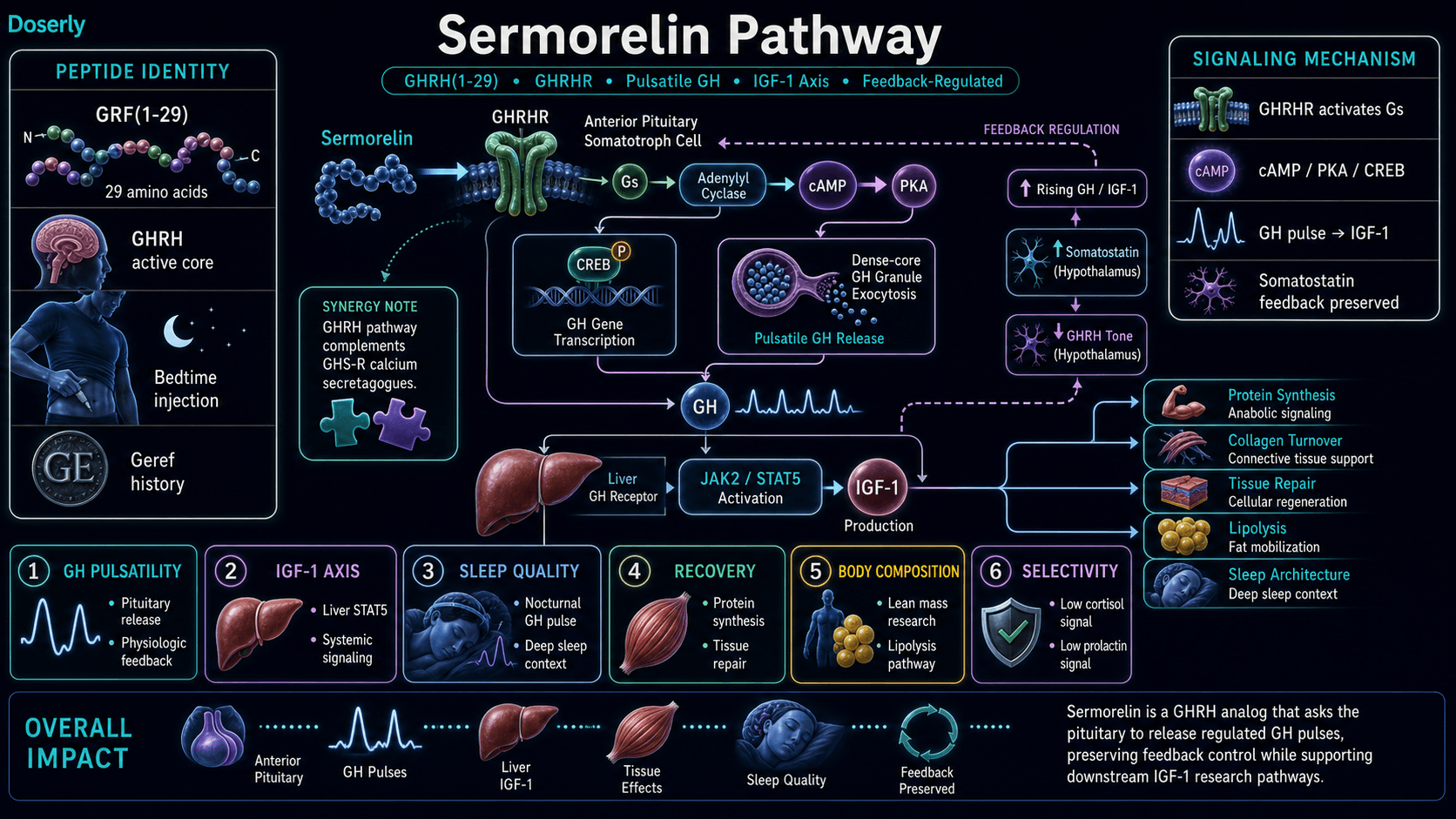
Pathway Visualization Image
Pharmacokinetics
The Basics
Sermorelin has a very short life in your bloodstream, typically clearing within 10-20 minutes after injection. This is actually by design. Rather than maintaining constant drug levels (which would eventually cause your body to stop responding), each injection creates a single sharp pulse that mimics the natural bursts of GHRH your brain produces during deep sleep.
When injected under the skin (subcutaneously), sermorelin reaches peak blood levels within about 5-20 minutes. However, only about 6% of the injected dose actually makes it into your bloodstream because enzymes at the injection site break down much of the peptide before it can be absorbed. Despite this low bioavailability, the amount that reaches the pituitary is sufficient to trigger a meaningful GH pulse.
The downstream effects last considerably longer than the peptide itself. After sermorelin disappears from the blood, the growth hormone pulse it triggered continues for roughly 2-3 hours, and the IGF-1 produced in response circulates for much longer. This is why once-daily bedtime dosing works: a single injection is enough to amplify the natural nocturnal GH pulse.
The short duration also means that if you experience any side effects (like flushing), they typically resolve quickly as the compound clears.
The Science
Key pharmacokinetic parameters based on published clinical data [1][2][5]:
- Route of administration: Subcutaneous injection (primary); intravenous (diagnostic use only)
- Tmax (time to peak concentration): 5-20 minutes following subcutaneous administration
- Bioavailability (subcutaneous): Approximately 6%, reflecting substantial first-pass proteolytic degradation at the injection site [2]
- Volume of distribution: 23.7-25.8 liters (approximating extracellular fluid volume), indicating limited tissue penetration consistent with the peptide's hydrophilic character [2]
- Plasma clearance: 2.4-2.8 L/min [2]
- Elimination half-life: 11-12 minutes (consistent across IV and SC routes) [2]
- Primary degradation pathways: Enzymatic hydrolysis by dipeptidyl peptidase-4 (DPP-4), neutral endopeptidase, and other serum/tissue proteases, plus renal ultrafiltration [2]
- Duration of GH-stimulating effect: Despite rapid plasma clearance, the triggered GH pulse persists for approximately 2-3 hours post-administration [1]
The low subcutaneous bioavailability (~6%) represents a significant pharmacokinetic limitation and has motivated development of structurally modified GHRH analogs. Tesamorelin incorporates a trans-3-hexenoic acid group providing DPP-4 resistance, while CJC-1295 (with DAC) uses Drug Affinity Complex technology for albumin binding and extended half-life [2]. Sermorelin, as the unmodified native sequence fragment, lacks these protective modifications.
Understanding half-life data points and clearance rates is informative, but seeing how they play out across your specific dosing schedule makes them actionable. Doserly's half-life estimator models your compound's concentration curve based on your dose, frequency, and route of administration, showing projected peaks, troughs, and steady-state levels over time.
Adjusting your dose or experimenting with timing? The estimator recalculates in real time, so you can visualize how titrating up, splitting doses, or changing frequency affects your blood levels before committing to a change. It transforms the pharmacokinetic data in this section from abstract numbers into a practical planning tool for your protocol.
Keep multi-step protocols organized from start to finish.
Use Doserly to map compounds, timing, cycle windows, notes, and review points so complex protocols stay readable in one place.
Plan view
Protocol schedule

Planning views are organizational and should be aligned with professional guidance.
Research & Clinical Evidence
Pediatric Growth Hormone Deficiency
The Basics
Sermorelin's strongest clinical evidence comes from pediatric trials that led to FDA approval. Children with growth hormone deficiency who received daily bedtime injections showed significant increases in how fast they grew, with improvements sustained over 12 months and some data extending to 36 months. These trials established that sermorelin can meaningfully stimulate the pituitary to release growth hormone and produce clinically measurable outcomes.
The practical finding was that sermorelin works, but not as powerfully as injecting growth hormone directly. In head-to-head comparisons at equivalent doses, recombinant human growth hormone (rhGH) produced faster growth. This is pharmacologically expected: asking the pituitary to make more hormone is inherently less potent than injecting the hormone itself. The trade-off is that sermorelin preserves the body's natural regulation, which some clinicians consider worth the reduced potency.
The Science
Clinical trials supporting FDA approval evaluated sermorelin at 30 mcg/kg/day subcutaneously in children with idiopathic growth hormone deficiency. Treatment demonstrated significant improvements in height velocity over 6-12 month periods, with preliminary data extending to 36 months of sustained growth effects [1][6].
Direct comparative data with rhGH at equivalent doses showed that sermorelin produced lower, though still clinically meaningful, height velocity increases [6]. This potency differential is mechanistically expected given the indirect mechanism of action and the approximately 6% subcutaneous bioavailability.
Adult Body Composition
The Basics
The evidence for adult use is much thinner than most wellness websites acknowledge. The entire adult clinical case rests primarily on a single small trial. In 1997, researchers gave a GHRH analog to 19 elderly adults (ages 55-71) for 16 weeks. The men in the study gained about 1.26 kg (roughly 2.8 pounds) of lean body mass, but the women did not. Nobody in the study lost a significant amount of body fat, gained bone density, or showed improvements in BMI.
This does not mean sermorelin has no value for adults. It means that the specific claims you will see on wellness websites ("increases lean muscle," "burns fat," "reverses aging") are built on a very small foundation. The lean mass finding is real, but it comes from fewer than 10 men over 16 weeks. Whether it applies to the typical person seeking sermorelin today (often a 35-55-year-old fitness-oriented adult) is genuinely unknown.
The Science
The primary adult evidence derives from Khorram et al. (1997), a single-blind trial of 19 elderly subjects (ages 55-71) treated with a GHRH analog for 16 weeks [7]:
- Nocturnal GH secretion: Significantly increased (P<0.01 in women, P<0.05 in men)
- IGF-1: Significantly increased (P<0.05)
- IGFBP-3: Significantly increased (P<0.001)
- Lean body mass: Improved in men only (P<0.05), approximately +1.26 kg
- Total body fat: No significant change in either sex
- BMI: No significant change
- Bone mineral density: No significant change
Limitations include the small sample (N=19), single-blind design, gender-discordant results, and absence of functional endpoints (strength, exercise capacity, quality of life) [7].
Within the GH secretagogue class, tesamorelin has substantially more adult evidence (two Phase III RCTs, N=816, demonstrating 15-20% visceral fat reduction) [8], while MK-677 has a 2-year RCT (N=65) showing +1.1 kg lean mass but no strength improvement [9]. CJC-1295 without DAC has no published human body composition trial data.
GH/IGF-1 Axis and Combination Therapy
The Basics
When sermorelin is combined with a ghrelin-receptor agonist (such as ipamorelin or GHRP-6), the two compounds work through different biological pathways that amplify each other. Research suggests this combination can produce 3 to 5 times greater growth hormone release than either compound alone. This synergy has led to combination protocols becoming common in clinical practice, though large-scale human trials specifically evaluating the combination remain limited.
The Science
Co-administration of GHRH and growth hormone secretagogues (GHS) exploits mechanistic synergy between two distinct signaling pathways: GHRHR-mediated cAMP/PKA signaling and GHS-R-mediated calcium mobilization through phospholipase C [2][10]. The resulting GH release exceeds the sum of individual responses by 3- to 5-fold. GHS additionally suppress hypothalamic somatostatin release, further amplifying GHRH effects [2].
A retrospective study of 14 hypogonadal men receiving triple-peptide therapy (GHRP-6 100 mcg, GHRP-2 100 mcg, sermorelin 100 mcg, three times daily) for 134 days demonstrated a 50% increase in IGF-1 (159.5 to 239.0 ng/mL) with preserved LH and FSH signaling [10]. This preservation of native gonadotropin signaling represents an important safety distinction from exogenous testosterone administration.
Biomarker Evidence Matrix
Category
Sleep Quality
- Evidence Strength
- 5/10
- Reported Effectiveness
- 8/10
- Summary
- GH pulsatility supports sleep architecture mechanistically. No published sermorelin sleep trial, but community reports are overwhelmingly positive. MK-677 (similar class) showed 50% increase in Stage 4 sleep [11].
Category
Recovery & Healing
- Evidence Strength
- 4/10
- Reported Effectiveness
- 7/10
- Summary
- GH/IGF-1 axis supports protein synthesis and tissue repair. Animal data supportive; human evidence for sermorelin specifically is limited to indirect GH/IGF-1 elevation. Community consistently reports faster workout recovery.
Category
Energy Levels
- Evidence Strength
- 3/10
- Reported Effectiveness
- 7/10
- Summary
- No direct clinical evidence for sermorelin and energy. Community reports improved daytime energy, likely secondary to improved sleep quality.
Category
Muscle Growth
- Evidence Strength
- 5/10
- Reported Effectiveness
- 6/10
- Summary
- Khorram 1997 showed +1.26 kg lean mass in elderly men (P<0.05). Limited to one small trial. Community reports moderate muscle definition improvements.
Category
Fat Loss
- Evidence Strength
- 4/10
- Reported Effectiveness
- 5/10
- Summary
- Khorram 1997 found no significant fat change. Mechanistically plausible via GH-mediated lipolysis, but direct evidence is absent. Community reports mixed and confounded by co-interventions.
Category
Mood & Wellbeing
- Evidence Strength
- 3/10
- Reported Effectiveness
- 6/10
- Summary
- No direct clinical data. Community reports improved wellbeing, likely secondary to better sleep and energy.
Category
Physical Performance
- Evidence Strength
- 4/10
- Reported Effectiveness
- 6/10
- Summary
- GH/IGF-1 axis supports exercise capacity. No sermorelin-specific performance trials. Community reports improved gym performance and endurance.
Category
Skin Health
- Evidence Strength
- 3/10
- Reported Effectiveness
- 5/10
- Summary
- GH/IGF-1 stimulates collagen synthesis. No sermorelin skin trials. Sparse but positive community reports after several months of use.
Category
Focus & Mental Clarity
- Evidence Strength
- 2/10
- Reported Effectiveness
- 5/10
- Summary
- No clinical evidence. Small number of community reports describe reduced brain fog.
Category
Side Effect Burden
- Evidence Strength
- 6/10
- Reported Effectiveness
- 7/10
- Summary
- Well-characterized from FDA approval era. Injection site reactions (~17%), flushing (5-15%), headache (~10%). Generally well-tolerated with low discontinuation rates.
Category
Joint Health
- Evidence Strength
- 3/10
- Reported Effectiveness
- 5/10
- Summary
- GH/IGF-1 supports connective tissue. Very sparse community data. One EDS patient reported improved subluxation recovery.
Category
Fluid Retention
- Evidence Strength
- 4/10
- Reported Effectiveness
- 4/10
- Summary
- Known GH-class side effect. Less prominent with sermorelin than with tesamorelin or direct GH. Rarely discussed in community reports.
Category
Hair Health
- Evidence Strength
- 2/10
- Reported Effectiveness
- 4/10
- Summary
- One community mention of faster hair/nail growth. Insufficient data for meaningful scoring.
Category
Treatment Adherence
- Evidence Strength
- N/A
- Reported Effectiveness
- 6/10
- Summary
- Fasting requirement before bedtime dosing is the primary adherence challenge reported by community members.
Categories scored: 14
Categories with community data: 14
Categories not scored (insufficient data): Weight Management, Appetite & Satiety, Food Noise, Memory & Cognition, Anxiety, Stress Tolerance, Motivation & Drive, Emotional Aliveness, Emotional Regulation, Libido, Sexual Function, Inflammation, Pain Management, Gut Health, Digestive Comfort, Nausea & GI Tolerance, Heart Health, Blood Pressure, Heart Rate & Palpitations, Hormonal Symptoms, Temperature Regulation, Body Image, Immune Function, Bone Health, Longevity & Neuroprotection, Cravings & Impulse Control, Social Connection, Withdrawal Symptoms, Daily Functioning
Benefits & Potential Effects
The Basics
The benefits most reliably associated with sermorelin reflect its core action of increasing growth hormone pulses. Better sleep quality is the most consistently reported benefit, with many users noticing improvements within the first two weeks. This makes physiological sense because the largest natural growth hormone pulse occurs during deep sleep, and sermorelin administered at bedtime amplifies exactly that window.
Improved recovery from exercise is the second most commonly reported effect. People describe less soreness after workouts, faster bounce-back between training sessions, and greater exercise endurance over time. These reports align with the well-established role of growth hormone and IGF-1 in protein synthesis and tissue repair.
Some users report improvements in body composition (increased muscle definition, modest fat reduction), skin quality, energy levels, and mental clarity. These effects tend to appear more gradually, typically over 8-12 weeks of consistent use. It is worth noting that the clinical trial evidence for most of these benefits is limited. The clearest direct evidence supports GH and IGF-1 elevation and modest lean mass gains in elderly men. Many of the other reported benefits, while mechanistically plausible, have not been confirmed in controlled sermorelin-specific studies.
The Science
Supported by direct clinical evidence:
- Increased nocturnal GH secretion and serum IGF-1 elevation (P<0.05) [7]
- Increased IGFBP-3 (P<0.001) [7]
- Modest lean body mass improvement in elderly men (+1.26 kg, P<0.05) [7]
- Increased height velocity in GH-deficient children (FDA-approved indication) [1][6]
Supported by mechanism but lacking direct sermorelin trial data:
- Sleep quality improvement: GH secretion is tightly linked to slow-wave sleep architecture. MK-677 (a different GH secretagogue) demonstrated a 50% increase in Stage 4 sleep duration and >20% increase in REM sleep [11]. Sermorelin's bedtime dosing is designed to leverage this same physiological window, but no published study has directly measured sermorelin's sleep outcomes.
- Exercise recovery and tissue repair: GH and IGF-1 promote protein synthesis, collagen turnover, and angiogenesis at injury sites [3][4]. These are well-established physiological effects of the GH/IGF-1 axis.
- Cytoprotective effects: GHRH receptor activation has demonstrated neuroprotective and cardioprotective properties in preclinical models [10].
Not supported by available evidence:
- Independent fat loss: The Khorram trial found no significant change in total body fat or BMI [7].
- Bone mineral density improvement: No significant change observed in the adult trial [7].
- Functional improvements (strength, cognitive performance): The broader GH secretagogue class has struggled to demonstrate functional improvements beyond surrogate markers. MK-677's two-year trial increased lean mass but not strength [9].
Side Effects & Safety Considerations
The Basics
Sermorelin has one of the milder side effect profiles in the peptide space, which reflects both its years as an FDA-approved product and its self-limiting mechanism. The most common complaint is mild injection site reactions, such as redness, minor swelling, or tenderness, reported by roughly 1 in 6 users. These typically resolve within a day or two.
Facial flushing and a sensation of warmth after injection affect about 5-15% of users. This is usually brief, lasting minutes to an hour. Mild headaches occur in about 10% of users and generally respond to standard treatment.
An important finding from clinical use is that approximately 6.5% of patients developed subclinical hypothyroidism during treatment. Untreated hypothyroidism can blunt the GH response to sermorelin, so monitoring thyroid function is recommended during extended use.
What stands out about sermorelin's safety profile is what it does not do. At standard doses, it does not significantly elevate cortisol, ACTH, or prolactin. The somatostatin feedback brake makes it difficult to achieve dangerously high GH levels, even if you accidentally take more than intended. There are no reports of serious adverse events like acromegaly or severe hypoglycemia in the published literature at recommended dosages.
The Science
Adverse event data compiled from clinical trials and post-marketing surveillance during sermorelin's commercial availability [1][2][5][6]:
Common (>5% incidence):
- Injection site reactions: pain, erythema, swelling (15-25% of subjects); resolves within 24-48 hours
- Facial flushing/warmth: 5-15%, likely attributable to vasodilatory effects of acute GH release
Less common (1-5%):
- Headache: approximately 10%
- Nausea and altered taste: <5%
Rare (<1%):
- Dizziness, drowsiness, hyperactivity, urticaria
Metabolic considerations:
- Subclinical hypothyroidism: ~6.5% incidence in one study; monitoring of thyroid function recommended [5]
- No reports of serious acromegaly, hypoglycemia, or excessive IGF-1 elevations at recommended dosages [5]
Contraindications:
- Active malignancy (GH and IGF-1 possess mitogenic properties)
- Proliferative or severe non-proliferative diabetic retinopathy
- Critical illness with acute respiratory failure or multiple trauma
- Relative: uncontrolled diabetes mellitus (GH induces insulin resistance), pregnancy/lactation
Safety advantage of the secretagogue approach:
Treatment discontinuation due to adverse effects occurs in <5% of subjects in published trials. The somatostatin feedback mechanism provides a built-in safety margin: sermorelin cannot override the body's regulatory brake, making supraphysiological GH levels difficult to achieve [3][4]. This contrasts with exogenous rhGH, which more frequently produces fluid retention, arthralgias, and carpal tunnel syndrome.
Dosing Protocols
The Basics
Most practitioners and sources describe a once-daily bedtime injection as the standard sermorelin protocol. The timing matters because the largest natural growth hormone pulse happens during deep sleep. Injecting sermorelin 30-60 minutes before bed, on an empty stomach (at least 2 hours after eating), is designed to amplify that pulse at the optimal moment. Food intake, particularly carbohydrates, can suppress the GH response, so the fasting component is not optional for best results.
Commonly reported adult dose ranges fall between 200 and 500 mcg per day, with most sources describing a gradual titration approach: starting at 200 mcg nightly for the first two weeks, increasing by approximately 100 mcg every one to two weeks until reaching 300-500 mcg. This gradual approach allows the body to adapt and allows for IGF-1 monitoring to guide dose adjustments.
Cycle length recommendations vary. Some practitioners suggest 8-12 weeks on followed by 2-4 weeks off. Others recommend a 5-days-on, 2-days-off schedule used continuously. Pediatric trials ran 6-12 months of continuous therapy. There is no established consensus on optimal cycling for adult use; these protocols are derived from clinical practice rather than controlled dose-duration optimization studies.
The Science
Diagnostic dosing (provocative testing):
- IV bolus: 1 mcg/kg body weight (e.g., 70 mcg for a 70 kg adult)
- Serial GH sampling at baseline, 15, 30, 45, and 60 minutes post-administration
- Normal response: peak GH >10 ng/mL [2][5]
Pediatric therapeutic dosing (FDA-approved):
- 30 mcg/kg/day subcutaneously, administered before bedtime
- Treatment duration: 6-12 months in clinical trials, with some data extending to 36 months [1][6]
Adult off-label dosing (practitioner-derived):
- Range: 200-500 mcg daily subcutaneously
- Administration: Bedtime, minimum 2 hours fasted
- Titration: 200 mcg for weeks 1-2, increasing by 100 mcg every 1-2 weeks to target dose
- Target: 300-500 mcg nightly by weeks 5-8, adjusted based on IGF-1 response [5]
- Cycle: 3-6 months typical; some practitioners use 5-on-2-off schedules [5]
Combination dosing (with GH secretagogues):
- Sermorelin 200-300 mcg + Ipamorelin 200-300 mcg, or GHRP-6 100-200 mcg
- 1-2 times daily, administered simultaneously (can be mixed in same syringe)
- Co-administration produces 3-5x greater GH release than either agent alone [2][10]
Monitoring:
- IGF-1 levels at baseline and every 4-6 weeks during titration
- Fasting glucose/HbA1c (GH induces insulin resistance)
- Thyroid function (subclinical hypothyroidism incidence ~6.5%) [5]
- Lipid panel and comprehensive metabolic panel periodically
Consistency is the difference between a protocol that delivers results and one that wastes time and money. Doserly was built for exactly this: keeping you on track with the precision your protocol demands.
The built-in calculators handle the math you shouldn't be doing in your head. The reconstitution calculator tells you exactly how much bacteriostatic water to add for your target concentration. The dose calculator converts between units, milligrams, and syringe markings so you draw the right amount every time. The injection site heat map tracks where you've administered and when, helping you rotate sites systematically to reduce tissue damage, scarring, and absorption inconsistencies from overusing the same area. Pair that with smart reminders tuned to your protocol's timing requirements, and you build the kind of daily consistency that separates optimized protocols from haphazard ones.
Build reminders around the routine, not just the compound.
Doserly can keep timing, skipped doses, and schedule changes organized so the plan you read about becomes easier to follow and review.
Today view
Upcoming reminders

Reminder tracking supports consistency; it does not select a protocol for you.
What to Expect
Weeks 1-2: Sleep quality is typically the first noticeable change. Many users report deeper sleep, more vivid dreams, and waking up feeling more rested within the first week or two. Some describe being able to tell the difference in sleep quality on injection nights versus off nights. This is the most consistently reported early-onset benefit across community sources.
Weeks 2-4: Energy and recovery improvements begin to emerge. Daytime energy tends to improve, though this may be secondary to better sleep rather than a direct sermorelin effect. Recovery from workouts often becomes noticeably easier, with less soreness and faster bounce-back between training sessions. Some users report reduced brain fog and improved mental clarity during this period.
Weeks 4-8: Body composition changes may start becoming visible. Users who are exercising consistently sometimes notice improved muscle definition and fullness. Fat reduction is less predictable and often confounded by concurrent diet and exercise changes. Skin quality improvements (softness, elasticity) are occasionally reported during this timeframe but are not universal.
Weeks 8-12+: Full protocol effects accumulate. The most significant body composition and performance changes tend to manifest after 8-12 weeks of consistent use. IGF-1 levels should be measurably elevated and can be confirmed through blood work. Some practitioners recommend reassessing the protocol at this point to determine whether to continue, adjust dosing, or take an off-cycle break.
Individual variation is significant. A minority of users report minimal noticeable effects even after several weeks. Factors that influence response include age (older individuals with more significant GH decline may see more dramatic effects), baseline GH status, exercise habits, diet, sleep habits, and body composition. Sermorelin requires a functional pituitary gland to work, so individuals with pituitary damage or severe somatotroph hypoplasia are unlikely to respond.
The week-by-week expectations above are drawn from research and community reports, but your experience will be uniquely yours. Doserly's biomarker tracking transforms those general timelines into personal data points you can actually see and measure.
Log the specific markers relevant to this compound, whether that's pain levels, energy, sleep quality, body composition, recovery time, or mood, and watch your own trend lines emerge over weeks and months. Did your key markers start shifting in week three, like the research suggests? Is your experience tracking with what the community reports, or diverging? Over time, this creates something more valuable than any guide: an evidence-based picture of how your body responds to this specific compound, at your specific dose, within your specific health context.
Turn symptom and safety notes into a clearer timeline.
Doserly helps you log doses, symptoms, and safety observations side by side so patterns are easier to discuss with a qualified clinician.
Pattern view
Logs and observations
Pattern visibility is informational and should be reviewed with a clinician.
Interaction Compatibility
Good With (Synergistic)
- Ipamorelin: Preferred combination partner for GHRH/GHRP synergy. Ipamorelin provides clean GH secretagogue activity via the ghrelin receptor without elevating cortisol, prolactin, or appetite. The combination produces 3-5x greater GH release than either agent alone.
- CJC-1295: Modified GHRH analog with extended half-life. Some practitioners alternate between sermorelin and CJC-1295 rather than combining them, as both target the GHRH receptor.
- Tesamorelin: More potent GHRH analog with FDA approval for visceral fat reduction. Some practitioners use sermorelin as a lower-cost, gentler alternative when tesamorelin's full potency is not needed.
- GHRP-2: Potent ghrelin receptor agonist providing synergistic GH release. More appetite stimulation and cortisol elevation than ipamorelin.
- GHRP-6: First-generation ghrelin receptor agonist with cardioprotective properties. Significant appetite stimulation is the primary off-target effect.
- DSIP: Delta sleep-inducing peptide may extend the deep sleep window where GH pulses fire, complementing sermorelin's bedtime GH amplification.
- GHK-Cu: Tissue repair and collagen synthesis peptide that may complement sermorelin's GH-mediated regenerative effects.
- BPC-157: Healing peptide operating through distinct angiogenic mechanisms. Commonly stacked in recovery-focused protocols.
- TB-500: Thymosin beta-4 fragment with anti-inflammatory and tissue repair properties. Part of broader healing stacks that sometimes include GH secretagogues.
Not Good With (Caution)
- MK-677: Oral GH secretagogue that produces continuous 24-hour GH elevation. Combining with sermorelin may lead to excessive IGF-1 levels and is generally considered redundant rather than synergistic. Monitor IGF-1 carefully if used together.
- Hexarelin: Most potent ghrelin receptor agonist but demonstrates tachyphylaxis (reduced effectiveness) with chronic use. Less predictable in combination protocols.
- IGF-1 LR3: Direct IGF-1 analog that bypasses GH axis entirely. Combining with GH secretagogues may lead to excessive IGF-1 levels with increased mitogenic risk.
- Exogenous Growth Hormone (rhGH): Combining sermorelin with direct GH injection is generally considered unnecessary and counterproductive, as rhGH suppresses endogenous pituitary GH production that sermorelin is trying to stimulate.
Administration Guide
Materials required:
- Reconstituted sermorelin vial
- U-100 insulin syringe (0.3-0.5 mL with 28G-31G needle, 5/16 to 1/2 inch length)
- Alcohol swabs (one for vial stopper, one for injection site)
- Sharps disposal container
Recommended reconstitution solution:
Bacteriostatic water (containing 0.9% benzyl alcohol as preservative) is the standard reconstitution solution. For a 10 mg vial, adding 3.0 mL of bacteriostatic water produces a concentration of approximately 3.33 mg/mL, which allows convenient measurement using U-100 insulin syringe markings (1 unit = approximately 33.3 mcg). For a 5 mg vial, 3.0 mL produces approximately 1.67 mg/mL. Do not use bacteriostatic water if allergic to benzyl alcohol; sterile water for injection is an alternative but limits the reconstituted vial to single-use.
Timing considerations:
- Administer 30-60 minutes before bedtime to align with the natural nocturnal GH pulse
- Minimum 2 hours fasted; avoid high-carbohydrate meals before injection as insulin spikes can blunt the GH response
- Consistency in timing helps establish predictable GH pulsatility
Post-administration care:
- Apply gentle pressure with cotton ball at injection site; do not rub
- Mild injection site redness or tenderness is common (~17% incidence) and typically resolves within 24-48 hours
- Transient facial flushing may occur within minutes of injection; this is normal and resolves quickly
- Contact a healthcare provider if severe injection site reactions, persistent swelling, or signs of infection develop
Supplies & Planning
Peptide vials:
Sermorelin is commonly available in 5 mg and 10 mg lyophilized vials through compounding pharmacies. Having an extra vial on hand as backup is recommended in case of spillage during reconstitution.
Insulin syringes:
U-100 insulin syringes with 28G-31G needles in 5/16 to 1/2 inch lengths are standard for subcutaneous peptide injection. For doses below 10 units (0.10 mL), consider 30-unit or 50-unit insulin syringes for improved measurement precision. One syringe per injection; never reuse syringes.
Bacteriostatic water:
Available in 10 mL and 30 mL vials. Each reconstitution uses approximately 3.0 mL. A single 10 mL vial provides enough for 3 reconstitutions.
Alcohol swabs:
Two per injection day (one for the vial stopper, one for the injection site). Purchase in 100-count boxes.
Sharps container:
One puncture-proof disposal container for safe disposal of used syringes and needles.
General planning note:
Specific quantities of vials and supplies depend on the dose, frequency, and cycle duration prescribed by a healthcare provider. The reconstitution calculator can help determine the exact preparation specifications for your prescribed concentration. Consult with a healthcare provider to determine the appropriate protocol for your specific needs.
Storage & Handling
Lyophilized (powder) form:
- Refrigerate at 2-8C (36-46F) for short to medium-term storage
- For long-term storage (months), -20C or colder is recommended
- Protect from light and moisture
- Store in original sealed packaging with desiccant when possible
- Do not freeze the dry powder at standard refrigerator temperatures (it is already dry and stable)
- Allow vials to reach room temperature (10-30 minutes) before reconstituting to prevent condensation inside the vial
Reconstituted (liquid) form:
- Refrigerate immediately at 2-8C (36-46F) after reconstitution
- Use within 10-14 days when reconstituted with bacteriostatic water (multi-dose vial)
- Do not freeze reconstituted solution (freezing denatures the peptide)
- Inspect solution before each use; it should be clear and colorless with no cloudiness, particles, or discoloration
- Discard if any visual abnormalities are observed
- Swab vial stopper with alcohol before each withdrawal
- Label the vial with the reconstitution date
General handling:
- Use aseptic technique for all vial access
- Avoid repeated temperature fluctuations
- Keep vials away from direct sunlight, heaters, and excessive heat
Lifestyle Factors
Sleep optimization:
Prioritize 7-9 hours of uninterrupted sleep nightly. Sermorelin's primary mechanism leverages the natural nocturnal GH pulse, so optimizing sleep conditions (cool, dark environment; consistent bedtime; minimized screen exposure before sleep) directly supports its effectiveness.
Exercise:
Resistance training 3-5 times per week is commonly recommended alongside GH secretagogue protocols. Exercise itself stimulates GH release, and the combination with sermorelin may produce additive effects on body composition and recovery. Moderate aerobic activity complements the metabolic benefits.
Nutrition:
Adequate protein intake (commonly cited range: 1.6-2.2 g/kg/day) supports the anabolic processes stimulated by GH/IGF-1 elevation. Avoid high-carbohydrate meals within 2 hours of injection, as the resulting insulin spike can blunt GH release. Some practitioners recommend a protein-focused diet with carbohydrates timed away from the injection window.
Fasting compliance:
The fasting requirement before injection is the most commonly cited adherence challenge. Plan dinner early enough to allow at least 2 hours before the bedtime injection. Some users who struggle with this timing take sermorelin if they wake during the night, when they are naturally in a fasted state.
Stress management:
Chronic elevated cortisol suppresses GH secretion. Stress-reduction practices (meditation, adequate rest, workload management) support GH axis responsiveness.
Avoid alcohol and smoking:
Both impair GH release and may blunt the sermorelin response.
Regulatory Status & Research Classification
United States (FDA):
Sermorelin acetate was FDA-approved in 1997 under the brand name Geref for the diagnosis and treatment of idiopathic growth hormone deficiency in children. The manufacturer (EMD Serono) voluntarily withdrew Geref from the commercial market in 2008 due to manufacturing economics and declining market demand, not safety concerns. The compound is currently available through FDA-registered compounding pharmacies under Section 503A of the Federal Food, Drug, and Cosmetic Act, which permits compounding of previously FDA-approved bulk drug substances with a valid patient-specific prescription. This gives sermorelin the most defensible legal position of any GH secretagogue in the compounding space.
Canada (Health Canada):
Sermorelin does not hold a Drug Identification Number (DIN) in Canada. Access may be available through compounding pharmacies or special access programs at the discretion of prescribing physicians.
United Kingdom (MHRA):
Sermorelin is not listed as an approved medicine by the MHRA. It may be available through specialist clinics or compounding pharmacies under practitioner supervision.
Australia (TGA):
Sermorelin is not separately listed on the Australian Register of Therapeutic Goods. Growth hormone secretagogues may fall under Schedule 4 (prescription only) or require Special Access Scheme authorization.
European Union (EMA):
No centralized marketing authorization exists for sermorelin from the EMA. Availability varies by member state through compounding or specialist channels.
WADA status:
Sermorelin is prohibited by the World Anti-Doping Agency as a growth hormone secretagogue. Athletes subject to WADA-governed testing should be aware that use may result in a positive test and sanctions.
Active clinical trials:
No active clinical trials for sermorelin are currently listed on ClinicalTrials.gov as of March 2026. The compound's clinical development has effectively ceased in favor of newer GHRH analogs (tesamorelin, CJC-1295) and direct GH products.
Regulatory status changes frequently. Always verify the current legal status of any compound in your specific country or jurisdiction before making any decisions.
FAQ
What is the difference between sermorelin and growth hormone (HGH)?
Sermorelin stimulates your pituitary gland to produce and release its own growth hormone, preserving natural pulsatile secretion and somatostatin feedback regulation. Recombinant human growth hormone (rhGH) is the hormone itself injected directly, bypassing the pituitary entirely. The practical consequence is that rhGH can produce supraphysiological GH levels because it ignores the body's brake system, while sermorelin's effects are self-limiting.
How long does it take to notice effects?
Based on available community reports and clinical practice observations, sleep quality improvements are often the first noticeable change, with many users reporting better sleep within 1-2 weeks. Energy and recovery improvements typically follow at 2-4 weeks. Body composition changes generally require 8-12 weeks of consistent use. Individual response varies significantly based on age, baseline GH status, lifestyle factors, and protocol adherence.
Does sermorelin cause fat loss?
The only controlled adult trial (Khorram 1997, N=19) found no significant change in body fat. Community reports of fat loss are common but heavily confounded by concurrent diet changes, exercise, and co-administration of other compounds (particularly GLP-1 agonists). Sermorelin may support fat metabolism indirectly through GH/IGF-1 elevation, but an independent fat-reducing effect has not been established in clinical research.
Is sermorelin still legal?
In the United States, sermorelin is available by prescription through licensed compounding pharmacies under the 503A framework. Its prior FDA approval gives it the strongest legal footing of any GH secretagogue in the compounding space. A valid prescription from a licensed healthcare provider is required. Regulatory status varies by country.
Can sermorelin be taken long-term?
Long-term adult safety data are limited. The longest adult trial was 16 weeks. Clinical practice commonly employs cycling protocols (8-12 weeks on, 2-4 weeks off), though these are derived from practitioner experience rather than published optimization studies. Periodic IGF-1 monitoring is recommended during extended use to confirm levels remain within a physiological range.
Why does sermorelin need to be taken on an empty stomach?
Food intake, particularly carbohydrates, triggers insulin release. Elevated insulin suppresses GH secretion and can blunt the pituitary's response to sermorelin. Maintaining a fasted state for at least 2 hours before injection helps ensure an optimal GH response.
How does sermorelin compare to CJC-1295 and ipamorelin?
CJC-1295 (without DAC) is a modified GHRH analog with slightly longer half-life than sermorelin but no published human body composition trials. Ipamorelin is a ghrelin-receptor agonist (different mechanism) often combined with GHRH analogs for synergistic GH release. Sermorelin has the advantage of prior FDA approval and the longest safety record, while newer compounds offer structural modifications for extended activity. Healthcare providers can help determine which approach best fits individual goals and medical history.
Sources & References
Clinical Trials and Reviews:
[1] Prakash A, Goa KL. "Sermorelin: a review of its use in the diagnosis and treatment of children with idiopathic growth hormone deficiency." BioDrugs. 2004;18(5):339-354. https://pubmed.ncbi.nlm.nih.gov/18031173/
[2] NCBI Bookshelf. "Growth Hormone Deficiency." NBK279056. Additional pharmacokinetic data from RxList Sermorelin Acetate Injection Monograph and Mayo Clinic Sermorelin (injection route) reference.
[3] Walker RF. "Sermorelin: A better approach to management of adult-onset growth hormone insufficiency?" Clinical Interventions in Aging. 2006;1(4):307-308. https://pmc.ncbi.nlm.nih.gov/articles/PMC2699646/
[4] Bowers CY et al. "On the actions of the growth hormone-releasing hexapeptide, GHRP." Endocrinology. 1994;79:940-942.
[5] RxList. Sermorelin Acetate Prescribing Information. Adverse effects, dosing, and thyroid monitoring data.
[6] Keating GM, Wellington K. "Sermorelin: a review of its use in the diagnosis and treatment of children with idiopathic GHD." BioDrugs. 2004;18(5):339-354.
[7] Khorram O et al. "Endocrine and metabolic effects of long-term administration of [Nle27]GHRH-(1-29)-NH2 in age-advanced men and women." Journal of Clinical Endocrinology & Metabolism. 1997;82(5):1472-1479. https://pubmed.ncbi.nlm.nih.gov/9141536/
[8] Falutz J et al. "Effects of tesamorelin in HIV-infected patients with excess abdominal fat: pooled Phase 3 analysis." Journal of Clinical Endocrinology & Metabolism. 2010;95(9):4291-4304. https://pubmed.ncbi.nlm.nih.gov/20554713/
[9] Nass R et al. "Effects of an Oral Ghrelin Mimetic on Body Composition and Clinical Outcomes in Healthy Older Adults." Annals of Internal Medicine. 2008. https://pmc.ncbi.nlm.nih.gov/articles/PMC2757071/
[10] Sigalos JT, Pastuszak AW. "The Safety and Efficacy of Growth Hormone Secretagogues." Sexual Medicine Reviews. 2018;6(1):45-53. https://pmc.ncbi.nlm.nih.gov/articles/PMC5632578/
[11] Copinschi G et al. "Effects of a 7-day treatment with a novel, orally active, growth hormone (GH) secretagogue, MK-677, on 24-hour GH profiles, insulin-like growth factor I, and adrenocortical function in normal young men." Journal of Clinical Endocrinology & Metabolism. 1996;81(8):2776-2782.
Animal and Mechanistic Studies:
[12] Sinha DK et al. "Beyond the androgen receptor: the role of growth hormone secretagogues in the modern management of body composition in hypogonadal males." Translational Andrology and Urology. 2020;9(Suppl 2):S149-S159. https://pmc.ncbi.nlm.nih.gov/articles/PMC7108996/
[13] Vittone J, Blackman MR, Busby-Whitehead J, et al. "Effect of Sermorelin on Body Composition in Adults." JAMA. 1997. DOI: 10.1001/jama.1997.03540480040032
Related Peptide Guides
- Ipamorelin — Selective GH secretagogue; preferred combination partner for GHRH/GHRP synergy
- CJC-1295 — Modified GHRH analog with extended half-life
- Tesamorelin — FDA-approved GHRH analog with visceral fat reduction data
- GHRP-2 — Potent ghrelin receptor agonist for GH secretion
- GHRP-6 — First-generation ghrelin receptor agonist with cardioprotective properties
- MK-677 — Oral GH secretagogue with 24-hour activity
- DSIP — Delta sleep-inducing peptide complementary to bedtime GH protocols
- GHK-Cu — Tissue repair peptide commonly stacked with GH secretagogues
- BPC-157 — Healing peptide with complementary angiogenic mechanisms
- TB-500 — Thymosin beta-4 fragment for tissue repair and recovery
- Hexarelin — Most potent ghrelin receptor agonist (note: tachyphylaxis risk)
Need the reconstitution math for Sermorelin: Complete Research Guide?
Open the calculator with Sermorelin: Complete Research Guide prefilled to estimate concentration, draw volume, and related measurement math from the reconstitution details you already have.