IGF-1 LR3: Complete Research Guide
On this page
Quick Reference Card
Attribute
Also Known As
- Detail
- Long R3 IGF-1, LR3 IGF-1, Long Arg3 IGF-1, Insulin-like Growth Factor 1 Long Arg3
Attribute
Administration
- Detail
- Injectable (subcutaneous or intramuscular)
Attribute
Research Status
- Detail
- Research Compound. No FDA approval for human therapeutic use. WADA prohibited (classified as peptide hormone/growth factor analog).
Attribute
Typical Dose Range
- Detail
- 20-50 mcg per day subcutaneously (commonly reported range; no clinically validated human dosing protocol exists)
Attribute
Half-Life
- Detail
- 20-30 hours (compared to 12-15 hours for native IGF-1)
Attribute
Cycle Length
- Detail
- 4-8 weeks on, 4-8 weeks off (varies by source)
Attribute
Storage
- Detail
- Lyophilized: -20°C (-4°F) for up to 12 months; Reconstituted: 2-8°C (35.6-46.4°F), use within 30 days
Overview / What Is IGF-1 LR3?
The Basics
IGF-1 LR3 is a synthetic, modified version of insulin-like growth factor 1 (IGF-1), a hormone your body naturally produces in the liver in response to growth hormone. Think of natural IGF-1 as the messenger that carries out many of growth hormone's effects: telling cells to grow, divide, and repair themselves. The problem with natural IGF-1 is that it gets quickly captured by binding proteins in the blood, limiting how long it can actually work.
IGF-1 LR3 was engineered to solve that problem. By adding 13 extra amino acids to the front of the molecule and swapping one amino acid at position 3, scientists created a version that slips past those binding proteins. The result is a compound that stays active in the body roughly 120 times longer than natural IGF-1 and delivers approximately three times the biological potency at comparable doses.
This makes IGF-1 LR3 one of the most powerful growth-promoting peptides available in research contexts. It has attracted interest for its potential to promote muscle cell growth, enhance recovery, improve nutrient partitioning (directing calories toward muscle rather than fat), and support tissue repair. However, that same potency is a double-edged sword. The compound carries notable safety concerns including hypoglycemia risk, potential cancer-promoting effects from stimulating cell growth indiscriminately, and the inability to monitor its levels through standard bloodwork. No clinical trials have been conducted with IGF-1 LR3 in humans, and it has never received regulatory approval for any therapeutic use.
The Science
IGF-1 LR3 (Long R3 Insulin-like Growth Factor-1) is a recombinant analog of human IGF-1, consisting of 83 amino acids with a 13-amino-acid N-terminal extension and an arginine substitution at position 3 (replacing glutamic acid) [1]. These structural modifications dramatically reduce binding affinity to the six known insulin-like growth factor binding proteins (IGFBP-1 through IGFBP-6), which normally sequester approximately 99% of circulating IGF-1 [2].
The reduced IGFBP binding results in markedly enhanced bioavailability and a circulating half-life of approximately 20-30 hours, compared to 12-15 hours for unmodified IGF-1 and only minutes for the unbound free fraction [1][3]. In functional assays, IGF-1 LR3 demonstrates approximately three-fold greater potency than native IGF-1 in stimulating cell proliferation and protein synthesis [4].
IGF-1 LR3 activates the IGF-1 receptor (IGF-1R), a transmembrane tyrosine kinase receptor, and to a lesser extent insulin receptor isoforms. Receptor binding triggers two primary intracellular signaling cascades: the PI3K-AKT-mTOR pathway (driving protein synthesis, cell survival, and glucose uptake) and the RAS-MAPK pathway (promoting cell proliferation and differentiation) [5]. Downstream effects include satellite cell activation, myoblast proliferation, and enhanced anabolic signaling across multiple tissue types including muscle, bone, liver, kidney, nerve, and skin [4][6].
Unlike native IGF-1, which requires GH-mediated hepatic production and is tightly regulated through IGFBP sequestration, IGF-1 LR3 delivers sustained, supraphysiological IGF-1R activation that bypasses endogenous regulatory mechanisms. This property underlies both its research utility and its safety concerns.
Molecular Identity
Attribute
Common Names
- Detail
- IGF-1 LR3, Long R3 IGF-1, LR3 IGF-1, Insulin-like Growth Factor 1 Long Arg3
Attribute
Amino Acid Sequence
- Detail
- MFPAMPLSSL FVNGPRTLCG AELVDALQFV CGDRGFYFNK PTGYGSSSRR APQTGIVDEC CFRSCDLRRL EMYCAPLKPA KSA (83 amino acids)
Attribute
Molecular Formula
- Detail
- C₄₀₀H₆₂₅N₁₁₁O₁₁₅S₉
Attribute
Molecular Weight
- Detail
- 9117.5 g/mol (~9.7 kDa)
Attribute
CAS Number
- Detail
- 946870-92-4
Attribute
Key Modifications
- Detail
- 13-amino-acid N-terminal extension + Glu→Arg substitution at position 3
Attribute
Functional Class
- Detail
- IGF-1 receptor agonist, growth factor analog
Attribute
Salt Forms
- Detail
- Lyophilized powder (free peptide or acetate salt)
Mechanism of Action
The Basics
Your body uses a relay system for growth and repair. Growth hormone (GH) is released by the pituitary gland and travels to the liver, where it triggers the production of IGF-1. IGF-1 is the molecule that actually does the building work, telling cells throughout your body to grow, divide, and repair themselves. Think of GH as the manager issuing orders and IGF-1 as the construction crew executing them.
Under normal circumstances, most of the IGF-1 in your blood is bound up by carrier proteins (IGFBPs) that regulate how much is free and active at any given time. This keeps the growth signals carefully controlled. IGF-1 LR3 bypasses this control system almost entirely. Because of its structural modifications, it barely sticks to those carrier proteins, so it circulates freely and keeps activating growth receptors for far longer than the natural version.
When IGF-1 LR3 reaches a cell, it locks onto IGF-1 receptors on the cell surface and flips the switch on two major growth pathways. One pathway (PI3K-AKT-mTOR) drives protein synthesis, essentially telling the cell to build more muscle protein and take up more glucose and amino acids. The other pathway (RAS-MAPK) drives cell division, creating entirely new cells rather than just enlarging existing ones. This distinction between making cells bigger (hypertrophy) and making more cells (hyperplasia) is one of the features that distinguishes IGF-1 LR3 from many other anabolic compounds [4].
The important caveat is that this growth signaling is not selective. IGF-1 LR3 does not distinguish between muscle cells, organ cells, or potentially precancerous cells. It promotes growth across all cell types that carry the IGF-1 receptor, which is why safety monitoring is such a critical consideration.
The Science
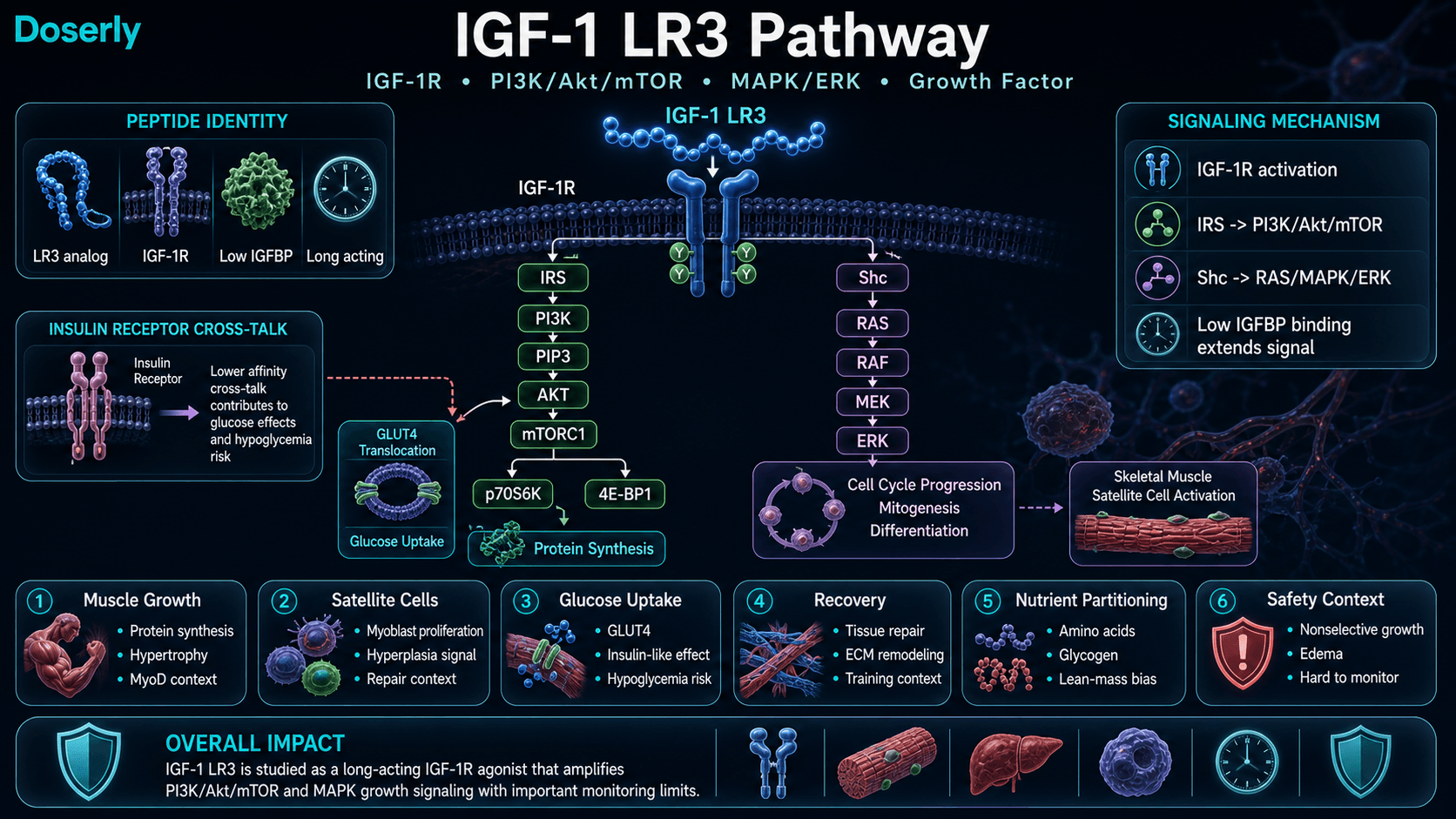
IGF-1 LR3 functions as a potent agonist of the type 1 insulin-like growth factor receptor (IGF-1R), a heterotetrameric transmembrane receptor tyrosine kinase expressed across virtually all mammalian cell types [5]. Upon ligand binding, IGF-1R undergoes autophosphorylation of intracellular tyrosine residues, recruiting insulin receptor substrate (IRS) proteins and Shc adaptor proteins to initiate two principal signaling cascades:
PI3K-AKT-mTOR Pathway: IRS recruitment activates phosphatidylinositol 3-kinase (PI3K), generating PIP₃ and activating protein kinase B (AKT/PKB). AKT subsequently activates mechanistic target of rapamycin complex 1 (mTORC1), which phosphorylates p70S6K and 4E-BP1 to upregulate cap-dependent translation and protein synthesis [5]. This pathway also promotes glucose transporter (GLUT4) translocation, enhancing cellular glucose uptake, which partially explains the insulin-like hypoglycemic effects observed with IGF-1 analogs [7].
RAS-MAPK Pathway: Shc recruitment activates the RAS-RAF-MEK-ERK cascade, promoting cell cycle progression, mitogenesis, and cellular differentiation [5]. In skeletal muscle, this pathway activates satellite cells and drives myoblast proliferation, supporting the hyperplastic (new cell formation) component of muscle growth [4][6].
In mouse models of Duchenne muscular dystrophy (DMD), IGF-1 LR3 and related IGF-1 derivatives have been shown to counteract myostatin (GDF-8) signaling and prevent apoptosis through activation of the myogenic differentiation factor MyoD [6]. IGF-1 LR3 also binds the insulin receptor with lower affinity than the IGF-1R, contributing to its effects on glucose metabolism and lipid handling [7].
A critical pharmacological distinction: standard clinical assays for total IGF-1 (immunoassay or LC-MS/MS) do not reliably distinguish exogenous LR3 from endogenous IGF-1, and IGFBP displacement can artifactually alter measured values. Free IGF-1 and IGFBP-3 correlate poorly with LR3 exposure. No commercially available functional bioassay exists for clinical monitoring of IGF-1 LR3 pharmacodynamics [8].
Pathway Visualization Image
Pharmacokinetics
The Basics
The defining pharmacokinetic feature of IGF-1 LR3 is its dramatically extended half-life compared to natural IGF-1. Where the active (unbound) fraction of natural IGF-1 lasts only minutes in the bloodstream, IGF-1 LR3 remains active for approximately 20-30 hours. Some sources describe it as staying active up to 120 times longer than natural IGF-1 [4]. This extended duration is what allows once-daily dosing rather than the frequent administration that would be needed with unmodified IGF-1.
This long activity window means that a single morning injection can maintain elevated IGF-1R signaling throughout the entire day and into the following morning. It also means that the compound accumulates somewhat with daily dosing, reaching steady-state levels within a few days of consistent administration.
The extended half-life comes directly from the structural modifications that prevent binding proteins from capturing the molecule. Normally, IGFBPs serve as a reservoir and buffer system, binding up IGF-1 and then slowly releasing it. With IGF-1 LR3, this buffer is largely bypassed, resulting in higher sustained free concentrations but also less of the natural "pulsatile" delivery pattern.
The Science
The pharmacokinetics of IGF-1 LR3 are primarily determined by its reduced IGFBP binding affinity. Native IGF-1 exists in three circulating pools: the ternary complex with IGFBP-3 and ALS (approximately 75%, half-life 12-15 hours), binary complexes with other IGFBPs (approximately 20%, half-life 20-30 minutes), and unbound free IGF-1 (less than 1%, half-life approximately 10-12 minutes) [2].
IGF-1 LR3 predominantly circulates in the unbound form due to its reduced IGFBP affinity, yet achieves a functional half-life of approximately 20-30 hours [1][3]. This apparent paradox is explained by the peptide's altered tissue distribution and slower renal clearance relative to its molecular weight compared to the small free IGF-1 fraction.
Administration is typically via subcutaneous injection, with systemic distribution confirmed in research models. The compound demonstrates systemic activity rather than primarily local effects, distinguishing it from IGF-1 DES (des(1-3)IGF-1), which has a much shorter half-life and is sometimes used for localized effects [1].
Once-daily administration maintains relatively stable plasma levels throughout the dosing interval. At standard reported doses of 20-50 mcg/day subcutaneously, steady-state conditions are expected to be reached within 3-5 days of consistent daily administration [3].
Research & Clinical Evidence
The Basics
It is important to be upfront about the evidence base: there are no published clinical trials of IGF-1 LR3 in humans. The available research comes from animal studies, cell culture (in vitro) experiments, and extrapolation from studies of native IGF-1 and the FDA-approved IGF-1 analog mecasermin (Increlex). Community experience reports supplement this preclinical data, but they are anecdotal and uncontrolled.
IGF-1 LR3 and Muscle Growth
The Basics
The strongest area of research interest for IGF-1 LR3 is muscle growth. In cell culture and animal studies, IGF-1 LR3 has been shown to stimulate both the growth of existing muscle fibers and the creation of entirely new muscle cells through satellite cell activation. This makes it distinct from many anabolic compounds that primarily enlarge existing fibers. Animal research also suggests that IGF-1 LR3 can counteract myostatin, a protein that naturally limits muscle growth, by activating a competing pathway through MyoD [6].
The Science
In vitro studies demonstrate that IGF-1 LR3 activates satellite cell proliferation and myoblast differentiation through the PI3K-AKT-mTOR and MAPK signaling cascades [4][5]. In mouse models of DMD, IGF-1 derivatives including LR3 counteracted myostatin-mediated muscle wasting by activating MyoD-dependent myogenic programs and suppressing apoptotic signaling [6].
Philippou et al. (2007, 2009) characterized the role of IGF-1 isoforms in skeletal muscle physiology, demonstrating that mechanical loading activates IGF-1 signaling cascades that drive both hypertrophic and hyperplastic responses [9][10]. While these studies examined endogenous IGF-1 rather than the LR3 variant specifically, the receptor-level mechanism is conserved.
The potency advantage of LR3 over native IGF-1 has been quantified at approximately 3-fold in cell proliferation assays, attributable to its reduced IGFBP sequestration and prolonged receptor occupancy [4].
IGF-1 LR3 and Wound Healing / Tissue Repair
The Basics
IGF-1 LR3 has drawn attention for its potential to accelerate tissue repair. The same cell growth signaling that drives muscle development also supports healing in tendons, ligaments, and other connective tissues. Research in animal models suggests that IGF-1 signaling promotes new blood vessel formation and cell migration toward damaged tissue, processes that are essential for recovery from injury [11].
The Science
IGF-1 signaling plays a central role in tissue repair across multiple organ systems. In nerve injury models, IGF-1 has been identified as a promising therapeutic target for peripheral nerve repair, promoting Schwann cell proliferation and axonal regeneration [11]. Jonker et al. (2020) demonstrated that IGF-1 stimulates coronary vascular growth matching cardiac growth in fetal sheep models, confirming angiogenic effects [12].
White et al. (2025) studied IGF-1 LR3 specifically in late-gestation growth-restricted fetal sheep and found that LR3 did not promote growth in this context, suggesting that the compound's effects may be context-dependent and not universally growth-promoting [13].
IGF-1 LR3 and Metabolic Effects
The Basics
IGF-1 LR3 shares structural similarity with insulin, and that similarity extends to some metabolic effects. It can increase glucose uptake into muscle and liver cells, which lowers blood sugar levels. While this could theoretically benefit blood sugar management, it is also the source of one of the compound's most immediate safety concerns: hypoglycemia [7]. Some animal research suggests that IGF-1 derivatives can reduce insulin requirements by approximately 10%, but this has not been studied with LR3 in humans.
The Science
IGF-1 LR3 binds the insulin receptor (IR) with lower affinity than IGF-1R but sufficient to produce insulin-mimetic metabolic effects [7]. These include GLUT4-mediated glucose uptake in skeletal muscle and hepatocytes, glycogen synthesis stimulation, and suppression of hepatic gluconeogenesis. In animal models, IGF-1 administration has been shown to reduce circulating insulin levels and improve insulin sensitivity [7].
The dual IGF-1R/IR activation also drives nutrient partitioning effects, directing glucose and amino acid uptake preferentially toward skeletal muscle over adipose tissue. This metabolic shift, combined with lipolytic effects mediated through reduced insulin levels, underlies the body recomposition effects reported in community use [4].
Biomarker Evidence Matrix
Category
Muscle Growth
- Evidence Strength
- 5/10
- Reported Effectiveness
- 6/10
- Summary
- Strong in vitro and animal model evidence for hyperplasia and satellite cell activation. No human clinical data. Community reports positive but modest muscle gains at 20-50 mcg/day.
Category
Recovery & Healing
- Evidence Strength
- 5/10
- Reported Effectiveness
- 7/10
- Summary
- Animal models support tissue repair mechanisms. Community reports notably positive for recovery and injury healing. Strongest community signal category.
Category
Physical Performance
- Evidence Strength
- 3/10
- Reported Effectiveness
- 6/10
- Summary
- Limited direct evidence; mechanism supports enhanced performance through IGF-1R signaling. Anecdotal reports of improved endurance.
Category
Fat Loss
- Evidence Strength
- 4/10
- Reported Effectiveness
- 5/10
- Summary
- Indirect fat metabolism effects through insulin-receptor crosstalk and nutrient partitioning. Community reports mixed, confounded by concurrent diet and exercise.
Category
Weight Management
- Evidence Strength
- 3/10
- Reported Effectiveness
- 5/10
- Summary
- Body recomposition effects reported anecdotally. Mechanism supports nutrient partitioning toward lean mass.
Category
Side Effect Burden
- Evidence Strength
- 5/10
- Reported Effectiveness
- 4/10
- Summary
- Known insulin-like hypoglycemic effects. Animal data on organ growth risk. Community cautionary consensus. Inability to monitor via standard bloodwork.
Category
Energy Levels
- Evidence Strength
- 2/10
- Reported Effectiveness
- 5/10
- Summary
- No direct evidence. Indirectly referenced through community endurance reports.
Category
Joint Health
- Evidence Strength
- 3/10
- Reported Effectiveness
- 5/10
- Summary
- Mixed: tissue repair mechanism may aid joint healing, but edema and arthralgia are reported side effects.
Category
Skin Health
- Evidence Strength
- 2/10
- Reported Effectiveness
- 4/10
- Summary
- Cell proliferation mechanism theoretically supports tissue repair. Single anecdotal report of gum tissue regrowth.
Category
Fluid Retention
- Evidence Strength
- 4/10
- Reported Effectiveness
- 5/10
- Summary
- Edema is a well-documented side effect of IGF-1 signaling. Consistent across sources.
Category
Nausea & GI Tolerance
- Evidence Strength
- 3/10
- Reported Effectiveness
- 4/10
- Summary
- Nausea and fatigue noted in safety profiles. Limited community data.
Category
Longevity & Neuroprotection
- Evidence Strength
- 4/10
- Reported Effectiveness
- 3/10
- Summary
- Paradox: short-term neuroprotective effects but chronically elevated IGF-1 is associated with increased all-cause mortality and cancer risk.
Categories scored: 12
Categories with community data: 12
Categories not scored (insufficient data): Sleep Quality, Focus & Mental Clarity, Memory & Cognition, Mood & Wellbeing, Anxiety, Stress Tolerance, Motivation & Drive, Emotional Aliveness, Emotional Regulation, Libido, Sexual Function, Inflammation, Pain Management, Gut Health, Digestive Comfort, Hair Health, Heart Health, Blood Pressure, Heart Rate & Palpitations, Hormonal Symptoms, Temperature Regulation, Body Image, Immune Function, Bone Health, Cravings & Impulse Control, Social Connection, Treatment Adherence, Withdrawal Symptoms, Daily Functioning, Appetite & Satiety, Food Noise, Other
Benefits & Potential Effects
The Basics
IGF-1 LR3 offers a range of potential benefits that stem from its ability to amplify the body's natural growth and repair signaling. The most commonly discussed benefits include enhanced muscle growth and recovery, improved nutrient partitioning, and support for tissue repair after injury. However, it is essential to keep perspective: these benefits are based primarily on animal research and community anecdotes rather than controlled human clinical trials.
Muscle growth is the primary reason most people investigate this compound. Unlike many peptides that work indirectly by stimulating growth hormone release, IGF-1 LR3 acts directly on muscle cells. It promotes both the enlargement of existing muscle fibers and, uniquely, the creation of entirely new muscle cells through a process called hyperplasia [4]. This dual mechanism is one of the features that distinguishes it in the peptide landscape.
Recovery and tissue repair represent another area of notable community interest. Users report faster recovery between training sessions, reduced muscle soreness, and in some cases accelerated healing of injuries. The underlying mechanism, enhanced cell division and tissue regeneration, is well-supported by preclinical research.
Nutrient partitioning effects, where the body directs more calories toward muscle and less toward fat storage, are frequently cited. This is mediated through IGF-1 LR3's effects on both IGF-1 receptors and insulin receptors, influencing how the body handles glucose and amino acids.
The Science
The benefits profile of IGF-1 LR3 derives from sustained IGF-1R activation and downstream effects on the PI3K-AKT-mTOR and RAS-MAPK pathways [5]:
Anabolic effects: Enhanced protein synthesis via mTORC1 activation, satellite cell proliferation, and MyoD-mediated myogenic differentiation. In cell culture, IGF-1 LR3 demonstrates approximately 3x the potency of native IGF-1 for stimulating cell proliferation [4].
Anti-catabolic effects: IGF-1 signaling counteracts myostatin (GDF-8) activity, protecting against muscle wasting. In DMD mouse models, IGF-1 derivatives prevented apoptosis and maintained muscle fiber integrity [6]. Additionally, research suggests potential for counteracting glucocorticoid-induced muscle wasting, as IGF-1 signaling opposes the catabolic effects of cortisol [14].
Metabolic effects: Dual IGF-1R/IR activation enhances GLUT4-mediated glucose uptake, promotes glycogen synthesis, and drives nutrient partitioning toward lean tissue. This produces a net effect of reduced adipose tissue and enhanced anabolism [7].
Tissue repair: IGF-1 signaling promotes angiogenesis, fibroblast migration, and extracellular matrix remodeling at injury sites. IGF-1 has been identified as a promising therapeutic target for peripheral nerve injury repair [11].
The benefits outlined above span multiple body systems, and your experience will be uniquely yours. Rather than guessing which effects are attributable to this compound versus other factors in your life, Doserly helps you log specific outcomes alongside your protocol details, building a clear picture of what's changing and when.
Over weeks and months, this creates something more useful than any anecdotal report: your own evidence-based record of how this compound affects you personally, at your specific dose, within the context of your full health protocol. When it's time to decide whether to continue, adjust, or discontinue, you have real data to inform that conversation with your healthcare provider.
Keep sensitive protocol records in a purpose-built app.
Doserly is designed for private health tracking with structured records, offline-ready workflows, and exportable history when you need it.
Privacy
Health records

Privacy controls help you manage records; keep clinical records where required.
Side Effects & Safety Considerations
The Basics
IGF-1 LR3 carries a more significant safety profile than many commonly discussed peptides. It is important to understand these risks clearly, because the same potency that makes it effective also makes it potentially dangerous without proper medical oversight.
Hypoglycemia (low blood sugar) is the most immediate and commonly reported concern. Because IGF-1 LR3 increases glucose uptake into cells similarly to insulin, it can drop blood sugar levels quickly, especially when taken on an empty stomach or at higher doses. Symptoms include shakiness, dizziness, sweating, confusion, and in severe cases, loss of consciousness. Most sources recommend administering with or shortly after food and keeping fast-acting carbohydrates (glucose tablets, juice) readily available during any protocol [3].
Edema and water retention are frequently reported side effects. This can manifest as puffiness in the face, hands, or extremities, and may contribute to joint discomfort or carpal tunnel-like symptoms [8].
Cancer risk is the most serious long-term concern. IGF-1 LR3 promotes growth across all cell types, including potentially precancerous cells. It also has anti-apoptotic effects, meaning it can prevent damaged cells from undergoing programmed cell death when they normally would. Chronically elevated IGF-1 signaling is associated with increased risk of prostate, breast, and colorectal cancers [15]. This is a theoretical but well-supported risk that multiple expert sources emphasize strongly.
Organ growth with prolonged use is another theoretical concern. Chronic supraphysiological IGF-1 signaling could potentially lead to organ enlargement (organomegaly) and acromegaloid features, similar to conditions seen with excess growth hormone production.
Unmonitorable is a practical concern that distinguishes IGF-1 LR3 from many other compounds. Standard laboratory tests for total IGF-1, free IGF-1, and IGFBP-3 do not reliably reflect LR3 exposure or its pharmacodynamic effects. No commercially available clinical assay can quantify LR3 specifically, which means dose-response and safety cannot be managed to a medical standard through routine bloodwork [8].
The Science
Hypoglycemia: The insulin-mimetic activity of IGF-1 LR3 via IR binding produces dose-dependent hypoglycemic effects. Clinical data from mecasermin (recombinant native IGF-1), the closest approved analog, documents hypoglycemia as the most common adverse event, occurring in approximately 40-50% of treated patients. Concurrent food intake is the primary mitigation strategy [7].
Fluid retention and edema: IGF-1 signaling promotes renal sodium retention and increases vascular permeability, producing dose-dependent fluid accumulation. Reported manifestations include peripheral edema, arthralgia, carpal tunnel-like symptoms, and facial puffiness [8].
Oncogenic potential: Elevated circulating IGF-1 is positively associated with cancer incidence in multiple epidemiological studies. The Endogenous Hormones and Breast Cancer Collaborative Group and subsequent meta-analyses have consistently demonstrated correlations between higher IGF-1 levels and increased risk of breast, prostate, and colorectal cancers [15]. The anti-apoptotic effects of IGF-1R signaling (via AKT-mediated inhibition of BAD and caspase-9) provide a mechanistic basis for this association.
Cardiovascular effects: Tachycardia, blood pressure changes, and headache are reported in the safety profile of IGF-1 analogs. Retinopathy and intracranial hypertension-like syndromes are rare but documented concerns with sustained IGF-1 elevation [8].
Monitoring limitations: Routine clinical IGF-1 assays (immunoassay or LC-MS/MS) measure total endogenous IGF-1 and do not distinguish exogenous LR3. IGFBP displacement by LR3 can artifactually alter measured values. No validated isoform-specific assay exists for clinical monitoring of LR3 pharmacodynamics [8].
Side effect profiles are most useful when you can compare them against your own experience in real time. Doserly lets you log symptoms, severity, and timing alongside your dosing data, creating a side-by-side view of your protocol and your body's response.
This kind of systematic tracking catches things that memory alone misses. A subtle mood shift that began three days after a dose increase. Sleep disruption that correlates with evening administration. These patterns become visible when the data is laid out on a timeline, and they give your healthcare provider actionable information rather than vague concerns. Early detection of emerging side effects means earlier intervention.
Keep side effects, flags, and follow-up notes visible.
Doserly helps you document safety observations, side effects, medication changes, and follow-up questions so important context is not scattered.
Safety log
Flags and notes

Safety notes are not emergency guidance; seek medical help when appropriate.
Dosing Protocols
The Basics
There are no clinically validated human dosing protocols for IGF-1 LR3. What follows is a summary of commonly circulating patterns found in community discussions and reference sources. These are presented for educational purposes to summarize the existing landscape of available data, not as recommendations.
The most commonly reported approach involves subcutaneous injection once daily, typically in the morning or shortly before a workout, with food intake to manage blood sugar effects [3]. Most conservative protocols suggest starting at 20 mcg per day for the first 1-2 weeks to assess tolerance, gradually increasing to 40 mcg and eventually 50 mcg if well tolerated [3].
Cycle length varies considerably across sources. Some suggest short cycles of 10 days on with 4 weeks off, while others describe 4-8 week cycles with equal or longer off-periods. The rationale for cycling includes preventing receptor desensitization (diminished response with continuous use), managing cumulative safety risks, and allowing the body to return to baseline signaling [3].
Sources generally agree that doses above 50-60 mcg per day lack meaningful research support and substantially increase the risk of adverse effects. Some community sources report doses of 100 mcg or higher, but these are considered aggressive protocols without safety data backing them.
The Science
No pharmacokinetic/pharmacodynamic dose-finding studies have been conducted with IGF-1 LR3 in humans. Dosing extrapolation from mecasermin (recombinant native IGF-1, FDA-approved for severe primary IGF-1 deficiency) is not straightforward due to the fundamentally different pharmacokinetics of LR3 [7].
The commonly reported titration protocol (20 mcg weeks 1-2, 40 mcg weeks 3-4, 50 mcg weeks 5-8) represents a gradual approach that allows assessment of individual tolerance, particularly regarding hypoglycemic response [3]. This protocol is not evidence-based in the clinical sense but represents community consensus on risk mitigation.
Receptor desensitization with continuous IGF-1R agonism is a theoretical concern supported by general receptor pharmacology principles. Cycling protocols (typically 4-8 weeks on, 4-8 weeks off) are intended to maintain receptor sensitivity, though no studies have directly measured IGF-1R desensitization kinetics with LR3 specifically [3].
The dosing protocols above involve numbers that matter: specific microgram amounts, reconstitution ratios, and timing windows. Getting any of these wrong compounds across every subsequent dose from that vial.
Doserly's dose and reconstitution calculators eliminate the guesswork. Enter your vial size, peptide amount, and target dose, and get the exact bacteriostatic water volume, units per tick mark, and doses per vial. The injection site tracker maps your administration history as a visual heat map across your body, flagging areas that need rest and suggesting rotation patterns. Combined with dose reminders that include compound name, amount, and route, every aspect of your daily protocol is handled with the precision it requires.
Build reminders around the routine, not just the compound.
Doserly can keep timing, skipped doses, and schedule changes organized so the plan you read about becomes easier to follow and review.
Today view
Upcoming reminders

Reminder tracking supports consistency; it does not select a protocol for you.
What to Expect
Most community experience reports follow a general pattern, though individual responses vary considerably:
Weeks 1-2: Many users report little to no noticeable effect during the initial titration phase (typically 20 mcg/day). Some report enhanced gym pumps and muscle fullness starting within the first few days. Blood sugar effects may become apparent, particularly if dosing without food [3].
Weeks 3-4: This is where most users report noticing the compound's effects. Commonly described changes include improved endurance during workouts, increased strength, and enhanced recovery between sessions. The muscle fullness effect typically becomes more pronounced. Some users report noticeable fat loss beginning in this window, though this is difficult to separate from diet and training effects.
Weeks 5-8: Users who continue through a full cycle typically describe continued improvements in body composition, with visible muscle definition and body recomposition effects. The endurance and recovery benefits tend to be most apparent during this phase. Some users describe a "plateau" effect where additional benefits diminish, which is part of the rationale for cycling.
Post-cycle: Users commonly report that the endurance benefits diminish quickly after stopping, often within the first week. Body composition changes tend to be more durable if training and nutrition are maintained. There are no reports of significant withdrawal effects or hormonal disruption, as IGF-1 LR3 does not directly suppress the hypothalamic-pituitary axis.
Interaction Compatibility
Good With (Synergistic or Complementary)
- CJC-1295 + Ipamorelin: Stimulate natural GH release, which in turn raises endogenous IGF-1. Combining with exogenous IGF-1 LR3 addresses both the upstream signal (GH) and the downstream effector (IGF-1). This is a commonly discussed stack in community sources.
- BPC-157: Complementary healing mechanisms. BPC-157 promotes angiogenesis through VEGF pathways, while IGF-1 LR3 drives cell proliferation and tissue repair. Multiple community members have combined these for injury recovery.
- TB-500: Another tissue repair peptide that promotes cell migration and reduces inflammation. Frequently stacked with IGF-1 LR3 for recovery-focused protocols.
- GHK-Cu: Copper peptide that supports tissue remodeling and collagen synthesis. Complementary mechanism to IGF-1 LR3's cell proliferation effects.
- Tesamorelin: GHRH analog that elevates GH and IGF-1 through physiological pulsatile release. Sometimes combined with IGF-1 LR3 for combined upstream and downstream growth signaling.
- MOTS-C: Metabolic peptide that activates AMPK signaling. Addresses a complementary metabolic pathway for body composition goals.
Not Good With (Contraindicated or Cautionary)
- Insulin or insulin secretagogues: Combining IGF-1 LR3 with insulin dramatically increases hypoglycemia risk. Both compounds lower blood sugar through overlapping mechanisms, and their combined effect can be severe and unpredictable.
- Other IGF-1 analogs (e.g., PEG-MGF): Stacking multiple growth factor analogs amplifies both benefits and risks without established safety data for the combination.
- Use in individuals with active or prior malignancy: IGF-1R activation promotes cell survival and proliferation in potentially malignant cells. Any history of cancer represents a strong contraindication.
Administration Guide
Materials Required
- IGF-1 LR3 lyophilized vial (typically 1 mg)
- Bacteriostatic water (BAC water) for reconstitution
- U-100 insulin syringes (29-31 gauge, 0.5 mL or 1 mL)
- Alcohol swabs for vial stopper and injection site preparation
- Sharps disposal container
Recommended Reconstitution Solution
Bacteriostatic water is the standard reconstitution solvent. Some sources recommend 0.6% acetic acid water for improved stability, noting that IGF-1 LR3 in acetic acid solution remains essentially unchanged in potency after extended storage at 4°C. Bacteriostatic water is more commonly used and easier to work with but may result in slightly faster peptide degradation over time [3].
A typical reconstitution uses 3.0 mL bacteriostatic water per 1 mg vial, yielding a concentration of approximately 0.333 mg/mL (333 mcg/mL). At this concentration, 1 unit on a U-100 insulin syringe delivers approximately 3.33 mcg.
Timing Considerations
- Most commonly administered in the morning or 30-60 minutes before a workout
- Administration with or shortly after food intake is strongly emphasized across all sources to mitigate hypoglycemia risk [3]
- Some users prefer post-workout administration for potential localized uptake effects, though IGF-1 LR3 acts systemically regardless of injection site [1]
- Avoid administration during fasting periods or late at night without food
Post-Administration Care
- Monitor for signs of hypoglycemia (shakiness, dizziness, sweating, confusion) for 1-2 hours after administration, particularly during initial titration
- Keep fast-acting carbohydrates readily available (glucose tablets, fruit juice)
- Track injection sites and rotate systematically to prevent local irritation or lipohypertrophy
- Note any immediate reactions (injection site redness, swelling) for discussion with a healthcare provider
Supplies & Planning
Typical Materials
Supply
IGF-1 LR3 vials
- Details
- Typically supplied as 1 mg lyophilized powder
Supply
Bacteriostatic water
- Details
- 10 mL multi-use vials; 3.0 mL per vial reconstitution
Supply
Insulin syringes
- Details
- U-100, 29-31 gauge, 0.5 mL or 1 mL capacity
Supply
Alcohol swabs
- Details
- For vial stoppers and injection sites (2 per administration)
Supply
Sharps container
- Details
- For safe disposal of used syringes
Supply
Glucose tablets or juice
- Details
- Fast-acting carbohydrate source for hypoglycemia management
Specific quantities depend on dose, cycle length, and injection frequency, which should be determined in consultation with a healthcare provider. The reconstitution calculator can help determine exact bacteriostatic water volumes and doses per vial based on your specific parameters.
Storage & Handling
Lyophilized (unreconstituted) powder:
- Optimal: -20°C (-4°F) or colder (-80°C for long-term) in dry, dark conditions
- Duration: Up to 12 months at -20°C
- Short-term: 2-8°C (35.6-46.4°F) is acceptable for several months
- Protect from light, moisture, and repeated temperature fluctuations
Reconstituted solution:
- Refrigerate immediately at 2-8°C (35.6-46.4°F)
- Use within 30 days for optimal potency
- For storage beyond 30 days: prepare sterile aliquots and freeze at -20°C (stable for 3-6 months)
- Never refreeze a thawed vial
- Always inspect solution for clarity before use; discard if cloudy or containing visible particles
Handling best practices:
- Allow frozen vials to reach room temperature before opening to minimize condensation
- Use aseptic technique when drawing from reconstituted vials
- Avoid shaking; gently swirl or roll to dissolve lyophilized powder
- Label all reconstituted vials with date and concentration
Lifestyle Factors
Nutrition: Adequate protein intake (commonly cited at 1.6-2.2 g/kg body weight) supports the anabolic processes enhanced by IGF-1 LR3 signaling. Regular meal timing is particularly important with this compound to manage blood glucose stability. High-carbohydrate meals may help mitigate hypoglycemia risk, particularly around the time of administration [3].
Resistance training: IGF-1 signaling pathways are activated by mechanical loading, meaning the compound's effects on muscle growth and recovery are enhanced when combined with structured resistance training. Multiple community sources emphasize that IGF-1 LR3 is not a "magic pill" and requires consistent training to produce meaningful results.
Sleep: Prioritizing 7-9 hours of quality sleep supports endogenous growth hormone production and tissue repair processes. Since IGF-1 is the primary mediator of GH's anabolic effects, optimizing both exogenous (LR3) and endogenous (sleep-driven) IGF-1 signaling may yield complementary benefits.
Blood glucose monitoring: Given the hypoglycemia risk, periodic blood glucose monitoring during dose titration is prudent. This is particularly important for individuals with any degree of insulin sensitivity issues or those taking other compounds that affect blood sugar.
Hydration: Consistent hydration supports metabolic function and may help manage the fluid retention that is commonly associated with IGF-1 signaling.
Regulatory Status & Research Classification
United States (FDA): IGF-1 LR3 has never received FDA approval for any human therapeutic indication. It is classified as a research compound. The FDA has approved recombinant native IGF-1 (mecasermin, brand name Increlex) for treatment of severe primary IGF-1 deficiency, but this approval does not extend to IGF-1 LR3 or any modified analogs. No IND applications or clinical trials for IGF-1 LR3 are registered on ClinicalTrials.gov as of 2026.
Canada (Health Canada): No Drug Identification Number (DIN) or Natural Product Number (NPN) assigned. Not approved for human use.
United Kingdom (MHRA): Not approved for human therapeutic use. Classified as a research compound.
Australia (TGA): Not listed on the Australian Register of Therapeutic Goods. Research use only.
European Union (EMA): No marketing authorization. Research compound status.
WADA Status: IGF-1 LR3 is prohibited at all times under the World Anti-Doping Agency's Prohibited List, classified under S2 (Peptide Hormones, Growth Factors, Related Substances, and Mimetics). This applies to all athletes subject to anti-doping regulations [1].
Active clinical trials: No clinical trials for IGF-1 LR3 specifically are registered in any major trial registry. Trials of native IGF-1 (mecasermin) exist for conditions including severe primary IGF-1 deficiency, but these are distinct compounds with different pharmacokinetics.
Regulatory status changes frequently. Always verify the current legal status of any compound in your specific country or jurisdiction before making any decisions.
FAQ
What is the difference between IGF-1 LR3 and regular IGF-1?
IGF-1 LR3 is a modified version of human IGF-1 with two key structural changes: a 13-amino-acid extension at the front of the molecule and a single amino acid swap at position 3. These changes reduce how strongly the molecule binds to carrier proteins in the blood, resulting in a compound that stays active approximately 120 times longer and delivers roughly 3x the biological potency of natural IGF-1.
Can IGF-1 LR3 levels be monitored through bloodwork?
Standard laboratory tests for IGF-1 do not reliably distinguish exogenous LR3 from endogenous IGF-1. No commercially available isoform-specific assay exists for clinical monitoring of IGF-1 LR3. This is a significant practical limitation, as dose-response relationships and safety parameters cannot be tracked through routine blood panels. Multiple expert sources cite this inability to monitor as a primary reason for recommending caution or avoidance.
Does IGF-1 LR3 cause muscle hypertrophy or hyperplasia?
Based on available research data, IGF-1 LR3 appears to promote both. Hypertrophy (enlargement of existing muscle cells) occurs through enhanced protein synthesis via the mTOR pathway. Hyperplasia (creation of new muscle cells) occurs through satellite cell activation and the MAPK signaling cascade. This dual mechanism distinguishes IGF-1 analogs from many other anabolic compounds that primarily drive hypertrophy alone.
What is the commonly reported dosing range?
Based on available sources, commonly reported ranges are 20-50 mcg per day administered subcutaneously. Most conservative protocols suggest starting at the lower end (20 mcg) and gradually titrating up based on tolerance. Sources generally agree that doses above 50-60 mcg/day lack meaningful research support and increase risk. All dosing decisions should be made in consultation with a qualified healthcare provider.
Is IGF-1 LR3 safe for long-term use?
No long-term safety data exists for IGF-1 LR3 in humans. Chronically elevated IGF-1 signaling is associated with increased risk of certain cancers and potentially accelerated aging at the cellular level, which is paradoxical given its tissue repair benefits. Most sources recommend time-limited cycles (4-8 weeks) with equal or longer off-periods rather than continuous use. Consulting a healthcare professional before beginning any protocol is strongly recommended.
Does IGF-1 LR3 suppress natural hormone production?
IGF-1 LR3 does not directly suppress the hypothalamic-pituitary-gonadal axis, so it does not lower testosterone production the way anabolic steroids do. However, sustained supraphysiological IGF-1R activation could theoretically affect the GH-IGF-1 feedback loop. No formal post-cycle therapy (PCT) is typically described for IGF-1 LR3, but cycling protocols serve a similar protective function.
Sources & References
Primary Research
- Biomolecules (MDPI). "Insulin-Like Growth Factor-1 (IGF-1) and Its Monitoring in Medical Diagnostic and in Sports." Review of IGF-1 biology, analogs, and detection methods. https://www.mdpi.com/journal/biomolecules
- Jones JI, Clemmons DR. "Insulin-like growth factors and their binding proteins: biological actions." Endocrine Reviews. 1995;16(1):3-34. Comprehensive review of the IGFBP system.
- Cell Sciences. "Recombinant Human LR3 IGF-1: Product Technical Datasheet." Storage, stability, and reconstitution specifications for IGF-1 LR3.
- Francis GL, Ross M, Ballard FJ, et al. "Novel recombinant fusion protein analogues of insulin-like growth factor (IGF)-I indicate the relative importance of IGF-binding protein and receptor binding for enhanced biological potency." Journal of Molecular Endocrinology. 1992;8(3):213-223.
- Boucher J, Tseng YH, Kahn CR. "Insulin and insulin-like growth factor-1 receptors act as ligand-specific amplitude modulators of a common pathway regulating gene transcription." Journal of Biological Chemistry. 2010;285(22):17235-17245.
Animal Studies
- Philippou A, Halapas A, Maridaki M, Koutsilieris M. "Type I insulin-like growth factor receptor signaling in skeletal muscle regeneration and hypertrophy." Journal of Musculoskeletal and Neuronal Interactions. 2007;7(3):208-218.
- Clemmons DR. "Involvement of insulin-like growth factor-I in the control of glucose homeostasis." Current Opinion in Pharmacology. 2006;6(6):620-625.
- Dopinglinkki (FINCIS Anti-Doping Authority). "Insulin-like growth factor 1 (IGF-1) and long chain IGF (LR3IGF-1): Medical information and safety overview."
Additional References
- Philippou A, Papageorgiou E, Bogdanis G, et al. "Expression of IGF-1 isoforms after exercise-induced muscle damage in humans." In Vivo. 2009;23(6):871-877.
- Sonntag WE, Csiszar A, deCabo R, Ferrucci L, Ungvari Z. "Diverse roles of growth hormone and insulin-like growth factor-1 in mammalian aging: progress and controversies." Journals of Gerontology Series A. 2012;67(6):587-598.
- Frontiers in Bioengineering and Biotechnology. "Insulin-Like Growth Factor-1: A Promising Therapeutic Target for Peripheral Nerve Injury." https://www.frontiersin.org/journals/bioengineering-and-biotechnology
- Jonker SS, Giraud GD, Chang EI, Elman MR, Louey S. "Coronary vascular growth matches IGF-1-stimulated cardiac growth in fetal sheep." 2020.
- White A, Stremming J, Wesolowski SR, et al. "IGF-1 LR3 does not promote growth in late-gestation growth-restricted fetal sheep." 2025.
- Hanaoka BY, Peterson CA, Horbinski C, Crofford LJ. "Implications of glucocorticoid therapy in idiopathic inflammatory myopathies." Nature Reviews Rheumatology. 2012;8(8):448-457.
- Endogenous Hormones and Breast Cancer Collaborative Group. "Insulin-like growth factor 1 (IGF1), IGF binding protein 3 (IGFBP3), and breast cancer risk: pooled individual data analysis of 17 prospective studies." Lancet Oncology. 2010;11(6):530-542.
Doping Detection
- Drug Testing and Analysis (PubMed). "Detection of LongR3-IGF-I, Des(1-3)-IGF-I, and R3-IGF-I using immunopurification and high resolution mass spectrometry for antidoping purposes."
Related Peptide Guides
- PEG-MGF - Mechano growth factor variant, related growth factor peptide
- CJC-1295 - GHRH analog that stimulates upstream GH/IGF-1 axis
- Ipamorelin - Selective GH secretagogue, commonly stacked with GHRH analogs
- BPC-157 - Tissue repair peptide, complementary healing mechanism
- TB-500 - Cell migration and tissue repair peptide
- GHK-Cu - Copper peptide for tissue remodeling
- Tesamorelin - FDA-approved GHRH analog
- MOTS-C - Metabolic peptide, complementary pathway for body composition
- AOD-9604 - GH fragment for fat mobilization
- Sermorelin - GHRH analog for GH stimulation
- MK-677 - Oral GH secretagogue
- GHRP-2 - Growth hormone releasing peptide
- GHRP-6 - Growth hormone releasing peptide
- Hexarelin - Potent GH secretagogue with cardiac effects
- Follistatin-344 - Myostatin inhibitor, complementary anabolic mechanism
- SLU-PP-332 - Exercise mimetic compound
- 5-Amino-1MQ - NNMT inhibitor for metabolic support
- Tesofensine - Mentioned in community stacking context
Need the reconstitution math for IGF-1 LR3: Complete Research Guide?
Open the calculator with IGF-1 LR3: Complete Research Guide prefilled to estimate concentration, draw volume, and related measurement math from the reconstitution details you already have.