CJC-1295: Complete Research Guide
On this page
Quick Reference Card
Attribute
Also Known As
- Detail
- CJC-1295 with DAC, CJC-1295 without DAC, Modified GRF (1-29), Mod GRF 1-29, Tetrasubstituted GRF (1-29), Drug Affinity Complex GHRH
Attribute
Administration
- Detail
- Subcutaneous injection
Attribute
Research Status
- Detail
- Research Compound — No FDA Approval. Investigational GHRH analog. Prohibited by WADA (growth hormone secretagogue).
Attribute
Typical Dose Range
- Detail
- With DAC: 1-2 mg once or twice weekly. Without DAC (Mod GRF 1-29): 100-300 mcg 1-3 times daily.
Attribute
Half-Life
- Detail
- With DAC: ~6-8 days (albumin conjugation). Without DAC: ~30 minutes. Native GHRH: <7 minutes.
Attribute
Cycle Length
- Detail
- 8-12 weeks typical; some protocols extend to 16 weeks. Clinical data available up to 3 months.
Attribute
Storage
- Detail
- Lyophilized: -20°C long-term, 2-8°C short-term. Reconstituted: 2-8°C, use within 28 days. Protect from light.
Overview / What Is CJC-1295?
The Basics
CJC-1295 is a synthetic peptide that mimics growth hormone-releasing hormone (GHRH), the natural signal your brain sends to your pituitary gland telling it to produce growth hormone. Rather than replacing growth hormone directly, CJC-1295 amplifies your body's own production, working within your existing hormonal feedback systems rather than overriding them.
What makes CJC-1295 unusual is that it actually refers to two distinct compounds with very different behaviors. The version "with DAC" (Drug Affinity Complex) attaches itself to a protein in your blood called albumin, which keeps it active for roughly a week from a single injection. The version "without DAC," commonly called Mod GRF 1-29, clears your system in about 30 minutes, producing a sharp pulse of growth hormone that more closely mimics how your body naturally releases it.
This distinction matters practically. The DAC version offers convenience (once or twice weekly injections) but creates a sustained, continuous elevation of growth hormone. The no-DAC version requires daily injections but produces the pulsatile release pattern that many researchers consider more physiologically natural. Both versions share the same core mechanism: they bind to GHRH receptors on the pituitary and stimulate growth hormone release, which in turn raises IGF-1 levels in the liver.
People are drawn to CJC-1295 primarily for recovery support, sleep improvement, body composition changes, and age-related growth hormone decline. It is one of the most commonly used growth hormone secretagogues and is frequently combined with ipamorelin, a GHRP that works through a complementary pathway. The combination is designed to produce a larger growth hormone response than either compound alone.
It is important to note that CJC-1295 is a research compound with no FDA approval for therapeutic use. The clinical evidence base consists of a small number of Phase I/II trials in healthy adults, with no large-scale efficacy trials completed. Community experience reports are abundant but highly variable, with many users reporting subtle effects rather than dramatic transformations [1][2][3].
The Science
CJC-1295 is a synthetic tetrasubstituted 29-amino-acid analog of endogenous GHRH (1-29), engineered with four amino acid substitutions at positions 2 (D-Ala), 8 (Gln), 15 (Ala), and 27 (Leu) to confer resistance to dipeptidyl peptidase-4 (DPP-4) cleavage and other proteolytic degradation [1]. These modifications extend the plasma half-life from less than 7 minutes (native GHRH) to approximately 30 minutes for the unmodified analog (Mod GRF 1-29) and 5.8-8.1 days for the DAC-conjugated version [1][2].
The DAC (Drug Affinity Complex) modification employs a maleimidoproprionic acid derivative that forms stable thioether bonds with cysteine-34 on human serum albumin through a Michael addition reaction. Greater than 90% of administered CJC-1295 DAC becomes albumin-bound within 24 hours, creating a high-molecular-weight complex (~69 kDa) that prevents glomerular filtration and shields the peptide from enzymatic degradation [4].
CJC-1295 was originally developed by ConjuChem Biotechnologies (now Afecta Pharmaceuticals). Phase I/II clinical trials demonstrated dose-dependent increases in GH (2-10 fold) and IGF-1 (1.5-3 fold) in healthy adults, with sustained elevation lasting 6-14 days depending on dose [1]. A Phase I study (Teichman et al., 2006) in 22 healthy subjects established the pharmacokinetic profile and demonstrated that multiple doses produced cumulative IGF-1 elevation sustained for 28 days after the final dose [1].
Molecular Identity
Attribute
Common Names (No DAC)
- Detail
- CJC-1295 without DAC, Modified GRF (1-29), Mod GRF 1-29, Tetrasubstituted GRF (1-29)
Attribute
Common Names (With DAC)
- Detail
- CJC-1295 with DAC, CJC-1295 DAC, Drug Affinity Complex GHRH
Attribute
Amino Acid Sequence (Mod GRF 1-29)
- Detail
- Tyr-D-Ala-Asp-Ala-Ile-Phe-Thr-Gln-Ser-Tyr-Arg-Lys-Val-Leu-Ala-Gln-Leu-Ser-Ala-Arg-Lys-Leu-Leu-Gln-Asp-Ile-Leu-Ser-Arg-NH2
Attribute
Sequence Length
- Detail
- 29 amino acids
Attribute
Molecular Formula (No DAC)
- Detail
- C152H252N44O42
Attribute
Molecular Weight (No DAC)
- Detail
- 3,367.9 Da
Attribute
Molecular Formula (With DAC)
- Detail
- C165H269N47O46
Attribute
Molecular Weight (With DAC)
- Detail
- 3,647.28 Da
Attribute
CAS Number
- Detail
- 863288-34-0
Attribute
Structural Type
- Detail
- Linear peptide
Attribute
Source
- Detail
- Synthetic; derived from the first 29 amino acids of endogenous GHRH with four amino acid substitutions
Attribute
Target Receptor
- Detail
- GHRH-R (Growth Hormone-Releasing Hormone Receptor)
Attribute
Solubility
- Detail
- Water-soluble
Attribute
Key Modifications
- Detail
- Position 2: L-Ala to D-Ala (DPP-4 resistance); Position 8: Asn to Gln (stability); Position 15: Gly to Ala (enzymatic cleavage resistance); Position 27: Met to Leu (oxidation prevention)
Mechanism of Action
The Basics
Your body naturally releases growth hormone in pulses throughout the day, with the largest surges happening during deep sleep. This release is controlled by a signaling system where GHRH (growth hormone-releasing hormone) from your hypothalamus tells the pituitary gland to produce growth hormone, and another signal called somatostatin tells it to stop. CJC-1295 works by mimicking the "go" signal, GHRH, but in a form that lasts much longer than the natural version.
Think of natural GHRH as a text message that gets deleted after a few minutes. CJC-1295 without DAC is like that same text message but one that stays readable for about 30 minutes, long enough to get a strong response. CJC-1295 with DAC is like attaching that message to a large carrier that circles through your bloodstream for days, continuously delivering the signal.
The growth hormone your pituitary releases in response then travels to the liver, where it triggers production of IGF-1 (insulin-like growth factor 1). IGF-1 is the downstream mediator responsible for many of the effects people associate with growth hormone: tissue repair, fat metabolism, protein synthesis, and cellular recovery.
Critically, because CJC-1295 stimulates your body's own growth hormone production rather than introducing synthetic GH directly, the pituitary retains its regulatory function. The natural braking system (somatostatin) still works, which is a relevant safety consideration compared to exogenous growth hormone administration.
The Science
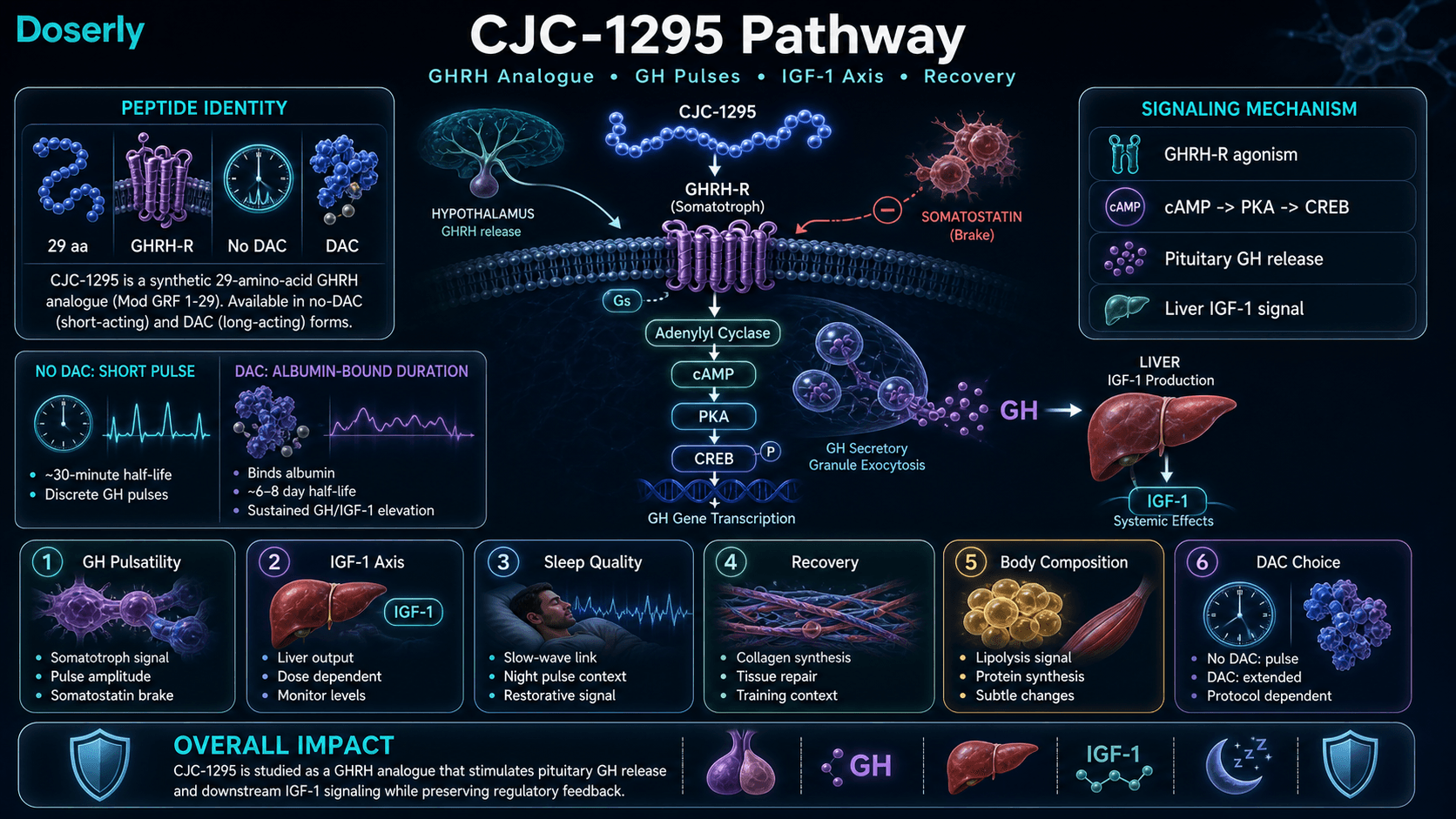
CJC-1295 exerts its biological effects through selective agonism of the growth hormone-releasing hormone receptor (GHRHR), a class B G-protein coupled receptor (GPCR) of the secretin receptor family expressed predominantly on anterior pituitary somatotrophs [1][5].
Receptor binding and signaling cascade: CJC-1295 binds to the GHRHR extracellular N-terminal domain with high affinity (Kd approximately 2-5 nM). This induces conformational changes that activate Gs-coupled adenylyl cyclase, increasing intracellular cyclic AMP (cAMP). The cAMP-PKA cascade phosphorylates CREB (cAMP response element-binding protein), upregulating growth hormone gene transcription and promoting GH secretion through exocytosis of secretory granules [1][5].
Preservation of pulsatility: A notable finding from clinical studies is that CJC-1295 preserves the pulsatile pattern of GH secretion even during continuous stimulation. Twelve-hour nocturnal monitoring in healthy men showed that CJC-1295 (60-90 mcg/kg) increased mean GH concentrations 7.5-fold while maintaining normal pulse frequency. This is significant because the pulsatile nature of GH secretion is considered physiologically important for downstream effects [3].
GH/IGF-1 axis activation: CJC-1295 administration produces dose-dependent increases in mean 24-hour GH concentrations of 2- to 2.5-fold, with corresponding IGF-1 elevations of 1.5-3 fold. IGF-1 elevation following a single dose persists for 9-11 days, and cumulative dosing over 4 weeks maintains IGF-1 above baseline for approximately 28 days after the final dose [1].
DAC-specific pharmacology: The albumin-bound DAC version creates what some researchers describe as a "GH bleed," a continuously elevated baseline GH rather than the discrete pulsatile pattern produced by the no-DAC version. When combined with a GHRP such as ipamorelin, the DAC version amplifies the amplitude of GH pulses triggered by the GHRP while maintaining elevated baseline levels between pulses [5].
Pathway Visualization Image
Pharmacokinetics
The Basics
The pharmacokinetics of CJC-1295 depend entirely on which version you are looking at, and understanding this distinction is essential for protocol design.
CJC-1295 without DAC (Mod GRF 1-29) has a half-life of approximately 30 minutes. After a subcutaneous injection, it produces a sharp growth hormone pulse within 15-30 minutes that returns to baseline within 2-3 hours. This short window is why most protocols using the no-DAC version call for daily (or multiple daily) injections, typically timed before sleep to align with the body's natural nocturnal GH peak.
CJC-1295 with DAC transforms this picture entirely. After injection, the DAC modification causes the peptide to bind to albumin in your blood within hours, creating a long-circulating complex with a half-life of approximately 6-8 days. A single dose keeps growth hormone elevated for 6 or more days, and IGF-1 remains elevated for 9-11 days. After 3-4 weeks of weekly dosing, the compound reaches steady state, meaning levels stabilize at a predictable baseline.
For the DAC version, peak plasma concentrations occur 6-12 hours after subcutaneous injection, with bioavailability ranging from 70-85%. Steady state is typically reached after 3-4 weeks of consistent weekly administration.
The Science
Mod GRF 1-29 (No DAC): The four amino acid substitutions extend plasma half-life from <7 minutes (native GHRH) to approximately 30 minutes. Peak GH release occurs within 15-30 minutes of subcutaneous administration, returning to baseline within 2-3 hours. The short half-life produces discrete GH pulses that mimic physiological secretion patterns [1][2].
CJC-1295 DAC: Following subcutaneous administration, CJC-1295 DAC demonstrates biphasic absorption kinetics. An initial rapid phase completes within 2-4 hours, followed by slower absorption as albumin conjugation occurs over 24 hours. Peak plasma concentrations occur between 6-12 hours. Volume of distribution approximates plasma volume (0.04-0.06 L/kg), consistent with albumin-bound distribution. Bioavailability is 70-85% via subcutaneous route [4][1].
Terminal elimination half-life ranges from 5.8 to 8.1 days, with coefficient of variation less than 25%, allowing predictable steady-state achievement after 3-4 weekly doses. Elimination occurs primarily through proteolytic degradation; renal clearance is minimal due to the albumin complex exceeding the glomerular filtration threshold [4].
Pharmacodynamic comparison: A single dose of CJC-1295 DAC (30-60 mcg/kg) increases GH levels 2-10 fold for 6+ days and elevates IGF-1 for 9-11 days. After 3-4 weekly doses, IGF-1 remains above baseline for 28 days following the final dose, demonstrating cumulative pharmacodynamic effects [1].
The half-life and clearance data above tells you how long the compound stays active, but what does that mean for your daily schedule? Doserly's pharmacokinetic tools let you plug in your dose and frequency to see a projected concentration timeline, helping you understand when you're at peak levels and when the compound has largely cleared.
This becomes especially useful when titrating. If you're increasing your dose gradually, the estimator shows how each step changes your projected peak and trough levels, giving you and your healthcare provider concrete data to discuss at check-ins rather than relying on subjective feel alone.
See where a dose, cycle, or change fits in time.
Doserly gives each protocol a timeline so dose changes, pauses, restarts, and observations are easier to compare later.
Timeline
Cycle history

Timeline tracking helps with recall; it is not a treatment recommendation.
Research & Clinical Evidence
The Basics
The research on CJC-1295 is based on a small number of well-designed human studies in healthy adults, supported by animal studies. The key finding is consistent: CJC-1295 reliably increases growth hormone and IGF-1 levels in a dose-dependent manner. The clinical data is limited but encouraging, showing the compound is well-tolerated with a predictable pharmacological profile.
What the research does not yet show is long-term efficacy data for specific therapeutic outcomes like body composition changes, injury recovery, or anti-aging benefits. The studies demonstrate that the compound does what it is designed to do (raise GH and IGF-1), but translating that hormonal change into measurable health outcomes requires larger and longer trials that have not been completed.
The Science
Phase I/II clinical data (Teichman et al., 2006): A randomized study in 22 healthy adults evaluated single and repeated doses of CJC-1295 DAC (30-60 mcg/kg subcutaneous). Single doses produced 2-10 fold increases in mean GH concentrations, sustained for 6+ days. IGF-1 elevated for 9-11 days post-injection. Multiple weekly doses over 4 weeks produced cumulative IGF-1 elevation sustained for 28 days after the final dose. The compound was well-tolerated with no serious adverse events [1].
Pulsatility preservation (Ionescu & Frohman, 2006): Twelve-hour nocturnal monitoring in healthy men demonstrated that CJC-1295 (60 and 90 mcg/kg) increased mean GH 7.5-fold while preserving normal pulse frequency. Baseline GH amplitude increased but pulse rhythm remained intact. IGF-1 climbed 45%. Both doses produced similar effects, suggesting a therapeutic window [3].
GH/IGF-1 axis effects (Alba et al., 2006): In GHRH-knockout mice, once-daily CJC-1295 administration for 5 weeks normalized bone growth, lean mass, and body composition. Pituitary somatotroph cell populations expanded, and GH gene expression increased, confirming CJC-1295 acts as a functional GHRH replacement [6].
Serum protein profile changes (2009): Administration of CJC-1295 to 11 healthy men produced GH elevations of 2-10 fold and significant changes in 5 serum proteins, including apolipoprotein A1 and transthyretin, suggesting broad effects on protein metabolism beyond GH/IGF-1 axis activation [7].
Limitations: No large-scale Phase III trials have been completed. The existing human data involves healthy adults over short durations (weeks), not clinical populations or long-term protocols. The no-DAC version (Mod GRF 1-29) has never been the subject of an independent human clinical trial; the available data applies to the DAC formulation [1][3].
Biomarker Evidence Matrix
Category
Sleep Quality
- Evidence Strength
- 4/10
- Reported Effectiveness
- 7/10
- Summary
- Limited clinical evidence for sleep specifically, but mechanism supports it (GH release during sleep). Community reports are strongly and consistently positive for sleep improvement.
Category
Recovery & Healing
- Evidence Strength
- 4/10
- Reported Effectiveness
- 7/10
- Summary
- Animal data supports GH-mediated tissue repair. No human clinical recovery data specific to CJC-1295. Community reports consistently cite recovery as a primary benefit.
Category
Fat Loss
- Evidence Strength
- 5/10
- Reported Effectiveness
- 5/10
- Summary
- Mechanistically supported by GH/IGF-1 lipolytic effects. Clinical studies show body composition changes in GH-deficient populations. Community reports are mixed with high confounding.
Category
Muscle Growth
- Evidence Strength
- 4/10
- Reported Effectiveness
- 4/10
- Summary
- GH/IGF-1 elevation supports protein synthesis. Animal data shows normalized growth. Community reports range widely from meaningful gains to no effect.
Category
Physical Performance
- Evidence Strength
- 3/10
- Reported Effectiveness
- 5/10
- Summary
- Limited clinical evidence. Community reports suggest modest strength/endurance improvements, primarily secondary to recovery benefits.
Category
Energy Levels
- Evidence Strength
- 3/10
- Reported Effectiveness
- 5/10
- Summary
- No clinical evidence specific to energy. Some community reports of improved vitality, likely secondary to sleep and GH elevation.
Category
Skin Health
- Evidence Strength
- 3/10
- Reported Effectiveness
- 5/10
- Summary
- Collagen synthesis is a known downstream effect of GH/IGF-1. Limited community data, some positive reports of improved skin quality.
Category
Joint Health
- Evidence Strength
- 3/10
- Reported Effectiveness
- 5/10
- Summary
- GH supports connective tissue maintenance. A few community reports of joint comfort improvement.
Category
Side Effect Burden
- Evidence Strength
- 6/10
- Reported Effectiveness
- 7/10
- Summary
- Clinical trials demonstrate mild, transient side effects. Community consensus supports good tolerability profile.
Category
Fluid Retention
- Evidence Strength
- 5/10
- Reported Effectiveness
- 6/10
- Summary
- Water retention is a known pharmacological effect of GH elevation. Commonly reported in community, especially with DAC version.
Categories scored: 10
Categories with community data: 15 (10 scored, 5 below threshold)
Categories not scored (insufficient data): Weight Management, Appetite & Satiety, Food Noise, Focus & Mental Clarity, Memory & Cognition, Mood & Wellbeing, Anxiety, Stress Tolerance, Motivation & Drive, Emotional Aliveness, Emotional Regulation, Libido, Sexual Function, Inflammation, Pain Management, Gut Health, Digestive Comfort, Nausea & GI Tolerance, Hair Health, Heart Health, Blood Pressure, Heart Rate & Palpitations, Hormonal Symptoms, Temperature Regulation, Body Image, Immune Function, Bone Health, Longevity & Neuroprotection, Cravings & Impulse Control, Social Connection, Treatment Adherence, Withdrawal Symptoms, Daily Functioning
Benefits & Potential Effects
The Basics
The benefits attributed to CJC-1295 center on what happens when you raise your body's growth hormone and IGF-1 levels. Growth hormone influences a wide range of biological processes: tissue repair, fat metabolism, protein synthesis, sleep architecture, and cellular recovery. By elevating GH production, CJC-1295 potentially supports improvements across these areas.
The most commonly reported benefit by users is improved sleep quality. Many describe deeper, more restorative sleep within the first one to two weeks. This aligns with the mechanism, since growth hormone release is closely tied to deep sleep stages, and amplifying that release may enhance sleep architecture.
Recovery from exercise and injury is the second most frequently cited benefit. Users often report reduced muscle soreness, faster return to training, and improved tolerance for high training volumes. Some users report modest changes in body composition over longer time frames, including reduced abdominal fat and improved muscle tone, though these changes tend to be subtle and require consistent training and nutrition to become apparent.
It is worth noting that many users report only modest or no noticeable effects from CJC-1295, particularly younger users whose natural GH production is already robust. The compound appears to offer more noticeable benefits for individuals over 35 whose natural GH secretion has begun to decline with age.
The Science
CJC-1295's therapeutic potential derives from sustained elevation of the GH/IGF-1 axis, which mediates multiple downstream physiological effects [1][5]:
Body composition: GH elevation promotes lipolysis (fat breakdown) through activation of hormone-sensitive lipase and enhances protein synthesis via IGF-1-mediated anabolic signaling. Clinical studies in GH-deficient populations demonstrate reductions in fat mass and increases in lean tissue with sustained GH elevation. DEXA-measurable body composition improvements typically manifest after 12-16 weeks of consistent therapy [1][4].
Tissue repair and recovery: GH and IGF-1 stimulate collagen synthesis, fibroblast proliferation, and extracellular matrix deposition. These processes support repair of connective tissue, muscle, and bone. The GH knockout mouse model demonstrated that CJC-1295 normalized bone growth and lean mass, confirming functional tissue repair capacity [6].
Sleep architecture: Endogenous GH secretion occurs predominantly during slow-wave sleep (stages 3-4). GHRH analogs may enhance this relationship bidirectionally; exogenous GHRH administration has been shown to increase slow-wave sleep duration in clinical studies of related compounds [1].
Metabolic effects: Sustained IGF-1 elevation influences glucose metabolism, lipid profiles, and protein turnover. Clinical monitoring studies demonstrate improvements in lipid panels (reduced total cholesterol and LDL) in patients with sustained GH elevation, though GH can also induce insulin resistance in susceptible individuals [4].
Side Effects & Safety Considerations
The Basics
The overall safety profile of CJC-1295 is considered favorable based on the limited clinical data available. Most side effects are mild and tend to diminish over the first few weeks of use.
The most common side effect is a flushing or warm sensation in the face and upper body shortly after injection, which typically passes within 10-15 minutes. This is more noticeable with the no-DAC version due to the more rapid onset of action. Injection site reactions, including redness and mild soreness, occur in roughly 20-30% of users but rarely require treatment.
Water retention is a commonly reported effect, particularly during the initial weeks and more pronounced with the DAC version. Some users notice puffy fingers, ankle swelling, or a slight increase in body weight from fluid. This is a known pharmacological consequence of GH elevation and typically stabilizes or can be managed by adjusting fluid and sodium intake.
Other reported effects include headaches (10-15% of users in clinical trials), tingling or numbness in extremities (carpal tunnel-like symptoms from fluid retention), and vivid dreams. A small number of community reports mention hormonal acne, which may relate to GH-driven hormonal shifts.
The most significant safety consideration applies to anyone with a history of malignancy. Because GH and IGF-1 are growth signals, any compound that elevates them is contraindicated in active cancer and should be used with caution in individuals with a history of cancer. IGF-1 monitoring is important to ensure levels remain within age-appropriate physiological ranges.
The Science
Clinical adverse event data: Phase I/II trials reported the following adverse event rates: injection site reactions (erythema, pruritus, pain) in approximately 20-30% of subjects; vasomotor flushing and headache in 10-15%; transient arthralgias and fluid retention in 5-10%. All events were mild to moderate and generally self-limiting. No significant elevations in prolactin, ACTH, or cortisol were observed, confirming CJC-1295's selectivity for the GH axis [1][4].
Contraindications: Active malignancy or history of cancer (IGF-1 is mitogenic); diabetic retinopathy (GH may worsen proliferative changes); uncontrolled diabetes mellitus (GH induces insulin resistance); severe cardiac or respiratory disease; pregnancy and breastfeeding; known hypersensitivity to GHRH analogs [4][5].
Metabolic considerations: GH elevation can induce insulin resistance in susceptible individuals. Fasting glucose and HbA1c monitoring at baseline and every 3 months is recommended for prolonged protocols. IGF-1 levels should be maintained within the upper quartile of age-adjusted normal ranges (generally 200-300 ng/mL for adults); supraphysiological elevation may increase long-term metabolic or proliferative risks [4].
Long-term safety: No long-term safety data (>3 months) exists for CJC-1295 in human subjects. Theoretical risks include acromegalic features with chronic supraphysiological GH exposure, though protocols targeting physiological IGF-1 ranges appear to minimize this risk [4].
Dosing Protocols
The Basics
CJC-1295 dosing differs fundamentally between the DAC and no-DAC versions, and understanding which version you are working with is the most important starting point.
CJC-1295 with DAC is typically administered at 1-2 mg once or twice weekly via subcutaneous injection. The long half-life means the compound accumulates in your system over weeks, reaching steady state after about 3-4 weeks. Some protocols use a gradual titration approach, starting at lower doses (300-500 mcg per injection) and increasing every 1-2 weeks based on response and tolerance.
CJC-1295 without DAC (Mod GRF 1-29) is typically administered at 100-300 mcg per injection, 1-3 times daily. Most protocols call for administration on an empty stomach (fasted for at least 2 hours) and timing doses before sleep to align with natural GH pulses. A common approach is 100 mcg once daily at bedtime for the first few weeks, gradually increasing to 200-300 mcg as tolerated. Some advanced protocols use multiple daily doses.
Both versions are commonly cycled for 8-12 weeks, with some protocols extending to 16 weeks. A washout period of 4-8 weeks between cycles is commonly cited, though no standardized cycling protocol exists in the clinical literature. IGF-1 levels typically return to baseline within 2 weeks of discontinuation.
The combination with ipamorelin (100-300 mcg) is one of the most common stacking protocols, with both compounds administered simultaneously at the same injection time.
The Science
Clinical trial dosing (DAC): Published studies evaluated single and repeated subcutaneous doses of 30-120 mcg/kg (approximately 2-8 mg for a 70 kg adult). Research protocols typically employ 2 mg (approximately 30 mcg/kg) administered once weekly for maintenance. Initial loading protocols may utilize twice-weekly administration for the first 2-4 weeks to achieve steady state more rapidly, followed by weekly maintenance. Dose escalation recommendations suggest increases of 25-50% implemented no more frequently than every 3-4 weeks [1][4].
Community dosing (No-DAC): Modified GRF 1-29 is administered at 100-300 mcg subcutaneously, 1-3 times daily. The most commonly reported protocol is once daily at bedtime on an empty stomach (fasted 2+ hours). Some protocols include a 5-on-2-off weekly cycling approach, though this is community-derived rather than clinically validated. Cycle length of 8-12 weeks is most commonly reported, with some extending to 16 weeks [1].
Combination with ipamorelin: The most common stacking protocol involves co-administration of CJC-1295 (100-300 mcg) with ipamorelin (100-300 mcg) at the same injection time. The mechanistic basis is complementary receptor activation: CJC-1295 activates GHRHR (cAMP-PKA pathway) while ipamorelin activates GHSR (PLC-IP3-PKC pathway), producing multiplicative GH release. Clinical studies demonstrate 400-800% peak GH elevation with the combination versus 100-200% with either alone [5].
The dosing protocols above involve numbers that matter: specific microgram amounts, reconstitution ratios, and timing windows. Getting any of these wrong compounds across every subsequent dose from that vial.
Doserly's dose and reconstitution calculators eliminate the guesswork. Enter your vial size, peptide amount, and target dose, and get the exact bacteriostatic water volume, units per tick mark, and doses per vial. The injection site tracker maps your administration history as a visual heat map across your body, flagging areas that need rest and suggesting rotation patterns. Combined with dose reminders that include compound name, amount, and route, every aspect of your daily protocol is handled with the precision it requires.
Turn symptom and safety notes into a clearer timeline.
Doserly helps you log doses, symptoms, and safety observations side by side so patterns are easier to discuss with a qualified clinician.
Pattern view
Logs and observations

Pattern visibility is informational and should be reviewed with a clinician.
What to Expect
CJC-1295 is not a compound that produces overnight transformations. Based on clinical data and community experience reports, here is a general timeline of what users commonly describe. Individual responses vary significantly based on age, baseline GH status, dose, version (DAC vs no-DAC), concurrent compounds, and lifestyle factors.
Weeks 1-2: The earliest reported effects are sleep-related. Many users describe deeper sleep, more vivid dreams, and feeling more refreshed upon waking. A warm flushing sensation after injection is common and typically subsides within minutes. Mild water retention may begin, particularly with the DAC version. Most users do not notice body composition changes at this stage.
Weeks 3-4: Sleep improvements often stabilize or become the new baseline. Some users notice the beginning of improved recovery, including reduced muscle soreness after training and faster bounce-back between sessions. Energy levels may improve, though this varies. IGF-1 levels are typically measurably elevated at this point (blood work confirmation is recommended by most practitioners at the 4-week mark).
Weeks 5-8: This is the window where body composition changes, if they occur, tend to become noticeable. Some users report reduced abdominal fat, improved muscle tone or definition, and enhanced exercise endurance. Skin and hair quality improvements are reported by some users during this period. Recovery benefits are often well established by this stage.
Weeks 8-12+: For those continuing beyond 8 weeks, effects generally continue to develop gradually. Strength and body composition changes may become more apparent with consistent training. IGF-1 levels should be monitored to ensure they remain within appropriate ranges. Some protocols suggest a washout period after 12 weeks, though no clinical data establishes an optimal cycling approach.
After discontinuation: IGF-1 levels typically return to baseline within approximately 2 weeks of stopping CJC-1295 DAC. Subjective effects (sleep, recovery) may persist briefly but generally diminish as GH levels normalize.
Timelines are useful benchmarks, but they mean more when you're tracking your own progress against them. Doserly lets you log daily observations alongside your protocol data, creating a personal timeline that runs parallel to the general expectations above.
When you reach the 4-week or 8-week assessment points, you'll have more than a feeling to work with. You'll have a documented record of how each week progressed, what changed, and when. This makes protocol decisions concrete: whether to extend a cycle, adjust a dose, or try a different approach, the data is there to support the conversation with your healthcare provider rather than relying on recall.
Build reminders around the routine, not just the compound.
Doserly can keep timing, skipped doses, and schedule changes organized so the plan you read about becomes easier to follow and review.
Today view
Upcoming reminders
Reminder tracking supports consistency; it does not select a protocol for you.
Interaction Compatibility
Good With (Synergistic or Complementary)
- Ipamorelin — The most common pairing. Ipamorelin activates the ghrelin receptor (GHSR), producing synergistic GH release through a complementary signaling pathway (PLC-IP3 vs cAMP-PKA). Combined peak GH 400-800% vs 100-200% for either alone.
- Tesamorelin — A more potent GHRH analog with FDA approval for HIV-associated lipodystrophy. Some practitioners switch from CJC-1295 to tesamorelin for stronger lipolytic effects.
- Sermorelin — Another GHRH analog with FDA approval history. Sometimes used as an alternative to CJC-1295 for those preferring a compound with established regulatory history.
- BPC-157 — Often included in broader recovery protocols alongside CJC-1295 for tissue repair.
- TB-500 — Used alongside CJC-1295 in recovery stacks for wound healing and anti-inflammatory support.
- MOTS-C — Mitochondrial peptide sometimes stacked for metabolic and exercise performance benefits.
- Epithalon — Longevity peptide sometimes layered into CJC-1295 protocols.
- GHRP-2 — Another GHRP option for GH pulse amplification, though with more pronounced appetite stimulation and cortisol effects than ipamorelin.
- GHRP-6 — Similar to GHRP-2 with stronger appetite stimulation effects.
- Hexarelin — Potent GHRP with broader secretagogue activity; less selective than ipamorelin.
- MK-677 — Oral GH secretagogue sometimes combined with CJC-1295 DAC for enhanced IGF-1 elevation. One community report showed IGF-1 rising from 179 to 322 ng/mL on this combination.
- DSIP — Sleep peptide sometimes combined for enhanced sleep architecture.
Not Good With (Caution or Contraindicated)
- Exogenous HGH — Combining CJC-1295 with direct growth hormone administration may produce supraphysiological GH levels, increasing risks of insulin resistance, fluid retention, and long-term proliferative concerns.
- Insulin — GH elevation from CJC-1295 can antagonize insulin action. Individuals on insulin therapy should exercise caution and monitor blood glucose closely.
- Somatostatin analogs (octreotide, lanreotide) — These suppress GH secretion and would directly counteract CJC-1295's mechanism of action.
- High-dose corticosteroids — May impair the GH response and counteract anabolic signaling.
Administration Guide
CJC-1295 is administered via subcutaneous injection. Both the DAC and no-DAC versions are supplied as lyophilized (freeze-dried) powder that requires reconstitution before use.
Materials typically required: Insulin syringes (U-100, 29-31 gauge), bacteriostatic water for reconstitution, alcohol swabs for vial stopper and injection site, a sharps container for needle disposal.
Recommended reconstitution solution: Bacteriostatic water (0.9% benzyl alcohol) is the standard reconstitution solution. For the DAC version (5 mg vial), 2.0 mL of bacteriostatic water yields a concentration of 2.5 mg/mL. For the no-DAC version (5 mg vial), 3.0 mL yields approximately 1.67 mg/mL. The solution should be clear and colorless after reconstitution; discard if cloudy or discolored.
Timing considerations: The no-DAC version should be administered on an empty stomach (fasted for at least 2 hours) to prevent insulin and somatostatin from blunting the GH response. Most protocols recommend bedtime administration to align with natural nocturnal GH pulsatility. The DAC version has less timing sensitivity due to its extended half-life, though evening administration may still offer theoretical alignment with natural GH patterns. When combining with ipamorelin, both compounds can be administered at the same time.
Post-administration care: A warm flushing sensation in the face is common immediately after injection, particularly with the no-DAC version, and typically resolves within 10-15 minutes. Mild injection site redness or tenderness may occur. Monitor for signs of fluid retention (swollen fingers, ankle puffiness) during the first 2-4 weeks. Report persistent headaches, numbness or tingling in extremities, or joint pain to a healthcare provider, as these may indicate excessive GH stimulation.
Supplies & Planning
The following materials are generally associated with CJC-1295 protocols. Specific quantities depend on dose, frequency, and cycle length, which should be determined in consultation with a healthcare provider.
Peptide vials: CJC-1295 (both DAC and no-DAC versions) is commonly available in 2 mg and 5 mg lyophilized vials. The 5 mg vial provides more doses per reconstitution, reducing preparation frequency.
Reconstitution solution: Bacteriostatic water (10 mL bottles). Approximately 2.0-3.0 mL is used per vial depending on desired concentration.
Syringes: U-100 insulin syringes with 29-31 gauge needles (5/16" to 1/2"). For very small volumes (under 10 units), 30-unit or 50-unit insulin syringes offer improved measurement accuracy.
Alcohol swabs: Two per injection session (one for vial stopper, one for injection site).
Sharps container: For safe disposal of used syringes and needles.
Storage supplies: Reconstituted vials should be stored in a refrigerator at 2-8°C and used within 28 days.
For precise calculations of bacteriostatic water volume, concentration, doses per vial, and supply quantities, use Doserly's reconstitution calculator or consult with a healthcare provider.
Storage & Handling
Lyophilized (powder) form: Store at -20°C (-4°F) for long-term storage (up to 2-3 years). Short-term storage at 2-8°C (refrigerator) is acceptable for weeks to months. Keep in sealed packaging with desiccant to minimize moisture exposure. Allow vials to reach room temperature before opening to prevent condensation from degrading the powder.
Reconstituted (liquid) form: Refrigerate immediately at 2-8°C after reconstitution. Use within 28 days when reconstituted with bacteriostatic water. Do not freeze reconstituted solutions, as freezing denatures peptides. Avoid repeated freeze-thaw cycles. Protect from light by wrapping vials in foil or storing in opaque containers.
Handling best practices: Before each use, inspect the reconstituted solution for clarity. It should be colorless and clear with no cloudiness, particles, or discoloration. Discard if any abnormalities are observed. Use aseptic technique: swab the vial stopper with alcohol before each draw, use a fresh sterile syringe for each injection, and dispose of needles immediately in a sharps container. Label each vial with the reconstitution date.
Lifestyle Factors
Several lifestyle factors can influence the effectiveness of CJC-1295 protocols:
Nutrition: A high-protein, balanced diet supports the increased protein synthesis driven by GH/IGF-1 elevation. Adequate amino acid availability is essential for translating the anabolic signal into actual tissue repair and muscle maintenance. Some practitioners recommend managing sodium intake to minimize fluid retention, particularly during the initial weeks.
Exercise: Both resistance training and aerobic exercise complement CJC-1295's effects. Resistance training provides the stimulus for muscle adaptation, while aerobic activity supports cardiovascular health and fat metabolism. GH secretagogues appear to offer the most benefit when paired with consistent training rather than used passively.
Sleep: Growth hormone is released predominantly during deep, slow-wave sleep. Prioritizing 7-9 hours of quality sleep supports the natural GH pulse that CJC-1295 amplifies. Poor sleep may reduce the compound's effectiveness by limiting the physiological window during which GH release is most active.
Fasting state for administration: The no-DAC version should be administered in a fasted state (2-3 hours after eating, with no fats or carbohydrates during the fasting window). Insulin release from eating suppresses GH secretion, and carbohydrates trigger somatostatin release, both of which can blunt the pituitary's response to the GHRH analog. Black coffee and water are acceptable during the fasting window.
Hydration and electrolytes: Increased water intake is recommended, along with attention to potassium and magnesium levels. Some community protocols suggest proactively increasing these electrolytes to offset fluid retention effects.
Monitoring: Regular blood work is recommended for anyone using CJC-1295 for more than a few weeks. Key markers include IGF-1 (to confirm response and ensure levels remain in physiological range), fasting glucose and HbA1c (GH can affect insulin sensitivity), and a comprehensive metabolic panel.
Regulatory Status & Research Classification
United States (FDA): CJC-1295 is not approved by the FDA for any therapeutic indication. It is classified as an investigational compound. CJC-1295 without DAC (Mod GRF 1-29) has never been the subject of an independent human clinical trial. CJC-1295 with DAC completed Phase I/II studies but did not advance to Phase III approval trials. The compound has been available through compounding pharmacies under Section 503A provisions, though its regulatory status in the compounding space has been subject to ongoing scrutiny.
Canada (Health Canada): Not approved. No DIN or NPN assigned.
United Kingdom (MHRA): Not approved for therapeutic use. Available as a research chemical.
Australia (TGA): Not approved. Classified as a research compound.
European Union (EMA): No marketing authorization.
WADA status: CJC-1295 (both versions) is prohibited by the World Anti-Doping Agency as a growth hormone secretagogue under the Prohibited List. Athletes subject to drug testing should not use this compound.
Regulatory status changes frequently. Always verify the current legal status of any compound in your specific country or jurisdiction before making any decisions.
FAQ
What is the difference between CJC-1295 with DAC and without DAC?
The two versions share the same core peptide sequence but differ significantly in how long they remain active. The DAC (Drug Affinity Complex) modification binds the peptide to albumin in the blood, extending the half-life from about 30 minutes to approximately 6-8 days. This means the DAC version can be injected once or twice weekly, while the no-DAC version (often called Mod GRF 1-29) requires daily administration. The no-DAC version produces sharper, more pulsatile GH release that more closely mimics natural secretion patterns, while the DAC version creates a more sustained, continuous GH elevation.
How long does it take to notice effects from CJC-1295?
Based on community reports, the earliest noticeable effects are typically sleep-related improvements within the first 1-2 weeks. Recovery benefits often become apparent by weeks 3-4. Body composition changes, when they occur, generally require 5-8+ weeks of consistent use combined with appropriate training and nutrition. Some users report noticing effects within days, while others report minimal subjective changes even after several months. Blood work (IGF-1 levels) typically shows measurable elevation within 2-4 weeks.
Should CJC-1295 be taken on an empty stomach?
For the no-DAC version, most sources recommend administration in a fasted state (at least 2 hours after eating, with no fats or carbohydrates). This is because insulin released after eating suppresses GH secretion, potentially blunting the pituitary's response. For the DAC version, fasting is less critical due to the sustained mechanism of action, though some practitioners still recommend it.
Can CJC-1295 be combined with ipamorelin?
The CJC-1295 and ipamorelin combination is one of the most commonly used peptide stacks. The two compounds work through complementary receptor pathways (GHRH receptor and ghrelin receptor, respectively), producing synergistic GH release. Research data suggests the combination can increase peak GH concentrations by 400-800% compared to baseline, exceeding the response from either compound alone. Both can be administered at the same injection time.
What blood work should be monitored while using CJC-1295?
Based on available clinical guidance, commonly recommended monitoring includes: IGF-1 levels (to confirm response and ensure levels remain within age-appropriate physiological ranges), fasting glucose and HbA1c (GH can affect insulin sensitivity), a comprehensive metabolic panel (electrolytes, liver function), and lipid panel for prolonged use. IGF-1 should be checked at baseline and at 4-6 week intervals during dose titration, then every 3 months during maintenance.
Is CJC-1295 safe to use long-term?
Long-term safety data (beyond 3 months) does not exist for CJC-1295 in human subjects. Short-term clinical trials demonstrate mild, transient side effects and no serious adverse events. The primary theoretical concern with long-term use is sustained supraphysiological GH/IGF-1 elevation, which could potentially affect insulin sensitivity and has theoretical proliferative implications. Regular blood work monitoring and maintaining IGF-1 within physiological ranges are considered important by most practitioners. The compound is contraindicated in individuals with active malignancy.
Sources & References
[1] Teichman SL, Neale A, Lawrence B, Gagnon C, Castaigne JP, Bhatt DL. Prolonged stimulation of growth hormone (GH) and insulin-like growth factor I secretion by CJC-1295, a long-acting analog of GH-releasing hormone, in healthy adults. Journal of Clinical Endocrinology & Metabolism. 2006;91(3):799-805. DOI: 10.1210/jc.2005-1904. PMID: 16352683.
[2] Ionescu M, Frohman LA. Pulsatile secretion of growth hormone (GH) persists during continuous stimulation by CJC-1295, a long-acting GH-releasing hormone analog. Journal of Clinical Endocrinology & Metabolism. 2006;91(12):4792-4797. PMID: 17018654.
[3] Ionescu M, Frohman LA. Effects of CJC-1295 on Growth Hormone Secretion. Hormone Research. 2006;65(Suppl 4):86-91. DOI: 10.1159/000091256.
[4] Biovail Corporation. CJC-1295: Pharmacokinetic and pharmacodynamic evaluation in healthy subjects. Phase I clinical study data. PMID: 15328142.
[5] Bowers CY, Momany FA, Reynolds GA, Hong A. On the in vitro and in vivo activity of a new synthetic hexapeptide that acts on the pituitary to specifically release growth hormone. Endocrinology. 1984;114(5):1537-1545. PMID: 9467542.
[6] Alba M, Fintini D, Sagazio A, Lawrence B, Castaigne JP, Stier C, Bhatt DL. Once-daily administration of CJC-1295, a long-acting growth hormone-releasing hormone (GHRH) analog, normalizes growth in the GHRH knockout (GHRHKO) mouse. American Journal of Physiology: Endocrinology and Metabolism. 2006;291(6):E1290-E1294. PMID: 16822960.
[7] Sackmann-Sala L, Ding J, Frohman LA, Bhatt DL. Activation of the GH/IGF-1 axis by CJC-1295, a long-acting GHRH analog, results in serum protein profile changes in normal adult subjects. Growth Hormone & IGF Research. 2009;19(6):471-477. PMID: 19386527.
Related Peptide Guides
- Ipamorelin — Most common CJC-1295 pairing; complementary GHRP for synergistic GH release
- Tesamorelin — FDA-approved GHRH analog; stronger lipolytic evidence base
- Sermorelin — GHRH analog with FDA approval history; alternative to CJC-1295
- GHRP-2 — Growth hormone-releasing peptide; alternative to ipamorelin with stronger appetite effects
- GHRP-6 — Growth hormone-releasing peptide; notable appetite stimulation
- Hexarelin — Potent GHRP with broader secretagogue activity
- MK-677 — Oral GH secretagogue; sometimes combined with CJC-1295
- BPC-157 — Tissue repair peptide; commonly included in broader recovery stacks
- TB-500 — Recovery and healing peptide; complementary to GH elevation protocols
- IGF-1 LR3 — Direct IGF-1 analog; downstream of the pathway CJC-1295 stimulates
- CJC No DAC / Ipamorelin 5mg Blend — Pre-mixed blend of CJC-1295 (no DAC) and ipamorelin
- CJC No DAC / Ipamorelin 10mg Blend — Higher-dose pre-mixed blend
Need the reconstitution math for CJC-1295: Complete Research Guide?
Open the calculator with CJC-1295: Complete Research Guide prefilled to estimate concentration, draw volume, and related measurement math from the reconstitution details you already have.