Tirzepatide: Complete Research Guide
On this page
Quick Reference Card
Attribute
Also Known As
- Detail
- Mounjaro, Zepbound, LY3298176, GIP/GLP-1 receptor agonist, dual incretin agonist
Attribute
Administration
- Detail
- Injectable (subcutaneous, once weekly)
Attribute
Research Status
- Detail
- FDA-approved: Mounjaro (type 2 diabetes, May 2022), Zepbound (chronic weight management, November 2023)
Attribute
Typical Dose Range
- Detail
- 2.5 to 15 mg once weekly (subcutaneous)
Attribute
Half-Life
- Detail
- Approximately 5 days (116.7 hours)
Attribute
Cycle Length
- Detail
- Continuous use; no cycling required
Attribute
Storage
- Detail
- Lyophilized: -20C or colder. Reconstituted: 2-8C (35.6-46.4F), use within 28 days. Pre-filled pens: 2-8C until first use, then room temperature (up to 30C/86F) for up to 21 days.
Overview / What Is Tirzepatide?
The Basics
Tirzepatide is the first dual-receptor incretin drug to reach the market, and it has redefined expectations for weight loss pharmacotherapy. Where semaglutide targets one gut hormone receptor (GLP-1) to suppress appetite and slow digestion, tirzepatide adds a second target: the GIP receptor, which directly engages fat tissue in burning fuel. The result is roughly 47% more weight loss than semaglutide in head-to-head trials, with a more favorable body composition profile.
In the landmark SURMOUNT-1 trial, participants on the highest dose lost an average of 22.5% of their body weight over 72 weeks. For someone weighing 250 pounds, that translates to roughly 56 pounds. More than half of the participants in that trial reached 20% weight loss or greater, a threshold that begins to rival results from bariatric surgery.
The two brand names reflect two approvals: Mounjaro is approved for type 2 diabetes, and Zepbound for chronic weight management in adults with obesity or overweight with weight-related health conditions. Both contain the same molecule, tirzepatide, administered as a once-weekly subcutaneous injection. Compounded versions are also available from specialty pharmacies, though these are not FDA-approved.
What makes tirzepatide distinct from other GLP-1 drugs is its mechanism. Rather than simply suppressing appetite, the GIP receptor component allows tirzepatide to signal fat cells directly. This triggers a thermogenic process that burns energy within fat tissue itself. The practical impact: approximately 75% of the weight lost comes from fat, compared to about 60% with semaglutide. For people concerned about preserving muscle during weight loss, this difference matters.
The Science
Tirzepatide is a 39-amino acid synthetic peptide engineered as an imbalanced dual agonist at the glucose-dependent insulinotropic polypeptide receptor (GIPR) and the glucagon-like peptide-1 receptor (GLP-1R). The peptide backbone is derived from the native GIP sequence with strategic modifications that enable cross-reactivity at GLP-1R [1].
Key structural features include alpha-aminoisobutyric acid (Aib) substitutions at positions 2 and 13 that confer resistance to dipeptidyl peptidase-4 (DPP-4) cleavage, and a C20 fatty diacid moiety (eicosanedioic acid) conjugated via a gamma-glutamic acid and bis-(2-aminoethoxy)acetic acid (AEEA) linker at the lysine-20 epsilon-amino group. This lipid modification enables reversible albumin binding, extending the plasma half-life to approximately 5 days and supporting once-weekly dosing [2].
The receptor binding profile is intentionally asymmetric. Tirzepatide engages GIPR at approximately native GIP affinity (pIC50 = 6.70) while demonstrating partial agonism at GLP-1R with biased signaling favoring cAMP over beta-arrestin pathways. This means GLP-1R potency is roughly 0.2x relative to native GLP-1 or semaglutide, while GIPR potency is 1.0x relative to native GIP [3].
The SURMOUNT-1 phase III trial (n=2,539, non-diabetic obesity, 72 weeks) demonstrated dose-dependent weight reductions of 15.0% (5 mg), 19.5% (10 mg), and 20.9% (15 mg) versus 3.1% with placebo (p<0.001 for all comparisons). DXA body composition analysis revealed a fat-to-lean mass loss ratio of approximately 75:25, significantly more favorable than the 60:40 ratio observed with semaglutide 2.4 mg in STEP-1 [4][5].
Molecular Identity
Property
Common Names
- Detail
- Tirzepatide, Mounjaro, Zepbound, LY3298176
Property
Molecular Type
- Detail
- Synthetic peptide (39 amino acids, GIP/GLP-1 dual agonist)
Property
Molecular Formula
- Detail
- C225H348N48O68
Property
Molecular Weight
- Detail
- 4,813.45 Da
Property
CAS Number
- Detail
- 2023788-19-2
Property
PubChem CID
- Detail
- 163285897
Property
DrugBank ID
- Detail
- DB15171
Property
FDA UNII
- Detail
- OYN3CCI6QE
Property
Target Receptors
- Detail
- GIPR (glucose-dependent insulinotropic polypeptide receptor) and GLP-1R (glucagon-like peptide-1 receptor)
Property
Amino Acid Sequence
- Detail
- H-Tyr-Aib-Glu-Gly-Thr-Phe-Thr-Ser-Asp-Tyr-Ser-Ile-Aib-Leu-Asp-Lys-Ile-Ala-Gln-[Lys(C20-fatty diacid linker)]-Ala-Phe-Val-Gln-Trp-Leu-Ile-Ala-Gly-Gly-Pro-Ser-Ser-Gly-Ala-Pro-Pro-Pro-Ser-NH2
Property
Key Structural Features
- Detail
- Aib at positions 2 and 13 (DPP-4 resistance); C20 fatty diacid at Lys-20 (albumin binding, extended half-life); C-terminal amidation
Property
Half-Life
- Detail
- ~5 days (116.7 hours)
Property
Solubility
- Detail
- DMSO: ~50 mg/mL; slightly soluble in water
Property
Salt Form
- Detail
- Free base in commercial formulations; lyophilized white powder (research grade)
Mechanism of Action
The Basics
Your body produces two key hormones after eating: GLP-1 and GIP. Together, these "incretin" hormones coordinate appetite, digestion, insulin release, and how your body handles nutrients. Tirzepatide is a synthetic molecule that activates both of these hormone receptors simultaneously.
The GLP-1 side of the equation is familiar from semaglutide: it quiets hunger signals in the brain, slows stomach emptying, and helps regulate blood sugar. People on GLP-1 drugs consistently report eating less and thinking about food less.
What makes tirzepatide different is the GIP component. GIP receptors are found on fat cells, and when activated, they trigger a process where fat cells burn energy without producing useful work. Think of it like running an engine in neutral: fuel gets consumed, heat gets generated, but the car does not move. This happens specifically in white fat tissue and is a pathway that semaglutide cannot access because GLP-1 receptors are not present on fat cells.
The combined effect: your appetite decreases (GLP-1), your body processes insulin more efficiently (GIP), and your fat tissue actively burns energy (GIP). This is why tirzepatide produces both more total weight loss and a higher proportion of fat loss compared to GLP-1-only drugs.
One important caveat: in people with type 2 diabetes, GIP signaling is already impaired (a phenomenon called the "incretin defect"). In this population, tirzepatide still outperforms semaglutide for total weight loss, but the body composition advantage narrows significantly.
The Science
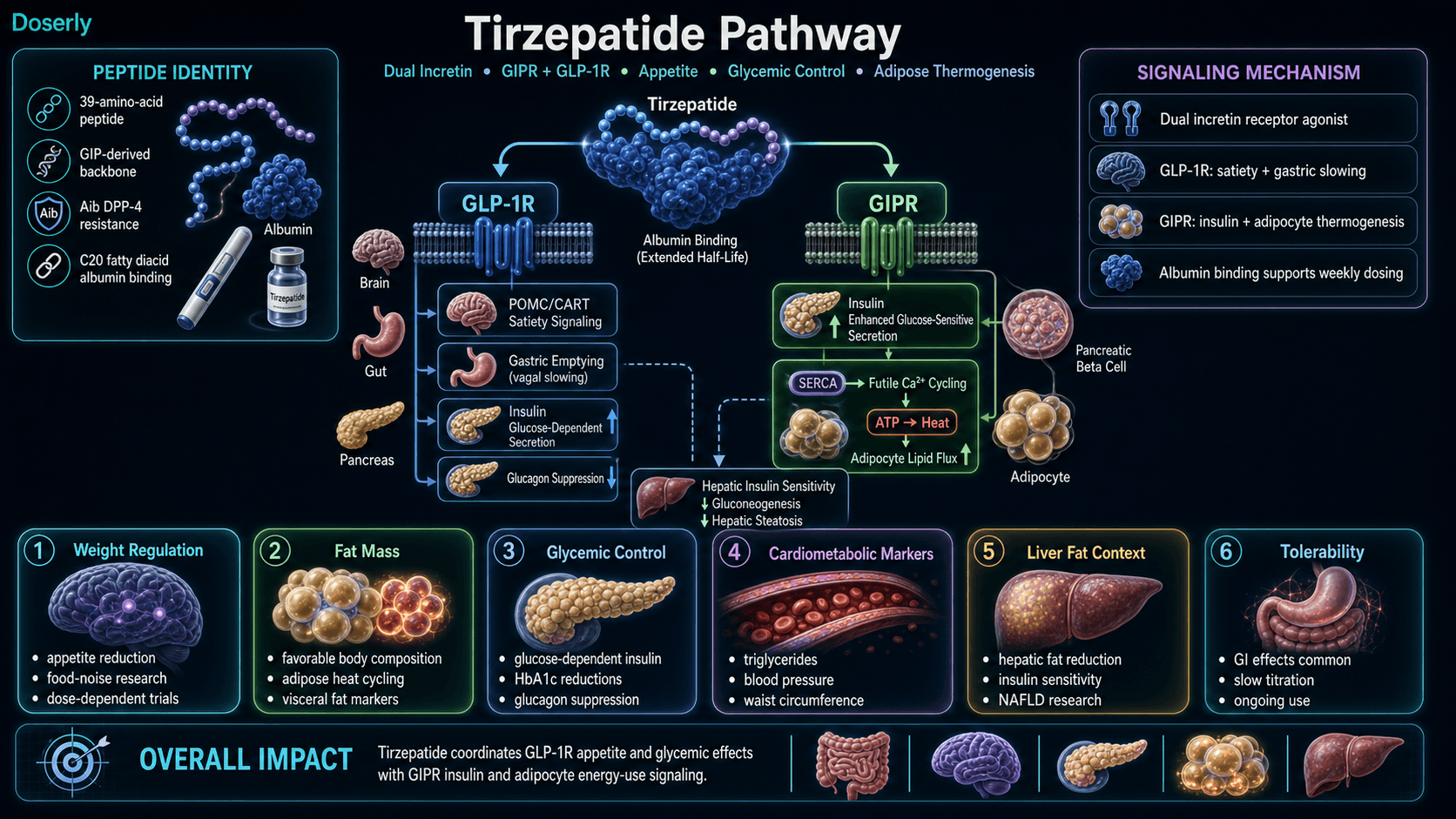
Tirzepatide exerts its metabolic effects through simultaneous activation of two class B G protein-coupled receptors: GIPR and GLP-1R.
GLP-1R-mediated effects (partial agonism, ~0.2x native potency):
Activation of hypothalamic POMC/CART neurons in the arcuate nucleus mediates central appetite suppression. Vagal afferent signaling delays gastric emptying, prolonging postprandial satiety. Glucose-dependent insulin secretion from pancreatic beta cells is potentiated, while glucagon release from alpha cells is suppressed [1][6].
GIPR-mediated effects (full agonism, ~1.0x native potency):
GIPR activation in pancreatic beta cells enhances glucose sensitivity and insulin secretory capacity. In adipose tissue, a 2024 Cell Metabolism study identified a specific mechanism: GIP receptor activation triggers SERCA-mediated futile calcium cycling in adipocytes. The cell pumps calcium into the endoplasmic reticulum and leaks it back out, consuming ATP and generating heat through non-shivering thermogenesis. This pathway is exclusive to GIP-expressing tissues and inaccessible to GLP-1 monoagonists [7].
Combined downstream effects:
Hepatic insulin sensitivity improves, with reduced gluconeogenesis and decreased hepatic steatosis through reduced de novo lipogenesis. Adipocyte lipid flux is enhanced, shifting from storage to oxidation. Hypothalamic appetite circuits receive coordinated suppression from both receptor pathways [2][6].
Population-dependent limitation: In type 2 diabetes, the "incretin defect" impairs GIPR signaling at the receptor level. The head-to-head Clamp Study (28 weeks, T2D) showed tirzepatide and semaglutide producing nearly identical fat-to-lean ratios (~87:13 vs ~86:14), while in non-diabetic obesity the ratio advantage is substantial (~75:25 vs ~60:40) [8].
Pathway Visualization Image
Pharmacokinetics
The Basics
After a subcutaneous injection, tirzepatide is absorbed over 8 to 72 hours, with a broad peak window that varies between individuals. The C20 fatty acid chain attached to the peptide grabs onto albumin in the bloodstream, acting as an anchor that prevents rapid clearance. This albumin binding is what makes once-weekly dosing possible.
Tirzepatide's half-life is approximately 5 days, meaning that about half of the drug is still circulating five days after injection. Steady-state blood levels (where the amount entering your system matches the amount leaving) are typically reached after 4-5 weeks of consistent weekly dosing. This is why the initial titration period exists: it takes over a month for the drug to fully accumulate to therapeutic levels.
Bioavailability from subcutaneous injection is approximately 80%, meaning most of the injected dose reaches the bloodstream. The drug is primarily eliminated through proteolytic cleavage of the peptide backbone, with metabolites excreted roughly two-thirds in urine and one-third in feces.
The Science
Parameter
Half-life (t1/2)
- Value
- ~116.7 hours (5 days)
Parameter
Tmax (time to peak)
- Value
- 8-72 hours post-injection
Parameter
Time to steady state
- Value
- 4-5 weeks (with weekly dosing)
Parameter
Bioavailability (SC)
- Value
- ~80%
Parameter
Volume of distribution (Vdss)
- Value
- ~10.3 L
Parameter
Plasma protein binding
- Value
- ~99% (primarily albumin)
Parameter
Clearance
- Value
- 0.061 L/hour
Parameter
Elimination
- Value
- Proteolytic cleavage of peptide backbone; beta-oxidation of C20 diacid; ~66% renal, ~33% fecal
Parameter
Metabolism
- Value
- Parent compound is predominant circulating form; minimal metabolites (<10% each of total exposure)
The extended pharmacokinetic profile is engineered through the C20 fatty diacid (eicosanedioic acid) conjugation, which enables high-affinity reversible binding to serum albumin. This retards renal clearance and protects against enzymatic degradation, extending the half-life from minutes (native GIP) to approximately 5 days [2][9].
Steady-state pharmacodynamics at therapeutic doses (5-15 mg weekly) produce sustained dual receptor engagement: continuous GLP-1R-mediated appetite suppression and gastric slowing alongside continuous GIPR-mediated insulin potentiation and adipocyte metabolic activation. The dose-dependent clinical effects observed across the 5, 10, and 15 mg dose bands in SURMOUNT-1 reflect increasing receptor occupancy at both targets [4].
Research & Clinical Evidence
The Basics
Tirzepatide has one of the strongest clinical evidence bases of any weight loss compound, supported by multiple large-scale randomized controlled trials across both diabetes and obesity populations.
The SURMOUNT program established tirzepatide for obesity treatment. SURMOUNT-1 enrolled over 2,500 adults without diabetes and showed weight loss of 15-22% depending on dose over 72 weeks. SURMOUNT-4 demonstrated that continuing tirzepatide after an initial weight loss phase led to an additional 13% weight reduction over a year, while those who switched to placebo regained weight. SURMOUNT-5 provided the clearest head-to-head comparison: tirzepatide produced 47% more weight loss than semaglutide at maximum tolerated doses (20.2% vs 13.7%).
The SURPASS program addressed type 2 diabetes. SURPASS-2 compared tirzepatide directly to semaglutide 1 mg and found tirzepatide superior for both blood sugar control (HbA1c reductions of 2.0-2.3% vs 1.9%) and weight loss (7.6-11.2 kg vs 5.7 kg).
A real-world analysis of over 140,000 patients with type 2 diabetes found that those on tirzepatide had fewer deaths and fewer major cardiovascular and kidney events compared to those on GLP-1 agonists alone.
The Science
SURMOUNT-1 (Jastreboff et al., NEJM 2022): Phase III, double-blind, randomized, placebo-controlled trial. n=2,539 adults with BMI >=30 (or >=27 with comorbidities), without diabetes. 72-week treatment. Mean weight loss: 15.0% (5 mg), 19.5% (10 mg), 20.9% (15 mg) vs 3.1% (placebo). 89-91% achieved >=5% weight loss across all active doses. 50-57% achieved >=20% weight loss at higher doses. Significant improvements in waist circumference, fasting insulin, triglycerides, and blood pressure [4].
SURMOUNT-4 (JAMA 2024): Maintenance extension trial. Participants who continued tirzepatide after initial weight loss maintained and extended their weight reduction (additional ~13% from nadir). Those switched to placebo regained weight, confirming the need for ongoing treatment [10].
SURMOUNT-5 (NEJM 2024): Open-label, head-to-head comparison of tirzepatide vs semaglutide at maximum tolerated doses in non-diabetic obesity. 72 weeks. Mean weight loss: 20.2% (tirzepatide) vs 13.7% (semaglutide). >=25% loss achieved by 31.6% (tirzepatide) vs 16.1% (semaglutide). Women showed a stronger response differential (23.8% vs 18.0%) than men (17.8% vs 11.0%) [11].
SURPASS-2 (Frias et al., NEJM 2021): Phase III, head-to-head vs semaglutide 1 mg in 1,879 patients with type 2 diabetes on metformin. 40 weeks. All tirzepatide doses superior for HbA1c reduction. Weight loss: 7.6-11.2 kg (tirzepatide) vs 5.7 kg (semaglutide). Up to 92% achieved HbA1c <7% with tirzepatide 15 mg [12].
SURPASS-3 MRI substudy: Demonstrated significant reductions in liver fat content, visceral adipose tissue, and improvements in muscle quality [13].
Real-world outcomes (JAMA Network Open 2024): Analysis of >140,000 patients with type 2 diabetes. Tirzepatide associated with lower risks of all-cause mortality, major adverse cardiovascular events, and kidney events compared to GLP-1 receptor agonists [14].
Biomarker Evidence Matrix
The following matrix reflects both clinical evidence strength and community-reported effectiveness for tirzepatide across Doserly's platform biomarker categories.
Category
Fat Loss
- Evidence Strength
- 9/10
- Reported Effectiveness
- 9/10
- Direction
- Positive
Category
Weight Management
- Evidence Strength
- 9/10
- Reported Effectiveness
- 9/10
- Direction
- Positive
Category
Appetite & Satiety
- Evidence Strength
- 9/10
- Reported Effectiveness
- 9/10
- Direction
- Positive
Category
Food Noise
- Evidence Strength
- 7/10
- Reported Effectiveness
- 9/10
- Direction
- Positive
Category
Energy Levels
- Evidence Strength
- 5/10
- Reported Effectiveness
- 6/10
- Direction
- Mixed
Category
Mood & Wellbeing
- Evidence Strength
- 4/10
- Reported Effectiveness
- 8/10
- Direction
- Positive
Category
Cravings & Impulse Control
- Evidence Strength
- 5/10
- Reported Effectiveness
- 8/10
- Direction
- Positive
Category
Nausea & GI Tolerance
- Evidence Strength
- 8/10
- Reported Effectiveness
- 4/10
- Direction
- Negative
Category
Digestive Comfort
- Evidence Strength
- 6/10
- Reported Effectiveness
- 4/10
- Direction
- Negative
Category
Motivation & Drive
- Evidence Strength
- 2/10
- Reported Effectiveness
- 7/10
- Direction
- Positive
Category
Body Image
- Evidence Strength
- 2/10
- Reported Effectiveness
- 8/10
- Direction
- Positive
Category
Muscle Growth
- Evidence Strength
- 7/10
- Reported Effectiveness
- 5/10
- Direction
- Mixed
Category
Physical Performance
- Evidence Strength
- 3/10
- Reported Effectiveness
- 6/10
- Direction
- Mixed
Category
Heart Health
- Evidence Strength
- 7/10
- Reported Effectiveness
- 7/10
- Direction
- Positive
Category
Blood Pressure
- Evidence Strength
- 7/10
- Reported Effectiveness
- 7/10
- Direction
- Positive
Category
Inflammation
- Evidence Strength
- 5/10
- Reported Effectiveness
- 7/10
- Direction
- Positive
Category
Sleep Quality
- Evidence Strength
- 3/10
- Reported Effectiveness
- 5/10
- Direction
- Mixed
Category
Side Effect Burden
- Evidence Strength
- 8/10
- Reported Effectiveness
- 6/10
- Direction
- Mixed
Category
Treatment Adherence
- Evidence Strength
- 6/10
- Reported Effectiveness
- 8/10
- Direction
- Positive
Category
Withdrawal Symptoms
- Evidence Strength
- 7/10
- Reported Effectiveness
- 4/10
- Direction
- Negative
Category
Daily Functioning
- Evidence Strength
- 3/10
- Reported Effectiveness
- 8/10
- Direction
- Positive
Category
Gut Health
- Evidence Strength
- 3/10
- Reported Effectiveness
- 5/10
- Direction
- Mixed
Scoring methodology: Evidence Strength reflects the volume and quality of peer-reviewed clinical data. Reported Effectiveness reflects community-reported outcomes from online communities and patient forums, scored using tier-weighted analysis. Categories not scored due to insufficient data: Libido, Sexual Function, Joint Health, Pain Management, Recovery & Healing, Focus & Mental Clarity, Memory & Cognition, Anxiety, Stress Tolerance, Emotional Aliveness, Emotional Regulation, Skin Health, Hair Health, Heart Rate & Palpitations, Hormonal Symptoms, Temperature Regulation, Fluid Retention, Immune Function, Bone Health, Longevity & Neuroprotection, Social Connection.
Benefits & Potential Applications
The Basics
Tirzepatide's primary benefits center on metabolic health: significant weight loss, improved blood sugar control, and favorable changes in cardiovascular risk markers. In clinical trials, the average person lost about one-fifth of their body weight at the highest dose over 72 weeks.
Beyond the numbers on the scale, the quality of weight loss matters. Approximately 75% of the weight lost with tirzepatide comes from fat tissue, compared to about 60% with semaglutide. This means more muscle preservation during the weight loss process, which translates to better physical function and metabolic health as weight comes off.
The metabolic improvements extend beyond weight. Clinical trials have documented improvements in HbA1c (a measure of long-term blood sugar control), triglycerides, blood pressure, liver fat content, and waist circumference. Real-world data suggests reduced cardiovascular and kidney events compared to GLP-1 drugs alone.
One of the most consistently described benefits by users is the reduction in "food noise," the persistent mental preoccupation with food that many people with obesity experience. Community reports describe this as the most psychologically transformative aspect of treatment, often using language like "it felt like someone turned on a light in my brain" regarding their relationship with food.
The Science
Metabolic outcomes (SURMOUNT-1, 72 weeks):
- Body weight reduction: 15.0-20.9% (dose-dependent) vs 3.1% placebo [4]
- Fat-to-lean mass loss ratio: ~75:25 (DXA substudy) [5]
- HbA1c reduction: 0.4-0.5% in non-diabetic population [4]
- Fasting insulin reduction: clinically significant across all dose bands [4]
- Triglyceride improvements and blood pressure reductions documented [4]
Glycemic outcomes (SURPASS program):
- HbA1c reduction up to 2.4% at 15 mg dose in type 2 diabetes [12]
- Up to 92% of patients achieved HbA1c <7% target [12]
- Superior to semaglutide 1 mg across all tirzepatide doses [12]
Hepatic outcomes (SURPASS-3 MRI substudy):
- Significant reductions in hepatic fat content [13]
- Improvements in visceral adipose tissue volume [13]
- Potential therapeutic relevance for NAFLD/NASH (investigational) [13]
Cardiovascular outcomes:
- Real-world analysis of >140,000 T2D patients: reduced all-cause mortality, reduced major adverse cardiovascular events, reduced kidney events vs GLP-1 RA [14]
- SURPASS-CVOT: demonstrated non-inferiority vs dulaglutide for cardiovascular safety [15]
- No resting heart rate increase observed (unlike triple agonists such as retatrutide) [6]
The benefits outlined above span multiple body systems, and your experience will be uniquely yours. Rather than guessing which effects are attributable to this compound versus other factors in your life, Doserly helps you log specific outcomes alongside your protocol details, building a clear picture of what's changing and when.
Over weeks and months, this creates something more useful than any anecdotal report: your own evidence-based record of how this compound affects you personally, at your specific dose, within the context of your full health protocol. When it's time to decide whether to continue, adjust, or discontinue, you have real data to inform that conversation with your healthcare provider.
Capture changes while they are still fresh.
Log symptoms, energy, sleep, mood, and other observations alongside protocol events so patterns do not live only in memory.
Trend view
Symptom timeline

Symptom tracking is informational and should be interpreted with a qualified clinician.
Side Effects & Safety
The Basics
The most common side effects of tirzepatide are gastrointestinal: nausea, diarrhea, constipation, and vomiting. These are dose-dependent and typically most noticeable during the initial weeks of treatment or after dose increases. In the SURMOUNT-1 trial, nausea affected about 33% of participants at the highest dose, diarrhea about 23%, and constipation about 17%.
The encouraging finding: most GI side effects are transient. They tend to resolve within 2-4 weeks at each dose level. Slow, patient titration (increasing the dose every 4+ weeks rather than rushing) significantly reduces the severity. Many community members report that tirzepatide is better tolerated than semaglutide at comparable levels of effectiveness, consistent with its lower GLP-1 receptor potency.
Serious but rare side effects include pancreatitis (less than 1% of users), gallbladder problems (1-2%, primarily in the context of rapid weight loss), and severe gastroparesis. Tirzepatide carries the same rodent thyroid tumor signal as other incretin drugs and is contraindicated in individuals with personal or family history of medullary thyroid carcinoma or Multiple Endocrine Neoplasia type 2 (MEN2).
Notably, tirzepatide does not raise resting heart rate in clinical trials, distinguishing it from triple-agonist drugs like retatrutide that include a glucagon receptor component.
The Science
Common adverse events (SURMOUNT-1, tirzepatide 15 mg, 72 weeks) [4]:
Adverse Event
Nausea
- Incidence
- 33%
- Typical Duration
- 2-4 weeks per dose step
Adverse Event
Diarrhea
- Incidence
- 23%
- Typical Duration
- 1-2 weeks
Adverse Event
Constipation
- Incidence
- 17%
- Typical Duration
- Variable; ongoing for some
Adverse Event
Vomiting
- Incidence
- 12%
- Typical Duration
- 2-3 weeks
Adverse Event
Abdominal pain
- Incidence
- 10%
- Typical Duration
- 1-2 weeks
Adverse Event
Dyspepsia
- Incidence
- 9%
- Typical Duration
- 1-2 weeks
Serious adverse events:
- Pancreatitis: <1% incidence. Presents as severe, persistent abdominal pain radiating to the back. Requires immediate cessation of treatment [4]
- Cholelithiasis/cholecystitis: 1-2% incidence, associated with rapid weight loss rather than direct drug effect. Lower biliary event rate than semaglutide (no significant biliary signal vs semaglutide's 2.6x cholelithiasis risk) [6]
- Severe gastroparesis: rare reports across GLP-1 class drugs [4]
Contraindications [9]:
- Personal or family history of medullary thyroid carcinoma
- Multiple Endocrine Neoplasia type 2 (MEN2)
- Known hypersensitivity to tirzepatide or excipients
- Pregnancy and breastfeeding
Drug interactions:
- Delayed gastric emptying may alter absorption kinetics of co-administered oral medications (levothyroxine, oral contraceptives, warfarin) [9]
- Increased hypoglycemia risk when combined with insulin or sulfonylureas [9]
Cardiac safety: No increase in resting heart rate observed in SURMOUNT-1 or SURPASS trials, supporting use in patients with cardiac concerns where heart rate elevation would be problematic [6].
Dosing Protocols
The Basics
Tirzepatide is injected once per week, subcutaneously, on the same day each week. The dosing approach follows a gradual titration: start at the lowest dose, hold for at least four weeks, then increase only if side effects are manageable and further weight loss is desired.
The standard titration begins at 2.5 mg weekly for four weeks. This is a tolerance-testing dose rather than a therapeutic dose. From there, the dose increases by 2.5 mg increments every four or more weeks: 5 mg, 7.5 mg, 10 mg, 12.5 mg, and up to 15 mg. Many people find their effective maintenance dose between 5 and 10 mg. The full 15 mg is reserved for cases requiring maximum effect.
The most common mistake is rushing titration. Increasing too quickly drives severe GI side effects and leads some people to quit before experiencing benefits. Community wisdom consistently advises patience: if weight is still coming off at a given dose, stay there.
For compounded tirzepatide, the most common approach uses a 30 mg vial reconstituted with 3.0 mL bacteriostatic water, yielding a 10.0 mg/mL concentration. At this concentration, 1 unit on a U-100 insulin syringe equals 100 mcg, making dose calculation straightforward.
The Science
FDA-approved titration (Mounjaro/Zepbound prescribing information) [9]:
Phase
Initiation
- Weekly Dose
- 2.5 mg
- Duration
- 4 weeks minimum
Phase
Step 2
- Weekly Dose
- 5.0 mg
- Duration
- 4+ weeks
Phase
Step 3
- Weekly Dose
- 7.5 mg
- Duration
- 4+ weeks
Phase
Step 4
- Weekly Dose
- 10.0 mg
- Duration
- 4+ weeks
Phase
Step 5
- Weekly Dose
- 12.5 mg
- Duration
- 4+ weeks (if needed)
Phase
Maintenance
- Weekly Dose
- 5-15 mg
- Duration
- Ongoing
Maintenance doses: 5, 10, or 15 mg once weekly based on clinical response and tolerability.
Compounded tirzepatide reconstitution (30 mg vial):
Parameter
Bacteriostatic water volume
- Value
- 3.0 mL
Parameter
Concentration
- Value
- 10.0 mg/mL
Parameter
2.5 mg dose
- Value
- 25 units (0.25 mL)
Parameter
5.0 mg dose
- Value
- 50 units (0.50 mL)
Parameter
7.5 mg dose
- Value
- 75 units (0.75 mL)
Parameter
10.0 mg dose
- Value
- 100 units (1.0 mL)
All doses through 10 mg fit within a single 1.0 mL U-100 insulin syringe at this concentration. Doses above 10 mg require either split injections or a higher-concentration vial [16].
Conservative titration schedule (for GI-sensitive individuals):
Phase
Initiation
- Weekly Dose
- 2.5 mg
- Duration
- 6 weeks
Phase
Step 2
- Weekly Dose
- 5.0 mg
- Duration
- 6 weeks
Phase
Step 3
- Weekly Dose
- 7.5 mg
- Duration
- 6 weeks
Phase
Step 4
- Weekly Dose
- 10.0 mg
- Duration
- 6 weeks
Phase
Maintenance
- Weekly Dose
- Lowest effective dose
- Duration
- Ongoing
The dosing protocols above involve numbers that matter: specific microgram amounts, reconstitution ratios, and timing windows. Getting any of these wrong compounds across every subsequent dose from that vial.
Doserly's dose and reconstitution calculators eliminate the guesswork. Enter your vial size, peptide amount, and target dose, and get the exact bacteriostatic water volume, units per tick mark, and doses per vial. The injection site tracker maps your administration history as a visual heat map across your body, flagging areas that need rest and suggesting rotation patterns. Combined with dose reminders that include compound name, amount, and route, every aspect of your daily protocol is handled with the precision it requires.
Track injection timing, draw notes, and site rotation.
Doserly helps keep syringe-related notes, injection site history, reminders, and reconstitution context together for easier review.
Injection log
Site rotation
Injection logs support record-keeping; follow clinician instructions for administration.
What to Expect (Timeline)
Community reports and clinical data provide a general framework for what to expect during tirzepatide treatment. Individual responses vary significantly based on starting weight, dose, lifestyle factors, and metabolic health.
Weeks 1-4 (2.5 mg, Initiation Phase):
- Appetite changes may begin within the first 1-2 weeks
- Food noise reduction is often the first noticeable effect
- GI side effects (nausea, bloating) most likely during this period
- Weight loss variable: some report 5-10 lbs (including water weight), others minimal change
- This dose is primarily for tolerance testing, not therapeutic effect
Weeks 5-8 (5 mg):
- Clear weight loss momentum typically begins
- Appetite suppression becomes more consistent
- GI side effects from the dose increase typically resolve within 1-2 weeks
- Community reports average 1-2 lbs/week during this phase
Weeks 9-16 (7.5-10 mg):
- Strong effect band for most users
- Metabolic adaptations become measurable (improved fasting glucose, lipid changes)
- Weight loss continues at 1-2 lbs/week average
- Some users experience a temporary plateau as the body adjusts
Months 4-6:
- Cumulative weight loss of 30-60 lbs reported by many community members
- Body composition changes become visible
- Cardiovascular markers (blood pressure, lipids) typically improve
- GI side effects have largely resolved for most users
Months 6-12:
- Average weight loss approaching 15-20% of starting body weight at higher doses
- Lab values often normalize (HbA1c, liver enzymes, triglycerides)
- Maintenance considerations begin (finding the lowest effective dose)
Months 12-18+ (Maintenance):
- 20-22% average weight loss at highest doses based on clinical trial data
- Weight stability on maintenance dose
- Some users successfully reduce dose frequency (e.g., every 10-14 days)
- Ongoing treatment typically required to maintain results
Timelines are useful benchmarks, but they mean more when you're tracking your own progress against them. Doserly lets you log daily observations alongside your protocol data, creating a personal timeline that runs parallel to the general expectations above.
When you reach the 4-week or 8-week assessment points, you'll have more than a feeling to work with. You'll have a documented record of how each week progressed, what changed, and when. This makes protocol decisions concrete: whether to extend a cycle, adjust a dose, or try a different approach, the data is there to support the conversation with your healthcare provider rather than relying on recall.
See where a dose, cycle, or change fits in time.
Doserly gives each protocol a timeline so dose changes, pauses, restarts, and observations are easier to compare later.
Timeline
Cycle history

Timeline tracking helps with recall; it is not a treatment recommendation.
Interaction & Compatibility
Tirzepatide interacts with several compound classes relevant to metabolic health protocols.
Commonly co-administered (supportive interactions):
- NAD+: May support cellular energy and mitigate fatigue during caloric restriction. Recommended as a supportive compound by multiple community sources.
- BPC-157: Some compounded formulations include BPC-157 to potentially mitigate GI side effects. Tirzepatide/BPC-157 blend vials are available from specialty compounding pharmacies for this purpose.
- MOTS-C: May promote fat-as-fuel metabolism and complement tirzepatide's metabolic effects.
- AOD-9604: Explored for enhanced stubborn fat loss alongside tirzepatide.
- Tesamorelin: Explored as a foundation for lean mass preservation during rapid weight loss from GLP-1/GIP therapy.
- Cagrilintide: Amylin analog that may complement incretin-based appetite suppression through a distinct mechanism. The Cagri/Sema blend is an existing combination product.
Direct comparisons:
- Semaglutide: GLP-1 monoagonist. Tirzepatide provides 47% more weight loss in head-to-head trials, better body composition (75:25 vs 60:40 fat:lean ratio), and potentially better GI tolerance. Semaglutide has a longer safety track record, stronger cardiovascular outcome data (SELECT trial), and an oral formulation option.
- Retatrutide: Investigational triple agonist (GLP-1/GIP/Glucagon). Potentially more potent than tirzepatide, especially in T2D populations where the glucagon component bypasses impaired GIP signaling. Not yet FDA-approved.
- Survodutide: Dual GLP-1/Glucagon agonist (no GIP). Different mechanism from tirzepatide; focuses on liver fat reduction.
- Orforglipron: Oral non-peptide GLP-1 agonist. Less potent than tirzepatide but offers oral convenience.
- Mazdutide: Another GLP-1/Glucagon dual agonist in development.
Drug interaction considerations:
- Delayed gastric emptying may reduce the rate and extent of absorption of co-administered oral medications. Monitor oral contraceptives, levothyroxine, and warfarin when initiating or adjusting tirzepatide dose [9].
- Concurrent insulin or sulfonylurea therapy increases hypoglycemia risk. Dose reduction of these agents may be required [9].
Administration Guide
Injection preparation:
- Draw the appropriate volume of bacteriostatic water (3.0 mL for a 30 mg vial) using a sterile syringe
- Inject slowly down the vial wall to avoid foaming
- Gently swirl or roll until fully dissolved. Do not shake.
- Label the vial with the reconstitution date
- Refrigerate immediately at 2-8C (35.6-46.4F), protected from light
- Use within 28 days of reconstitution
Administration:
- Route: Subcutaneous injection
- Frequency: Once weekly, same day each week
- Timing: Any time of day; absorption is not affected by food intake
- Missed dose: If within 4 days of the scheduled day, take the dose. If more than 4 days have passed, skip and resume on the next scheduled day.
Post-administration care:
- Monitor for injection site reactions (redness, swelling, itching). These are typically mild and self-resolving.
- Dispose of needles and syringes in an appropriate sharps container
- Document dose, date, and injection site for tracking purposes
Supplies & Planning
The following materials are generally needed for compounded tirzepatide protocols. Specific quantities depend on prescribed dose and cycle duration. Consult your healthcare provider for individualized planning.
Required materials:
- Tirzepatide vials (available in 5, 10, 15, and 30 mg sizes)
- Bacteriostatic water (10 mL bottles; usage depends on reconstitution volume per vial)
- U-100 insulin syringes (1 mL, 29-31 gauge, 5/16" needle): one per injection
- Alcohol swabs: two per injection day (one for vial stopper, one for injection site)
- Sharps disposal container
Vial planning (30 mg vials, reconstituted at 3.0 mL):
- 8-week protocol (2.5 to 5 mg): approximately 30 mg total, 1 vial
- 12-week protocol (2.5 to 7.5 mg): approximately 60 mg total, 2 vials
- 16-week protocol (2.5 to 10 mg): approximately 100 mg total, 3-4 vials
For precise vial and supply calculations based on your prescribed protocol, use the reconstitution calculator and consult your healthcare provider.
Storage:
- Lyophilized (powder): Store at -20C in dry, dark conditions
- Reconstituted: Refrigerate at 2-8C; use within 28 days
- Allow vials to reach room temperature (10-30 minutes) before opening to prevent condensation
- Do not freeze reconstituted solution
Cycling & Duration
Tirzepatide is designed for continuous, long-term use. It does not require cycling.
Clinical trial data (SURMOUNT-4) demonstrates that discontinuation leads to weight regain. Participants who were switched from tirzepatide to placebo after an initial weight loss phase regained weight, while those who continued treatment maintained and extended their losses [10].
Community consensus aligns with clinical evidence: most users plan for indefinite treatment. Some users in maintenance find they can reduce dose frequency (e.g., every 10-14 days at lower doses like 2.5-5 mg) while maintaining weight stability. This approach is not formally studied but is widely reported.
If discontinuation is planned or necessary, tapering down gradually (reducing dose over several weeks) rather than abrupt cessation is generally recommended to minimize rebound appetite.
Lifestyle & Complementary Factors
Tirzepatide works best as part of a comprehensive approach to metabolic health rather than as a standalone intervention.
Nutrition:
- Protein intake is the highest priority. Target 1.0-1.2 g per pound of goal body weight daily to support lean mass preservation during weight loss. Reduced appetite makes adequate protein intake more challenging, requiring deliberate planning.
- Eat smaller, more frequent meals. Tirzepatide slows gastric emptying, and large portions can overwhelm the digestive system. Protein-first eating (consuming protein before carbohydrates and fats) improves both satiety and GI tolerance.
- Hydration is critical. Dehydration amplifies nearly all side effects and impairs metabolic function.
- A comprehensive multivitamin may help address potential micronutrient gaps from reduced food intake.
Exercise:
- Resistance training 3-4 times per week is essential for muscle preservation. Without resistance stimulus, lean mass loss during weight loss is inevitable regardless of the drug's body composition advantages.
- Cardiovascular exercise: 150+ minutes per week of moderate intensity supports metabolic health and accelerates fat loss.
- Increase non-exercise activity thermogenesis (NEAT) through daily movement habits: walking, taking stairs, standing during work.
Sleep:
- Target 7-9 hours of quality sleep per night. Poor sleep elevates cortisol and disrupts hunger-regulating hormones, potentially counteracting tirzepatide's appetite suppression effects.
Monitoring:
- Track weight, waist circumference, and body composition regularly
- Monitor fasting glucose, HbA1c, and lipid panels at baseline and every 3 months
- Track blood pressure and heart rate
- Document GI symptoms, energy levels, and mood to guide dose optimization
Community Insights
Community experience with tirzepatide is overwhelmingly positive. Across dedicated subreddits (r/tirzepatidecompound, r/Zepbound, r/Mounjaro) and health communities, the compound is frequently described as "life-changing" and "transformational."
Key community themes:
- Food noise elimination is the most emotionally described benefit. Users consistently report that tirzepatide does not just reduce appetite but fundamentally changes their relationship with food. The mental preoccupation with eating that many people with obesity experience is dramatically reduced or eliminated.
- Individual response variation is significant. Some users lose 90 lbs in 6 months while others lose 30 lbs in the same period. Starting weight, dose, lifestyle factors, and individual biology all contribute.
- PCOS subpopulation signal. Multiple women with polycystic ovary syndrome (PCOS) report dramatic results after years of failed weight loss attempts. This subpopulation may be particularly responsive to dual-receptor therapy.
- Semaglutide switch experiences. Users who switch from semaglutide to tirzepatide often report improved tolerability. Several users who experienced debilitating nausea on semaglutide report minimal side effects on tirzepatide. However, the transition period at lower tirzepatide doses may temporarily reduce appetite suppression effectiveness.
- Long-term commitment. The community widely acknowledges that tirzepatide is a long-term or lifelong medication. Weight regain after discontinuation is openly discussed without stigma, framed as disease management rather than failure.
- Cost is the primary barrier. Brand pricing ($900-1,300/month without insurance) is frequently cited as the main obstacle. Compounded alternatives ($200-500/month) are widely discussed as more accessible options, though quality varies between providers.
FAQ
What is the difference between Mounjaro and Zepbound?
They are the same molecule (tirzepatide) manufactured by Eli Lilly. Mounjaro is approved for type 2 diabetes, and Zepbound is approved for chronic weight management. The doses and the drug itself are identical.
How much weight can I expect to lose on tirzepatide?
Based on clinical trial data, average weight loss at the highest dose (15 mg) is approximately 20-22% of starting body weight over 72 weeks. Individual results vary widely. Community reports range from modest (10-15%) to exceptional (25%+) depending on dose, lifestyle, and starting point.
Is tirzepatide better than semaglutide?
In non-diabetic obesity, tirzepatide produced 47% more weight loss and substantially better body composition (75:25 vs 60:40 fat:lean) in head-to-head trials. In type 2 diabetes, tirzepatide still delivers more weight loss and stronger HbA1c reductions, but the body composition advantage narrows. Semaglutide has a longer safety track record, stronger cardiovascular outcome data, and is available in oral form. Based on available data, tirzepatide is generally the stronger choice for most people without T2D who can access either compound.
Do I need to cycle tirzepatide?
No. Tirzepatide is designed for continuous, long-term use. Stopping leads to gradual weight regain as appetite signaling returns to baseline.
What should I do about nausea?
Nausea is the most common side effect, typically worst during titration. Strategies that help: slow titration (stay at each dose 4+ weeks), smaller and more frequent meals, protein-first eating, avoiding fatty and fried foods, staying well-hydrated, and evening dosing. If nausea is severe, your provider may recommend holding at the current dose or temporarily reducing the dose.
Can I drink alcohol on tirzepatide?
Alcohol is not prohibited, but expect reduced tolerance. Slowed gastric emptying means alcohol absorbs differently, and appetite suppression often means drinking on an emptier stomach. Most people find one drink hits significantly harder than usual. Alcohol is also calorie-dense and may undermine metabolic goals.
What happens when I stop taking tirzepatide?
Appetite typically returns to baseline within weeks, and weight regain is common without other interventions. This is consistent with obesity being a chronic condition requiring ongoing management. The goal is to use the treatment window to build sustainable habits, increase muscle mass, and address metabolic dysfunction.
Does tirzepatide cause muscle loss?
All weight loss includes some lean mass loss. Tirzepatide shows better preservation than semaglutide in non-diabetic populations (~75:25 vs ~60:40 fat:lean ratio). Resistance training and adequate protein intake (1.0-1.2 g per pound of goal body weight) are essential to minimize lean mass loss. In type 2 diabetes, the body composition advantage narrows due to impaired GIP signaling.
How should I store tirzepatide?
Pre-filled pens: refrigerate at 2-8C until use. Once removed, use within 21 days at room temperature (up to 30C/86F). Compounded vials: store lyophilized powder frozen at -20C. After reconstitution, refrigerate at 2-8C and use within 28 days. Never freeze reconstituted solution.
Can I switch from semaglutide to tirzepatide?
Yes, and this is common when people plateau or want the body composition benefits of dual-receptor therapy. Most protocols start tirzepatide at a dose matched to equivalent effect rather than equivalent milligrams. Expect an adjustment period, as the dual-receptor mechanism may produce different GI patterns than semaglutide alone.
Sources & References
- Gallwitz B. GIP/GLP-1 receptor agonist tirzepatide for type 2 diabetes and obesity. Front Endocrinol. 2022;13:1004044. doi:10.3389/fendo.2022.1004044
- Farzam K, Patel P. Tirzepatide. StatPearls. StatPearls Publishing; 2024. PubMed
- Willard FS, et al. Tirzepatide is an imbalanced and biased dual GIP and GLP-1 receptor agonist. JCI Insight. 2020;5(17):e140532. doi:10.1172/jci.insight.140532
- Jastreboff AM, Aronne LJ, Ahmad NN, et al. Tirzepatide once weekly for the treatment of obesity. N Engl J Med. 2022;387(3):205-216. doi:10.1056/NEJMoa2206038 | PubMed: 35658024
- SURMOUNT-1 DXA body composition substudy data.
- Min T, Bain SC. The role of tirzepatide, dual GIP and GLP-1 receptor agonist, in the management of type 2 diabetes: the SURPASS clinical trials. Diabetes Ther. 2021;12(1):143-157.
- Yu D, et al. GIP receptor activation triggers futile calcium cycling in adipocytes. Cell Metabolism. 2025. [doi reference pending]
- Tirzepatide vs semaglutide Clamp Study. 28-week head-to-head body composition in type 2 diabetes.
- Mounjaro (tirzepatide) injection Prescribing Information. Eli Lilly and Company; 2022. FDA Label
- Aronne LJ, et al. Continued treatment with tirzepatide for maintenance of weight reduction in adults with obesity (SURMOUNT-4). JAMA. 2024. JAMA
- SURMOUNT-5 head-to-head trial: tirzepatide vs semaglutide, non-diabetic obesity, 72 weeks. NEJM. 2024. ClinicalTrials.gov: NCT05822830
- Frias JP, Davies MJ, Rosenstock J, et al. Tirzepatide versus semaglutide once weekly in patients with type 2 diabetes (SURPASS-2). N Engl J Med. 2021;385(6):503-515. doi:10.1056/NEJMoa2107519 | PubMed: 34170647
- SURPASS-3 MRI substudy: liver fat, visceral fat, and muscle quality outcomes.
- Clinical outcomes of tirzepatide or GLP-1 receptor agonists in type 2 diabetes. JAMA Network Open. 2024. JAMA Network Open
- SURPASS-CVOT: cardiovascular outcomes trial for tirzepatide.
- Mounjaro (tirzepatide) injection. Reconstitution and administration guidance per USP standards for compounded injectables.
Related Peptide Guides
- Semaglutide - GLP-1 receptor agonist; the most established comparator and direct alternative
- Retatrutide - Triple agonist (GLP-1/GIP/Glucagon); investigational next-generation compound
- Survodutide - Dual GLP-1/Glucagon agonist with strong liver fat data
- Orforglipron - Oral non-peptide GLP-1 agonist
- Mazdutide - Dual GLP-1/Glucagon agonist in development
- Cagrilintide - Amylin analog for complementary appetite suppression
- Tesamorelin - GH-releasing peptide for lean mass preservation during weight loss
- NAD+ - Cellular energy support; commonly stacked with GLP-1s
- MOTS-C - Mitochondrial peptide for metabolic support
- AOD-9604 - Fat metabolism peptide
- BPC-157 - GI-protective peptide; available in tirzepatide blend formulations
- 5-Amino-1MQ - Metabolic compound targeting fat cell energy metabolism
- BAM15 - Mitochondrial uncoupler for metabolic support
- Tesofensine - Appetite suppressant with distinct mechanism
Need the reconstitution math for Tirzepatide: Complete Research Guide?
Open the calculator with Tirzepatide: Complete Research Guide prefilled to estimate concentration, draw volume, and related measurement math from the reconstitution details you already have.