TB-500 (Thymosin Beta-4 Fragment): Complete Research Guide
On this page
Quick Reference Card
Attribute
Also Known As
- Detail
- Thymosin Beta-4 Fragment 17-23, Ac-LKKTETQ, TB4 Frag, Fequesetide. Note: most commercial "TB-500" products actually contain full-length Thymosin Beta-4 (43 amino acids), not the 7-amino-acid fragment.
Attribute
Administration
- Detail
- Subcutaneous injection (primary); intramuscular injection (alternative, preferred for deep musculoskeletal injuries)
Attribute
Research Status
- Detail
- Research compound. No FDA approval for human therapeutic use. Full-length Thymosin Beta-4 has Phase 1 human safety data and Phase 3 ophthalmic trial data. TB-500 fragment has not undergone independent clinical trials. WADA prohibited (Class S0).
Attribute
Typical Dose Range
- Detail
- 2-5 mg per dose, 2-4 times per week during loading; 2-4 mg per week during maintenance. Some protocols use 500-1000 mcg daily.
Attribute
Half-Life
- Detail
- Plasma half-life approximately 0.5-2.1 hours (IV). Biological effects persist for days due to actin pool sequestration mechanism.
Attribute
Cycle Length
- Detail
- 6-8 weeks typical (4 weeks loading, 2-4 weeks maintenance). Some protocols extend to 12-16 weeks. 4-8 week break between cycles.
Attribute
Storage
- Detail
- Lyophilized: -20C or below, protected from light and moisture. Reconstituted: 2-8C, use within 28 days. Do not freeze reconstituted solution.
Overview / What Is TB-500?
The Basics
TB-500 is a synthetic peptide designed to support tissue repair. It is based on the active region of Thymosin Beta-4, a naturally occurring protein found throughout your body in platelets, wound fluid, and developing tissue. Thymosin Beta-4 is one of the most evolutionarily conserved proteins across species; the human version is nearly identical to versions found in fish, amphibians, and mammals, suggesting it plays an ancient and fundamental role in healing.
Where many healing compounds focus on telling your body to start repairing (by triggering growth signals), TB-500 addresses a different bottleneck: it helps the repair cells actually get to where they are needed and organize into functional tissue rather than scar. Think of it as the difference between hiring a construction crew and making sure the road to the construction site is clear and the blueprints are laid out. TB-500 handles the logistics of healing.
An important distinction that often gets overlooked: TB-500 as originally defined is a small 7-amino-acid fragment (positions 17-23 of Thymosin Beta-4). However, most products sold as "TB-500" actually contain the full-length 43-amino-acid Thymosin Beta-4 protein. Anti-doping laboratory analysis has confirmed this directly [1]. Both have tissue repair activity since they share the same active region, but they are not identical compounds. The full-length version contains additional active sites that the fragment lacks. If you want to know which one you have, check the Certificate of Analysis: a molecular weight of approximately 4,900 Da means full-length TB-4, while approximately 800 Da indicates the actual fragment.
The Science
TB-500 (Ac-LKKTETQ) is a synthetic N-terminally acetylated heptapeptide corresponding to amino acids 17-23 of Thymosin Beta-4 (Tb4), a 43-amino acid, 4,963 Da polypeptide belonging to the beta-thymosin family [1][2]. Tb4 is one of the most abundant intracellular peptides in mammalian systems, originally isolated from thymic tissue and subsequently identified in nearly all nucleated cells [3].
As an intrinsically unstructured protein (IUP), Tb4 exists predominantly in an unfolded state in solution, adopting specific conformations only upon binding to target proteins, particularly globular actin (G-actin) [4]. This structural plasticity enables Tb4 to make contact with both the barbed and pointed ends of actin monomers, a critical feature for its role in cytoskeletal regulation.
The LKKTET sequence beginning at residue 17 is the principal actin-binding motif shared between the fragment (TB-500) and the parent molecule (TB-4). A 2012 analysis synthesized and characterized the N-terminal acetylated 17-23 fragment, confirming it as the active component found in commercial TB-500 products, though it also confirmed that many commercial products contain the full-length protein instead [1]. Recent metabolic studies (2024) suggest TB-500 functions partly as a prodrug: serial C-terminal cleavage produces Ac-LKKTE, a pentapeptide metabolite that demonstrated significant independent wound healing activity in cell migration assays [5].
Molecular Identity
Attribute
Common Names
- Detail
- TB-500, Thymosin Beta-4 Fragment 17-23, Ac-LKKTETQ, Fequesetide, TB4 Frag
Attribute
Full-length Parent
- Detail
- Thymosin Beta-4 (Tb4), 43 amino acids
Attribute
Full-length Sequence
- Detail
- SDKPDMAEIEKFDKSKLKKTETQEKNPLPSKETIEQEKQAGES
Attribute
Fragment Sequence (TB-500)
- Detail
- Ac-LKKTETQ (positions 17-23)
Attribute
Molecular Formula (Fragment)
- Detail
- C36H66N10O13
Attribute
Molecular Weight (Fragment)
- Detail
- 846.97 Da (free base); 889.01 Da (acetate salt)
Attribute
Molecular Formula (Full-length)
- Detail
- C212H350N60O78S
Attribute
Molecular Weight (Full-length)
- Detail
- 4,963.44 Da
Attribute
CAS Number (Fragment)
- Detail
- 885340-08-9
Attribute
CAS Number (Full-length)
- Detail
- 77591-33-4
Attribute
PubChem CID (Full-length)
- Detail
- 16132341
Attribute
FDA UNII (Fragment)
- Detail
- QHK6Z47GTG
Attribute
Structural Type
- Detail
- Linear synthetic heptapeptide with N-terminal acetylation
Attribute
Functional Class
- Detail
- Actin-binding peptide, cytoskeletal modulator, tissue regeneration agent, angiogenic peptide
Mechanism of Action
The Basics
Every cell in your body has an internal scaffolding system made of a protein called actin. This scaffolding is what allows cells to move, divide, and change shape. When tissue is damaged, repair cells need to travel to the injury site and rearrange themselves into new, functional tissue. TB-500 helps with both of these processes.
TB-500 binds to the individual building blocks of actin (called monomers) and keeps them in reserve, like a stockpile of construction materials ready to be deployed at a moment's notice. When repair cells need to move to an injury site, they can draw from this reserve to quickly reorganize their internal structure and get moving. Without this stockpile, cells respond sluggishly to repair signals because they have to manufacture new building blocks from scratch.
TB-500 also promotes the growth of new blood vessels, which is how your body delivers oxygen and nutrients to healing tissue. This happens through a different pathway than BPC-157 (which sends the "build new vessels" signal), making the two peptides complementary rather than redundant. TB-500 enables the vessel-building cells to physically move and organize into functional capillaries.
One important caveat: TB-500 (the 7-amino-acid fragment) shares the actin-binding mechanism with full-length Thymosin Beta-4, but the parent molecule contains additional active sites the fragment lacks. Most notably, a 4-amino-acid fragment called Ac-SDKP (positions 1-4 of TB-4) is responsible for anti-fibrotic effects, reducing excessive scar tissue formation. The TB-500 fragment does not contain this sequence and therefore cannot produce this specific effect [6].
The Science
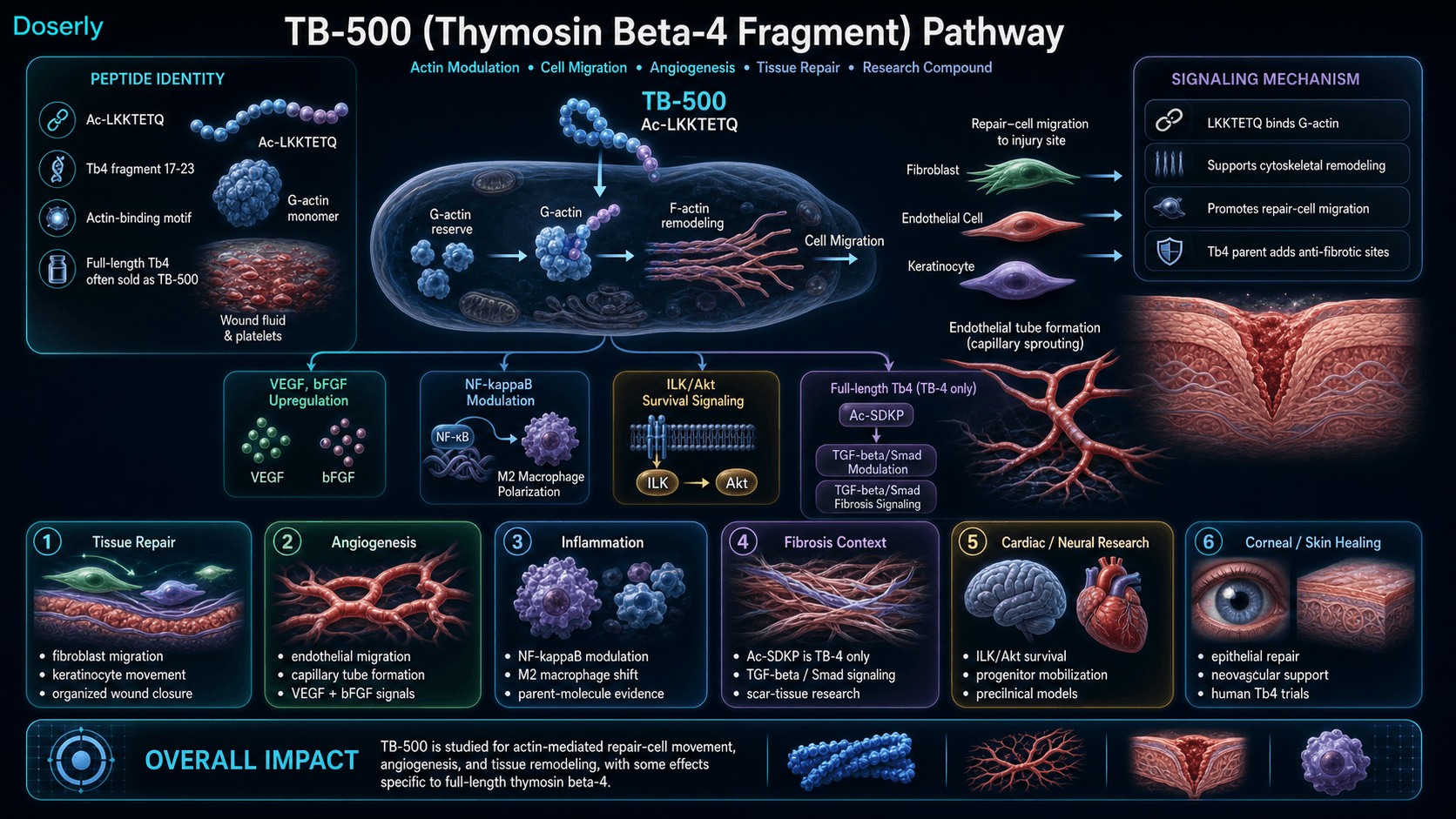
The primary mechanism of TB-500/Tb4 centers on actin sequestration. The LKKTETQ sequence binds G-actin monomers with high affinity, preventing premature polymerization into filamentous actin (F-actin) and maintaining a cytoplasmic reserve pool available for rapid deployment during cell migration, division, and cytoskeletal reorganization [3][7].
Key mechanistic pathways include:
- Actin sequestration and cell migration. Binding to G-actin creates reserve pools that enable fibroblasts, endothelial cells, and keratinocytes to rapidly reorganize their cytoskeleton and migrate to injury sites. The exchange mechanism between Tb4-bound actin and profilin-bound actin represents a critical control point for polymerization dynamics [4].
- Angiogenesis. Fragment 17-23 promotes endothelial cell migration and capillary tube formation, facilitating new blood vessel growth at injury sites [8]. This occurs through VEGF and bFGF upregulation, complementing but mechanistically distinct from BPC-157's VEGFR2-Akt-eNOS signaling pathway.
- Anti-inflammatory modulation. Full-length Tb4 reduces NF-kB activation and pro-inflammatory cytokine production, and promotes macrophage polarization from the pro-inflammatory M1 phenotype to the reparative M2 phenotype [3]. Whether the 17-23 fragment alone drives this effect remains unknown.
- Anti-fibrotic activity (TB-4 only). The N-terminal tetrapeptide Ac-SDKP (positions 1-4), released from TB-4 through a two-step enzymatic cascade involving meprin-alpha and prolyl oligopeptidase (POP), suppresses TGF-beta/Smad2/3 signaling and inhibits myofibroblast differentiation [6][9]. POP cannot cleave full-length Tb4 directly due to its approximately 30-amino-acid structural limit. TB-500 does not contain this sequence.
- Cell survival signaling. Tb4 activates the integrin-linked kinase (ILK)/PINCH-1/Akt pathway, promoting cardiac cell survival after ischemic injury and facilitating progenitor cell mobilization [10].
- DNA repair enhancement. Tb4 interacts with Ku80, enhancing DNA repair mechanisms [3].
A 2021 comprehensive review mapped three distinct active sites within Tb4: fragment 17-23 (LKKTETQ) drives angiogenesis and cell migration; fragment 1-4 (Ac-SDKP) suppresses NF-kB and reduces fibrosis; and fragment 1-15 inhibits caspases 2/3/8/9, providing anti-apoptotic activity [6].
Pathway Visualization Image
Pharmacokinetics
The Basics
TB-500 clears from the bloodstream relatively quickly, with a plasma half-life in the range of 0.5 to 2 hours when given intravenously. However, the way it works means that the biological effects last much longer than the peptide itself stays in circulation. Once TB-500 binds to actin monomers inside cells, those reserves remain available for days, even after the peptide has been cleared from the blood. This is why most protocols use intermittent dosing (two to four times per week) rather than daily injections.
Because TB-500 is a relatively small molecule (approximately 800 Da for the fragment, or approximately 4,900 Da for the commonly sold full-length form), it distributes systemically after subcutaneous injection. Both sizes are well below the approximately 16 kDa threshold for lymphatic absorption, meaning they diffuse directly into blood capillaries rather than being absorbed through the lymphatic system. This rapid systemic distribution is why TB-500 doesn't need to be injected at the exact injury site to have an effect, though local injection provides a higher initial concentration at the target tissue.
The Science
Pharmacokinetic data for TB-500/Tb4 derives primarily from a Phase 1 trial of recombinant human Thymosin Beta-4 (Wang et al., 2021), which enrolled 84 healthy volunteers across single-dose cohorts (0.05-25 ug/kg IV) and multiple-dose cohorts (0.5-5 ug/kg IV daily for 10 days) [11].
Key pharmacokinetic parameters:
- Half-life: Approximately 4 hours based on reference data; 0.5-2.1 hours IV per Phase 1 data [11]
- Peak plasma concentration: Within 30 minutes of subcutaneous injection
- Steady state: Approximately 18 hours with regular dosing
- Route of elimination: 44.6% urinary clearance [12]
- Distribution: Systemic, with rapid distribution to all tissues. Thymosin Beta-4 is highly expressed endogenously in platelets, wound fluid, developing embryonic tissue, and regenerating adult tissue [3]
A critical pharmacokinetic consideration for TB-500 is the distinction between plasma half-life and functional duration. Once TB-500 binds G-actin intracellularly, the sequestered actin pools persist independently of circulating peptide levels. This mass-action binding mechanism explains why milligram-scale bolus dosing 2-3 times per week is preferred over smaller daily doses: peak concentration drives the binding event, and the downstream biological effect self-sustains between administrations [12].
Recent metabolite studies (Yang et al., 2024) identified serial C-terminal cleavage products of TB-500, with the metabolite Ac-LKK demonstrating persistence up to 72 hours [5]. This sustained metabolite presence may contribute to the prolonged biological activity observed beyond plasma clearance.
Research & Clinical Evidence
Wound Healing
The Basics
TB-500's most established research area is wound healing. In animal studies, Thymosin Beta-4 applied to full-thickness skin wounds accelerated closure by 42% at just 4 days and up to 61% at one week compared to controls. The mechanism involves getting repair cells to the wound site faster, growing new blood vessels to supply the area, and laying down organized new tissue rather than chaotic scar.
In humans, a clinical trial of 72 patients with chronic venous ulcers (wounds that resist conventional treatment) tested a topical 0.03% Thymosin Beta-4 gel. Approximately 25% of patients achieved complete wound closure at 3 months [13]. While modest, this is meaningful for wounds that had failed standard care.
The Science
Preclinical wound healing data is extensive. In a rat full-thickness wound model, topical or intraperitoneal Thymosin Beta-4 increased re-epithelialization by 42% over saline controls at day 4 and by 61% at day 7 post-wounding. Wound contraction (dermal approximation) showed 11% improvement by day 7. Histological analysis revealed increased neovascularization and granulation tissue formation, with enhanced collagen deposition [14].
A Phase 2 clinical trial (Treadwell et al.) enrolled 72 patients with chronic venous ulcers across 10 European sites. Treatment with 0.03% Thymosin Beta-4 gel produced approximately 25% complete wound closure at 3 months [13]. A collagen-chitosan scaffold containing TB-4 achieved 93% wound closure at day 21 in diabetic rats with hindlimb ischemia, with confirmed VEGF/AKT pathway activation and significantly increased CD31-positive vessel density (p<0.05) [15].
Corneal Healing
The Basics
The most advanced human evidence for Thymosin Beta-4 comes from eye healing. The cornea is particularly useful for studying TB-4 because it lacks blood vessels, meaning any healing effect must come from direct cellular action rather than improved blood flow.
In a Phase 3 trial of patients with neurotrophic keratopathy (a condition where damaged corneal nerves impair healing), 60% of patients receiving Thymosin Beta-4 achieved complete corneal healing compared to 12.5% on placebo. At day 43, half of treated patients maintained complete healing versus none in the placebo group.
The Science
The SEER-1 Phase 3 trial enrolled 18 patients with neurotrophic keratopathy. 60% (6/10) of Thymosin Beta-4 (RGN-259, 0.1% ophthalmic solution) recipients achieved complete corneal healing versus 12.5% (1/8) placebo. At Day 43, 50% of treated patients maintained complete healing vs 0% placebo (p=0.0359) [16]. Multiple Phase 2/3 trials of RGN-259 for dry eye disease have also demonstrated symptom and sign improvements with acceptable safety profiles.
Cardiac Repair
The Basics
Animal studies have shown that Thymosin Beta-4 can reduce the damage caused by heart attacks. It appears to help heart cells survive the injury, encourages the growth of new blood vessels around the damaged area, and activates progenitor cells that can contribute to cardiac repair. This is one of the most promising research directions for TB-4, though it remains entirely preclinical.
The Science
In a landmark study, Thymosin Beta-4 treatment reduced infarct scar size and improved cardiac function post-myocardial infarction in mice. The mechanism involves activation of the Akt pathway for cardiomyocyte survival and mobilization of cardiac progenitor cells [10]. TB-4 activated integrin-linked kinase (ILK), promoting PINCH1-ILK-parvin complex formation essential for Akt-mediated cell survival and cardiac progenitor cell mobilization [10].
Free systemic TB-4 at the same total dose as a fibrin-targeted nanoparticle formulation produced no functional improvement in cardiac repair, establishing that local tissue concentration above a therapeutic threshold is necessary for efficacy [17].
Neurological Injury
The Basics
Research in rats has found that Thymosin Beta-4 encourages brain and nervous system tissues to repair after injury. In stroke models, treatment with TB-4 improved neurological function, promoted myelin production (the insulating coating on nerves), and stimulated the growth of new precursor cells in the brain. A dose-response study found that lower doses (2 mg/kg) actually outperformed higher doses (18 mg/kg), suggesting a ceiling effect.
TB-4 has also been shown to reduce oxidative stress following spinal cord injury and help transplanted neural stem cells survive long enough to support regeneration.
The Science
In a rat middle cerebral artery occlusion (stroke) model, intraperitoneal TB-4 administered 24 hours post-stroke improved functional outcomes on adhesive removal, modified neurological severity score (mNSS), and foot fault testing. The 2 mg/kg group demonstrated 24-32% relative global improvement. The 18 mg/kg group showed no improvement, establishing a ceiling effect [18]. Mechanisms included increased myelin basic protein expression and proliferation of neural progenitor cells in the striatum. TB-4 has also been shown to attenuate oxidative stress in spinal cord injury models through the TLR4/MyD88 pathway [19].
Hair Growth
The Basics
Hair growth effects were discovered accidentally when researchers noticed that mice genetically lacking Thymosin Beta-4 grew hair back much more slowly after shaving, while mice producing excess TB-4 grew hair back faster with increased numbers of hair shafts and grouped hair follicles. The mechanism likely involves TB-4's ability to stimulate VEGF expression and promote stem cell migration and differentiation in hair follicles.
The Science
TB-4 deficient mice showed significantly delayed hair regrowth compared to wild-type controls. Conversely, mice overexpressing TB-4 demonstrated accelerated hair regrowth with increased hair shaft numbers and grouped follicle formation, attributed to Tb4-induced stem cell migration and differentiation [20].
Antibiotic Synergy
The Basics
An intriguing finding showed that Thymosin Beta-4 combined with a standard antibiotic (ciprofloxacin) worked better than the antibiotic alone against a difficult-to-treat bacterial eye infection. Five days of combined therapy showed decreased bacteria counts, reduced immune cell infiltration, and lower levels of inflammatory molecules. This is the first evidence that TB-4 might enhance the effectiveness of existing antibiotics.
The Science
In a murine Pseudomonas aeruginosa keratitis model, TB-4 combined with ciprofloxacin demonstrated decreased colony-forming units (CFUs), reduced neutrophil counts, and decreased reactive oxygen species compared to antibiotic monotherapy at 5 days [21].
Biomarker Evidence Matrix
Category
Recovery & Healing
- Evidence Strength
- 7/10
- Reported Effectiveness
- 8/10
- Summary
- Extensive preclinical data on wound healing (42-61% improvement in rat models). Phase 2 venous ulcer trial (25% closure). Community strongly endorses for injury recovery, though most reports combine with BPC-157.
Category
Joint Health
- Evidence Strength
- 5/10
- Reported Effectiveness
- 7/10
- Summary
- No joint-specific clinical trials but strong mechanistic basis (actin modulation, angiogenesis). Community reports consistent improvement in joint mobility, stiffness, and load tolerance.
Category
Inflammation
- Evidence Strength
- 6/10
- Reported Effectiveness
- 7/10
- Summary
- Preclinical evidence for NF-kB modulation and M2 macrophage polarization (full-length TB-4). Community reports systemic inflammation reduction. Mechanism well-characterized for parent molecule.
Category
Pain Management
- Evidence Strength
- 4/10
- Reported Effectiveness
- 7/10
- Summary
- No direct analgesic studies. Pain relief likely secondary to tissue repair and inflammation reduction. Community reports significant pain improvement, particularly in chronic injuries.
Category
Physical Performance
- Evidence Strength
- 3/10
- Reported Effectiveness
- 6/10
- Summary
- No performance-specific studies. Performance improvement in community is reported as a recovery outcome, not direct enhancement.
Category
Skin Health
- Evidence Strength
- 6/10
- Reported Effectiveness
- 5/10
- Summary
- Phase 2 wound healing trial in humans. Extensive preclinical wound data. Community discussion focuses on wound healing rather than cosmetic skin effects.
Category
Hair Health
- Evidence Strength
- 4/10
- Reported Effectiveness
- 4/10
- Summary
- Preclinical evidence from TB-4 knockout/overexpression mouse models. No human hair-specific trials. Minimal community reports.
Category
Heart Health
- Evidence Strength
- 5/10
- Reported Effectiveness
- 4/10
- Summary
- Strong preclinical cardiac repair data (Nature, 2004). Phase 1 dose-finding framework for AMI registered. No community-reported cardiac outcomes.
Category
Energy Levels
- Evidence Strength
- 2/10
- Reported Effectiveness
- 5/10
- Summary
- No mechanistic basis for direct energy effects. Mixed community signal (some improved energy, some lethargy).
Category
Side Effect Burden
- Evidence Strength
- 7/10
- Reported Effectiveness
- 8/10
- Summary
- Phase 1 trial (84 volunteers) with no SAEs at doses up to 25 ug/kg/day. Community consistently reports excellent tolerability.
Category
Mood & Wellbeing
- Evidence Strength
- 2/10
- Reported Effectiveness
- 6/10
- Summary
- No direct CNS mechanism. Wellbeing improvements in community likely driven by pain resolution and functional recovery.
Category
Libido
- Evidence Strength
- 1/10
- Reported Effectiveness
- 5/10
- Summary
- No known mechanism. Single community report of increased libido, possibly secondary to general wellbeing improvement.
Categories scored: 12
Categories with community data: 12
Categories not scored (insufficient data): Fat Loss, Muscle Growth, Weight Management, Appetite & Satiety, Food Noise, Sleep Quality, Focus & Mental Clarity, Memory & Cognition, Anxiety, Stress Tolerance, Motivation & Drive, Emotional Aliveness, Emotional Regulation, Sexual Function, Gut Health, Digestive Comfort, Nausea & GI Tolerance, Blood Pressure, Heart Rate & Palpitations, Hormonal Symptoms, Temperature Regulation, Fluid Retention, Body Image, Immune Function, Bone Health, Longevity & Neuroprotection, Cravings & Impulse Control, Social Connection, Treatment Adherence, Withdrawal Symptoms, Daily Functioning
Benefits & Potential Effects
The Basics
TB-500's benefits center on one core capability: supporting your body's ability to repair damaged tissue. Most people explore TB-500 for injury recovery, and the research and community experience both point to this as the primary area of value.
The most commonly reported benefits include reduced morning stiffness in injured areas, faster recovery from tendon and ligament injuries, improved range of motion during rehabilitation, and reduced systemic inflammation. Many users describe it as the peptide that "makes everything else work better" by creating an environment where healing can actually progress rather than stalling.
For people dealing with chronic injuries that have plateaued in their recovery, TB-500 may help restart the healing process by addressing the cell migration bottleneck. Old injury sites that have been tight or painful for months sometimes begin loosening up within the first few weeks.
It is worth noting that TB-500 is almost always discussed alongside BPC-157 in what's known as the "Wolverine Stack." Isolating TB-500's individual contribution from these combined reports is difficult.
The Science
Documented and reported benefits, organized by evidence quality:
Strong preclinical evidence (animal models, multiple studies):
- Accelerated wound closure via enhanced keratinocyte and fibroblast migration [14][8]
- Angiogenesis at injury sites through endothelial cell migration and tube formation [8]
- Reduced fibrosis and scar tissue formation (full-length TB-4 only, via Ac-SDKP) [6][9]
- Cardiac tissue protection and repair following ischemic injury [10]
- Neurological recovery following stroke and spinal cord injury [18][19]
Human clinical evidence (limited):
- Corneal wound healing: 60% complete healing vs 12.5% placebo in Phase 3 neurotrophic keratopathy trial [16]
- Chronic venous ulcer healing: approximately 25% complete closure at 3 months in Phase 2 trial [13]
- Safety at supratherapeutic doses: Phase 1 data showing no SAEs at up to 25 ug/kg/day x 10 days [11]
Community-reported (anecdotal, confounded):
- Reduced joint stiffness and morning pain
- Improved load tolerance during rehabilitation
- Systemic inflammation reduction
- Enhanced recovery speed from surgical procedures and acute injuries
Side Effects & Safety Considerations
The Basics
TB-500 is widely regarded as one of the better-tolerated peptides. Most users report no side effects at all. When side effects do occur, they tend to be mild and temporary: occasional redness or irritation at the injection site, and rare episodes of mild lethargy lasting about a day.
The most important safety consideration is theoretical rather than commonly experienced: because TB-500 promotes the growth of new blood vessels and helps cells migrate, there is a legitimate concern that it could accelerate the growth or spread of existing cancers. This is not a hypothetical risk that researchers have invented for caution's sake; the angiogenic mechanism that makes TB-500 effective for healing is the same mechanism that tumors exploit to grow their own blood supply. For this reason, TB-500 should not be used by anyone with active cancer or a history of malignancy within the past two years.
Educators in the peptide community have emphasized that cycles should be limited in duration and reserved for acute injuries specifically because of this angiogenesis concern with chronic use.
The Science
Phase 1 safety data (full-length TB-4):
84 healthy volunteers received recombinant human Thymosin Beta-4 across single-dose (54 subjects, up to 25 ug/kg IV) and multiple-dose (30 subjects, up to 5 ug/kg daily for 10 days) arms. No serious adverse events (SAEs) and no dose-limiting toxicities were reported. Adverse events were mild to moderate [11]. Dose-proportional pharmacokinetics were observed across the tested range.
Reported side effects (community and literature):
Effect
Injection site reactions (redness, tenderness)
- Frequency
- Occasional
- Severity
- Mild
- Management
- Rotate injection sites; warm peptide to room temperature before injection
Effect
Mild lethargy
- Frequency
- Rare
- Severity
- Mild
- Management
- Hydrate; schedule injections on rest days
Effect
Headache
- Frequency
- Rare
- Severity
- Mild
- Management
- Typically resolves within 24 hours
Contraindications:
Absolute:
- Active cancer or malignancy within 2 years (angiogenesis may promote tumor growth and metastasis)
- Pregnancy or breastfeeding (insufficient safety data)
- Proliferative retinopathy (angiogenesis may worsen pathology)
- Surgery planned or recent (<2 weeks; excessive angiogenesis may complicate surgical wound healing)
Relative (medical supervision recommended):
- Concurrent corticosteroid use (steroids oppose tissue repair mechanisms)
- Severe cardiovascular disease
- Active autoimmune conditions
- Therapeutic anticoagulation
- Diabetic retinopathy (theoretical concern due to angiogenic properties)
Side effect profiles are most useful when you can compare them against your own experience in real time. Doserly lets you log symptoms, severity, and timing alongside your dosing data, creating a side-by-side view of your protocol and your body's response.
This kind of systematic tracking catches things that memory alone misses. A subtle mood shift that began three days after a dose increase. Sleep disruption that correlates with evening administration. These patterns become visible when the data is laid out on a timeline, and they give your healthcare provider actionable information rather than vague concerns. Early detection of emerging side effects means earlier intervention.
Connect protocol changes to labs and health markers.
Doserly can keep lab results, biomarkers, symptoms, and dose history close together so follow-up conversations have better context.
Insights
Labs and trends

Doserly organizes data; it does not diagnose or interpret labs for you.
Dosing Protocols
The Basics
TB-500 dosing works differently from many other peptides because of how it interacts with cells. Rather than sending a signal (like BPC-157, which works at tiny nanogram amounts), TB-500 physically binds to actin molecules one-to-one inside cells. This means you need enough of it in each dose to actually build up those cellular reserves. That is why TB-500 is typically dosed in milligrams rather than micrograms, and why less frequent but larger doses tend to work better than small daily amounts.
Most protocols follow a two-phase structure: a loading phase with higher, more frequent dosing to build up actin reserves during the critical early healing window, followed by a maintenance phase at lower doses to support the slower tissue remodeling that follows.
Sources report a range of protocols. The most commonly cited approach involves:
Loading phase (weeks 1-4): 2-4 mg per dose, administered subcutaneously 2-3 times per week (for example, Monday and Thursday). Some sources report higher loading at 4-8 mg total per week split across 2-4 injections. Others suggest an escalating daily approach starting at 500 mcg and titrating up to 1000 mcg daily.
Maintenance phase (weeks 5-8): 2-4 mg per week in 1-2 injections. Some protocols reduce to every-other-week dosing for ongoing maintenance.
Cycle length: 6-8 weeks is the most frequently cited, with a 4-8 week break between cycles. Some protocols extend to 12 weeks. Educators with safety concerns about chronic angiogenesis recommend a maximum of 12 weeks.
Weight-based reference: Approximately 0.04-0.06 mg/kg per dose has been cited as a reference point, though most protocols use fixed dosing.
It is important to emphasize that these ranges are derived from community practice and preclinical research, not from controlled human clinical trials. There is no established consensus on an optimal dose for any indication. Always consult a healthcare professional before making decisions about any protocol.
The dosing protocols above involve numbers that matter: specific microgram amounts, reconstitution ratios, and timing windows. Getting any of these wrong compounds across every subsequent dose from that vial.
Doserly's dose and reconstitution calculators eliminate the guesswork. Enter your vial size, peptide amount, and target dose, and get the exact bacteriostatic water volume, units per tick mark, and doses per vial. The injection site tracker maps your administration history as a visual heat map across your body, flagging areas that need rest and suggesting rotation patterns. Combined with dose reminders that include compound name, amount, and route, every aspect of your daily protocol is handled with the precision it requires.
Track injection timing, draw notes, and site rotation.
Doserly helps keep syringe-related notes, injection site history, reminders, and reconstitution context together for easier review.
Injection log
Site rotation
Injection logs support record-keeping; follow clinician instructions for administration.
What to Expect
TB-500's effects tend to develop gradually, with initial improvements in stiffness and comfort followed by more substantial changes in tissue function and load tolerance. Individual responses vary based on the severity and chronicity of the injury, dosing protocol, and whether TB-500 is used alone or combined with other compounds (most commonly BPC-157).
Weeks 1-2: Many users report subtle improvements. Morning stiffness begins to decrease. "First-step" pain (the sharp discomfort when you first move an injured area after rest) starts to calm down. Inflammation may begin to subside, with some people reporting a general reduction in systemic stiffness. These early changes are modest but consistent across community reports.
Weeks 2-4: This is typically when people notice more concrete changes. Joint pain decreases further. Range of motion begins improving at injured sites. Tissue planes that had been adhered or restricted start to separate and move more freely. Recovery time between workouts or physical therapy sessions shortens. Some users describe this phase as when "the injury stops being the first thing you think about."
Weeks 4-8: Continued and compounding improvements. Old nagging injuries feel noticeably better. Eccentric loading tolerance increases, meaning you can progressively load injured tissue without triggering setbacks. Range of motion keeps improving. For people using the Wolverine Stack (BPC-157 + TB-500), this phase is often described as when the synergy between the two peptides becomes most apparent.
Weeks 8-12 (extended protocols): Full benefits realized. Inflammation management becomes consistent. Chronic issues that have lingered for months or years may show meaningful resolution. This timeline is more relevant for severe or long-standing injuries.
Acute injuries generally respond faster than chronic ones. For fresh muscle tears or post-surgical recovery, meaningful improvement can begin within the first two weeks. Chronic injuries that have been present for months or years may need the full 6-8 week course, and sometimes benefit from repeat cycles after a break.
Timelines are useful benchmarks, but they mean more when you're tracking your own progress against them. Doserly lets you log daily observations alongside your protocol data, creating a personal timeline that runs parallel to the general expectations above.
When you reach the 4-week or 8-week assessment points, you'll have more than a feeling to work with. You'll have a documented record of how each week progressed, what changed, and when. This makes protocol decisions concrete: whether to extend a cycle, adjust a dose, or try a different approach, the data is there to support the conversation with your healthcare provider rather than relying on recall.
See where a dose, cycle, or change fits in time.
Doserly gives each protocol a timeline so dose changes, pauses, restarts, and observations are easier to compare later.
Timeline
Cycle history

Timeline tracking helps with recall; it is not a treatment recommendation.
Interaction Compatibility
Good With (Synergistic)
- BPC-157 — The most commonly used combination ("Wolverine Stack"). BPC-157 restores blood flow via VEGF upregulation; TB-500 enables cell migration and tissue organization. They address different bottlenecks in the healing cascade. Protocol: BPC-157 500-750 mcg daily + TB-500 2-4 mg 2x/week.
- GHK-Cu — Optimizes collagen quality and matrix composition during the remodeling phase. Front-load TB-500 weeks 1-8, layer GHK-Cu weeks 3-12+. Particularly useful when scar appearance matters.
- KPV — Anti-inflammatory peptide that silences inflammatory signaling without immunosuppression. Useful when tissue stays inflamed despite repair. TB-500 2 mg 2-4x/week + KPV 250-500 mcg daily.
- NAD+ — Supports mitochondrial function for energy-intensive healing processes. TB-500 per protocol + NAD+ IM 100-300 mg mid-day.
- SS-31 — Mitochondrial support for sustained repair processes.
- MOTS-C — Metabolic support during recovery periods.
- Glutathione — Antioxidant support listed as compatible in community protocols.
- Thymosin Alpha-1 — Immune modulation support; compatible with TB-500's tissue repair focus.
- LL-37 — Antimicrobial peptide; compatible for wound healing contexts.
- VIP — Anti-inflammatory neuropeptide; listed as compatible in community stacking protocols.
Blends
- BPC-157 + TB-500 Blend — Pre-mixed Wolverine Stack formulation.
- Wolverine Blend — Extended Wolverine formulation.
- GLOW — Multi-compound blend including BPC-157, TB-500, GHK-Cu.
- KLOW — Full 5-compound protocol including BPC-157, TB-500, KPV, GHK-Cu.
Not Good With (Contraindicated or Cautionary)
- Corticosteroids — Steroids oppose tissue repair mechanisms that TB-500 promotes. Concurrent use may reduce efficacy.
- Anti-angiogenic medications — Direct mechanistic conflict with TB-500's pro-angiogenic activity.
- Immunosuppressants — May interfere with macrophage polarization effects.
Administration Guide
Materials typically required:
- Insulin syringes (U-100, 29-31 gauge)
- Alcohol swabs (70% isopropyl)
- Bacteriostatic water for reconstitution
- Sharps disposal container
Recommended reconstitution solution: Bacteriostatic water (0.9% benzyl alcohol) is the standard. For a 5 mg vial, 3.0 mL of bacteriostatic water produces a concentration of approximately 1.67 mg/mL, providing convenient measurement on a U-100 insulin syringe (30 units = approximately 500 mcg). For a 10 mg vial, 3.0 mL produces approximately 3.33 mg/mL.
Timing considerations: TB-500 does not have strict timing requirements relative to meals, sleep, or exercise. Most practitioners recommend choosing a consistent time and maintaining that schedule. When using the Wolverine Stack with BPC-157 on the same day, some sources recommend administering at different injection sites.
Post-administration care: Monitor for injection site reactions (redness, swelling). Mild soreness at the injection site is common and typically resolves within hours. Report any unusual reactions, significant pain, or signs of infection to a healthcare provider.
Supplies & Planning
Typical supplies associated with TB-500 protocols:
- Peptide vials: TB-500 is commonly available in 5 mg and 10 mg vial sizes. Vial selection depends on protocol requirements.
- Bacteriostatic water: Standard reconstitution solution. Available in 10 mL and 30 mL vials. Each peptide vial typically requires 2-3 mL for reconstitution.
- Insulin syringes: U-100 syringes, 29-31 gauge, 0.5 or 1 mL capacity. A new syringe should be used for each injection.
- Alcohol swabs: For sterilizing vial stoppers and injection sites.
- Sharps container: For safe disposal of used syringes.
- Storage: Refrigerator space for reconstituted vials.
Specific quantities depend on the protocol determined in consultation with a healthcare provider. Use the reconstitution calculator for preparation math.
Storage & Handling
Lyophilized (powder) form:
- Store at -20C (-4F) or below for long-term storage (up to 2-3 years)
- Short-term storage at 2-8C (35.6-46.4F) is acceptable for weeks to months
- Keep in original sealed packaging with desiccant
- Store in a dry, dark environment; peptides are hygroscopic and light-sensitive
- Allow vials to reach room temperature before opening to prevent condensation
Reconstituted (liquid) form:
- Refrigerate immediately at 2-8C (35.6-46.4F) after reconstitution
- Use within 28 days when reconstituted with bacteriostatic water (0.9% benzyl alcohol)
- Do NOT freeze reconstituted solution; freezing denatures peptides
- Avoid repeated freeze-thaw cycles; each cycle can reduce potency by 25% or more
- Inspect for clarity before each use; discard if cloudy, discolored, or containing particles
Handling best practices:
- Use aseptic technique when drawing from vials (clean stopper with alcohol, use sterile needles)
- Label reconstitution date on each vial
- Protect from direct sunlight and heat sources
Lifestyle Factors
TB-500's tissue repair mechanisms work best when supported by lifestyle factors that complement the healing process:
Protein intake: Adequate protein is essential during tissue repair. The repair process requires amino acids for collagen synthesis, cell division, and matrix remodeling. Most practitioners recommend prioritizing protein intake during TB-500 cycles.
Physical activity: Gentle, targeted movement and rehabilitation exercises promote blood flow to injured areas and stimulate the cellular processes that TB-500 supports. However, overtraining during injury recovery can be counterproductive. Progressive loading should follow the injury's healing trajectory rather than pushing ahead of it.
Sleep: 7-9 hours of quality sleep supports the body's natural regenerative processes. Growth hormone release during deep sleep contributes to tissue repair. Some users schedule TB-500 injections in the evening to align with nocturnal recovery cycles.
Hydration: Adequate hydration supports systemic circulation and nutrient delivery to healing tissues. This is particularly relevant given TB-500's angiogenic mechanism, which creates new blood vessel networks that require adequate fluid volume to function.
Monitoring: Community sources recommend tracking hs-CRP (inflammation marker), comprehensive metabolic panel (electrolytes, kidney, liver function), and ALT/AST during cycles, particularly for longer protocols.
Regulatory Status & Research Classification
United States (FDA): TB-500 (Thymosin Beta-4 fragment) is not FDA-approved for any indication. Full-length Thymosin Beta-4 has been investigated in clinical trials, including Phase 1 safety studies and Phase 2/3 ophthalmic trials (RGN-259 for dry eye disease and neurotrophic keratopathy). A dose-finding trial framework in acute myocardial infarction (RGN-352) was registered. TB-500 is classified as a research compound. It is not a controlled substance.
WADA (World Anti-Doping Agency): TB-500 is prohibited for competitive athletes under Class S0: Non-Approved Substances. Testing protocols can detect TB-500 metabolites in urine [1][5]. Professional leagues including the NFL, NBA, MLB, and FIFA have adopted similar restrictions.
Other jurisdictions: Regulatory status varies. TB-500 is generally available through research peptide suppliers and some compounding pharmacies in jurisdictions where research compounds are legally purchasable. Specific country-by-country regulatory details are limited for TB-500 as a research compound.
Active clinical trials: Clinical trial activity has primarily focused on full-length Thymosin Beta-4 rather than the TB-500 fragment. Registered trials include ophthalmological indications (RGN-259), cardiovascular indications (RGN-352), and Phase 1 safety studies. No clinical trials specifically evaluating TB-500 (the fragment) for injectable therapeutic use have been registered as of 2026.
Regulatory status changes frequently. Always verify the current legal status of any compound in your specific country or jurisdiction before making any decisions.
FAQ
What is the difference between TB-500 and TB-4 (Thymosin Beta-4)?
TB-500 was originally defined as the 7-amino-acid fragment (positions 17-23, sequence LKKTETQ) of Thymosin Beta-4, with a molecular weight of approximately 800 Da. Full-length TB-4 is the complete 43-amino-acid protein at approximately 4,900 Da. Anti-doping laboratory analysis has confirmed that many products labeled "TB-500" actually contain full-length TB-4 [1]. Both share the actin-binding active region, but full-length TB-4 contains additional active sites including the Ac-SDKP anti-fibrotic fragment. A Certificate of Analysis can clarify which compound you have based on molecular weight.
What dosing ranges are reported in the literature for TB-500?
Based on available sources, commonly reported ranges include 2-4 mg per dose administered 2-3 times per week during a loading phase of 4 weeks, followed by 2-4 mg per week for maintenance. Some protocols use 500-1000 mcg daily with gradual titration. There is no established consensus, and these ranges are derived from community practice and preclinical research rather than controlled human dosing studies. Consult a healthcare professional for guidance specific to your situation.
Can TB-500 be used for old or chronic injuries?
Community reports suggest that TB-500 remains effective even months or years post-injury. Chronic injuries often have multiple stalled bottlenecks in the repair process, and TB-500 addresses the cell migration and organization component. Complete resolution of long-standing injuries may require addressing other bottlenecks as well, which is why many practitioners combine TB-500 with BPC-157 (perfusion), KPV (inflammation), or GHK-Cu (collagen quality).
Does TB-500 need to be cycled?
Based on available data, most sources recommend cycling TB-500 rather than continuous use. Typical protocols suggest 6-8 weeks on followed by 4-8 weeks off. The cycling structure serves two purposes: it allows assessment of whether the peptide is contributing to recovery, and it limits duration of pro-angiogenic exposure given the theoretical cancer risk concern with chronic use. Educators emphasizing safety suggest a maximum of 12 consecutive weeks.
Where is TB-500 typically administered?
Most sources recommend subcutaneous injection near the injury site when possible. For deeper musculoskeletal injuries, intramuscular injection may be preferred. For hard-to-reach injuries (spine, deep hip), abdominal or thigh injection is described as the practical alternative. The peptide enters systemic circulation regardless of injection site, but local injection provides a higher first-pass concentration at the target tissue, which may be meaningful given TB-500's concentration-dependent mass-action mechanism [17].
Can TB-500 and BPC-157 be combined in one syringe?
Based on community and practitioner reports, the two peptides are pH compatible and are commonly co-injected. Some sources recommend separate syringes if there is uncertainty about stability with a specific formulation.
What if there is no response to TB-500?
Commonly discussed factors include: insufficient dose (some sources suggest increasing frequency to 3-4x weekly), degraded peptide (verify storage conditions), missing complementary mechanism (consider adding BPC-157 for perfusion or KPV for inflammation), inadequate duration (chronic injuries may require 8+ weeks), or an underlying structural issue that requires imaging and a different intervention.
Sources & References
[1] Esposito S, et al. "Synthesis and characterization of the N-terminal acetylated 17-23 fragment of thymosin beta 4 identified in TB-500, a product suspected to be used in horse doping." Drug Test Anal. 2012;4(9):733-738. PMID 22962027. https://pubmed.ncbi.nlm.nih.gov/22962027/
[2] "Doping control analysis of TB-500, a synthetic version of an active region of thymosin." Drug Test Anal. 2013. PMID 23084823. https://pubmed.ncbi.nlm.nih.gov/23084823/
[3] Goldstein AL, et al. "Thymosin beta4: actin-sequestering protein moonlights to repair injured tissues." Trends Mol Med. 2005;11(9):421-429. PMID 16099219. https://pubmed.ncbi.nlm.nih.gov/16099219/
[4] Lappalainen P, Drubin DG. "Cofilin promotes rapid actin filament turnover in vivo." Nature. 1997;388(6644):78-82. Additional structural characterization in: Hertzog M, et al. "Molecular basis for the dual function of Eps8 on actin dynamics." J Biol Chem. 2010;285(44):34001-34013.
[5] Yang Y, et al. "Simultaneous quantification of TB-500 and its metabolite Ac-LKKTE in human serum with wound healing activity screening." Drug Test Anal. 2024;16(10):1248-1258. PMID 38382158. https://pubmed.ncbi.nlm.nih.gov/38382158/
[6] Xing Y, et al. "Progress on the Function and Application of Thymosin beta4." Front Endocrinol. 2021;12:767785. PMC8724243. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8724243/
[7] Philp D, et al. "Thymosin beta4 promotes angiogenesis, wound healing, and hair follicle development." Mech Ageing Dev. 2004;125(2):113-115. PMID 15037011. https://pubmed.ncbi.nlm.nih.gov/15037011/
[8] Philp D, Goldstein AL, Kleinman HK. "Thymosin beta4 promotes wound healing and hair growth." Expert Opin Biol Ther. 2004;4(7):1017. DOI: 10.1517/14712598.4.7.1017. https://pubmed.ncbi.nlm.nih.gov/15268670/
[9] Kumar N, Bhatt DL. "Meprin beta metalloproteases release N-acetyl-seryl-aspartyl-lysyl-proline from thymosin beta4." Kidney Int. 2016;89(6):1138-1150. PMC4889319. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4889319/
[10] Bock-Marquette I, et al. "Thymosin beta4 activates integrin-linked kinase and promotes cardiac cell migration, survival, and cardiac repair." Nature. 2004;432(7016):466-472. PMID 15282614. https://pubmed.ncbi.nlm.nih.gov/15282614/
[11] Wang D, et al. "Phase I study of recombinant human thymosin beta4." Ann Transl Med. 2021;9(15):1232. PMC8419156. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8419156/
[12] Mora CA, et al. "Biodistribution of synthetic thymosin beta 4 in the serum, urine, and major organs of mice." Int J Immunopharmacol. 1997;19(1):1-8. PMID 9226473. https://pubmed.ncbi.nlm.nih.gov/9226473/
[13] Treadwell T, et al. "Thymosin beta-4 and venous ulcer healing." Ann N Y Acad Sci. 2007. PMID 17495250. https://pubmed.ncbi.nlm.nih.gov/17495250/
[14] Malinda KM, et al. "Thymosin beta4 accelerates wound healing." J Invest Dermatol. 1999;113(3):364-368. PMID 10469335. https://pubmed.ncbi.nlm.nih.gov/10469335/
[15] Ti D, et al. "Controlled release of thymosin beta 4 using a collagen-chitosan sponge scaffold augments cutaneous wound healing and increases angiogenesis in diabetic rats with hindlimb ischemia." Tissue Eng Part A. 2015;21(3-4):541-549. PMID 25204972. https://pubmed.ncbi.nlm.nih.gov/25204972/
[16] Sosne G, et al. "0.1% RGN-259 (Thymosin beta4) Ophthalmic Solution Promotes Healing in Neurotrophic Keratopathy: Phase III Clinical Trial." Int J Mol Sci. 2022. PMC9820614. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9820614/
[17] Huang G, et al. "Targeted delivery of thymosin beta 4 to the injured myocardium using CREKA-conjugated nanoparticles." Int J Nanomedicine. 2017;12:3023-3036. PMC5396927. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5396927/
[18] Chopp M, Zhang ZG. "Thymosin beta4 as a restorative/regenerative therapy for neurological injury and neurodegenerative diseases." Expert Opin Biol Ther. 2015;15 Suppl 1:S9-12. PMID 26096836. https://pubmed.ncbi.nlm.nih.gov/26096836/
[19] Li H, et al. "Thymosin beta 4 attenuates oxidative stress-induced injury of spinal cord-derived neural stem/progenitor cells through the TLR4/MyD88 pathway." Gene. 2019;707:136-142. PMID 30981886. https://pubmed.ncbi.nlm.nih.gov/30981886/
[20] Philp D, et al. "Thymosin beta 4 induces hair growth via stem cell migration and differentiation." Ann N Y Acad Sci. 2007;1112:95-103. PMID 17496058. https://pubmed.ncbi.nlm.nih.gov/17496058/
[21] Carion TW, et al. "Thymosin Beta-4 and Ciprofloxacin Adjunctive Therapy Improves Pseudomonas aeruginosa-Induced Keratitis." Cells. 2018;7(10). PMID 30287720. https://pubmed.ncbi.nlm.nih.gov/30287720/
[22] Bock-Marquette I, Shrivastava S, Bhaumik A, et al. "Thymosin beta4 activates integrin-linked kinase." Circ Res. 2009. DOI: 10.1161/CIRCRESAHA.109.200907. https://pubmed.ncbi.nlm.nih.gov/19325145/
Related Peptide Guides
- BPC-157 — The most commonly stacked companion. Local repair peptide that restores blood flow to damaged tissue via VEGF upregulation.
- BPC-157 + TB-500 Blend — Pre-mixed Wolverine Stack formulation.
- Wolverine Blend — Extended Wolverine healing formulation.
- GHK-Cu — Copper peptide for collagen quality, matrix remodeling, and scar appearance.
- KPV — Anti-inflammatory tripeptide for persistent inflammation.
- NAD+ — Cellular energy support for energy-intensive healing processes.
- SS-31 — Mitochondrial-targeted peptide for cellular energy support.
- MOTS-C — Mitochondrial-derived peptide for metabolic support during recovery.
- Thymosin Alpha-1 — Immune modulation peptide from the same thymosin family.
- LL-37 — Antimicrobial peptide compatible with wound healing protocols.
- Glutathione — Antioxidant support peptide.
- VIP — Anti-inflammatory neuropeptide.
- GLOW — Multi-compound healing blend including TB-500.
- KLOW — Full 5-compound protocol including TB-500.
Need the reconstitution math for TB-500 (Thymosin Beta-4 Fragment): Complete Research Guide?
Open the calculator with TB-500 (Thymosin Beta-4 Fragment): Complete Research Guide prefilled to estimate concentration, draw volume, and related measurement math from the reconstitution details you already have.