Cagrilintide: Complete Research Guide
On this page
Quick Reference Card
Attribute
Also Known As
- Detail
- AM833, NN9838, CagriSema (when combined with semaglutide)
Attribute
Administration
- Detail
- Injectable (subcutaneous, once weekly)
Attribute
Research Status
- Detail
- Investigational, Phase 3. NDA filed December 2025; FDA decision anticipated late 2026. Not FDA-approved.
Attribute
Typical Dose Range
- Detail
- 0.25-4.5 mg once weekly (monotherapy); 0.25-2.4 mg once weekly (CagriSema combination)
Attribute
Half-Life
- Detail
- Approximately 159-195 hours (7-8 days)
Attribute
Cycle Length
- Detail
- 12-68+ weeks (based on clinical trial durations)
Attribute
Storage
- Detail
- Lyophilized: -20 C (-4 F); Reconstituted: 2-8 C (35.6-46.4 F), use within 30 days. Requires acidic pH (3.5-4.5) for optimal stability.
Overview / What Is Cagrilintide?
The Basics
Cagrilintide is a once-weekly injectable compound designed to reduce appetite and support weight management. It works by mimicking amylin, a natural hormone your pancreas releases alongside insulin every time you eat. While GLP-1 medications like semaglutide and tirzepatide have dominated conversations about metabolic peptides, cagrilintide targets a different pathway entirely. Amylin works in the brain's satiety centers to tell you that you are full, slows down how quickly food leaves your stomach, and helps control blood sugar spikes after meals.
Novo Nordisk, the same company behind Ozempic and Wegovy, developed cagrilintide and is studying it both on its own and in combination with semaglutide under the name CagriSema. The combination approach is based on a simple idea: if two different hormones both contribute to feeling full through separate mechanisms, activating both at the same time should produce a stronger effect than either one alone. Clinical trial results have supported this hypothesis, with CagriSema producing some of the largest weight loss numbers seen in obesity research to date.
As of early 2026, cagrilintide is not approved by any regulatory agency for human use. Novo Nordisk filed a New Drug Application with the FDA in December 2025, and a decision is expected by late 2026.
The Science
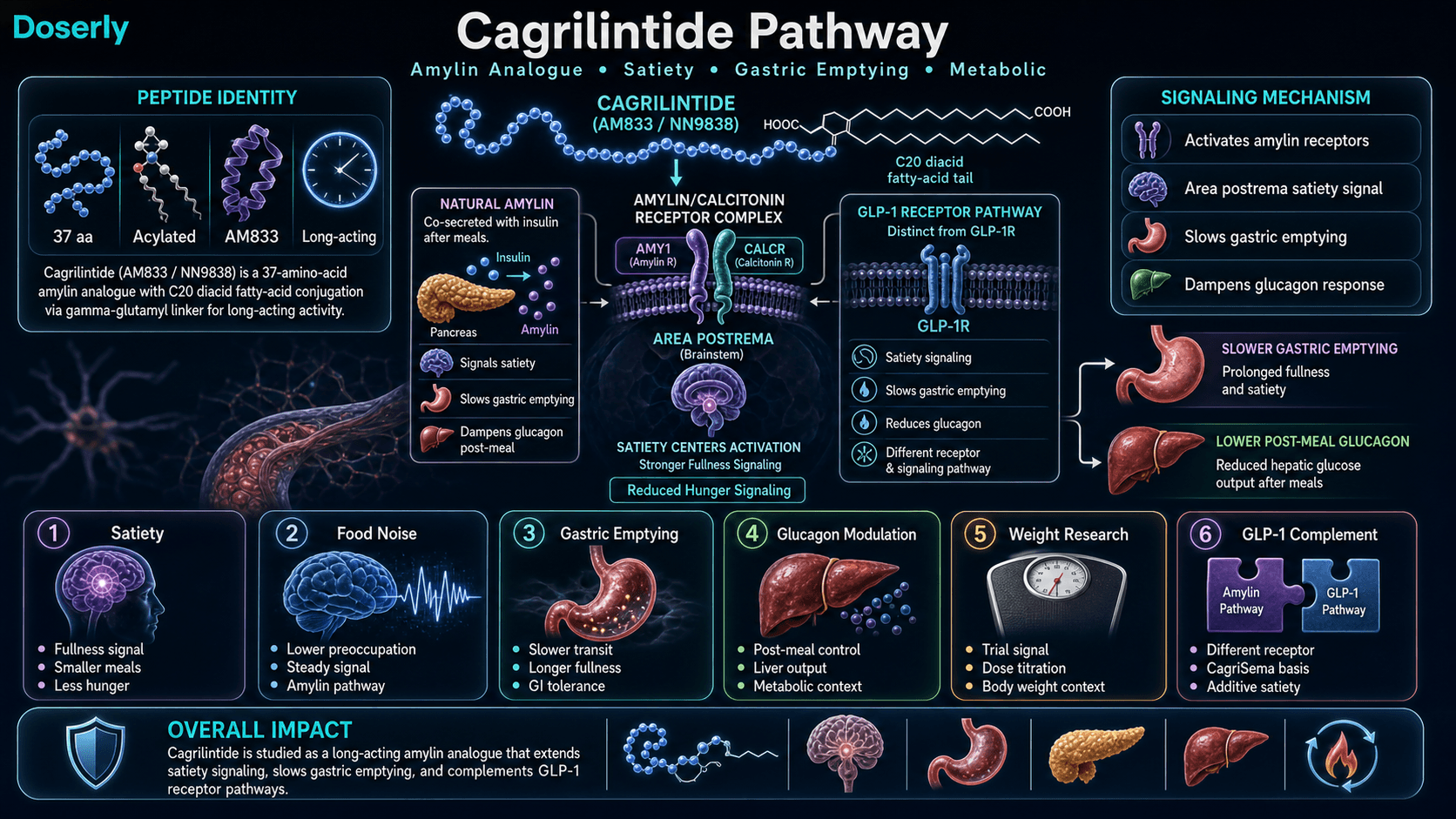
Cagrilintide is a long-acting acylated analogue of human amylin, classified as a dual amylin and calcitonin receptor agonist (DACRA). It was designed by optimizing the human amylin backbone with calcitonin-inspired structural modifications and fatty acid acylation to extend its pharmacological half-life from the minutes-range of native amylin to approximately 159-195 hours, enabling once-weekly subcutaneous administration [1][2].
Native amylin (islet amyloid polypeptide, IAPP) is a 37-amino acid peptide co-secreted with insulin from pancreatic beta cells in response to nutrient ingestion [3][4]. It acts primarily on the area postrema and nucleus tractus solitarius (NTS) in the brainstem to promote satiation, delay gastric emptying, and suppress postprandial glucagon secretion [3][5]. Cagrilintide retains these pharmacological activities while providing sustained receptor engagement through its extended half-life.
The compound activates both amylin receptors (formed by the calcitonin receptor complexed with receptor activity-modifying proteins, CTR + RAMPs) and calcitonin receptors, placing it in the DACRA class [1]. In the phase 2 dose-finding trial published in The Lancet (2021), cagrilintide 4.5 mg weekly produced 10.8% mean body weight loss over 26 weeks compared to 3.0% with placebo (n=706) [6]. When combined with semaglutide 2.4 mg in the phase 3 REDEFINE 1 trial, co-administered cagrilintide and semaglutide achieved approximately 22.7% weight loss at 68 weeks [7].
Molecular Identity
Attribute
Common Names
- Detail
- Cagrilintide, AM833, NN9838
Attribute
Structural Class
- Detail
- Long-acting acylated amylin analogue; dual amylin and calcitonin receptor agonist (DACRA)
Attribute
Amino Acid Length
- Detail
- 37 amino acids
Attribute
Key Structural Modification
- Detail
- C20 diacid fatty acid conjugated at the N-terminus via a gamma-glutamyl linker
Attribute
Developer
- Detail
- Novo Nordisk
Note: The molecular weight of cagrilintide varies in published sources depending on whether the acylation modification and counterion are included. Reported values range from approximately 3,800 Da to 4,409 Da. The higher value likely reflects the complete modified molecule including the C20 diacid fatty acid chain and linker.
Mechanism of Action
The Basics
To understand cagrilintide, it helps to know about amylin. Every time you eat and your pancreas releases insulin to handle blood sugar, it also releases amylin. Amylin's job is to act as a brake on eating: it signals the brain's satiety center (an area called the area postrema) to tell you that you are full, it slows down how quickly food empties from your stomach so you feel satisfied longer, and it dampens the release of glucagon, a hormone that would otherwise raise blood sugar after meals.
Cagrilintide is an engineered version of amylin that lasts much longer in the body. While natural amylin breaks down within minutes, cagrilintide's molecular modifications keep it active for about a week. Think of it as turning a quick signal into a sustained broadcast. Your satiety center receives a steady "you're full" message instead of a brief pulse after each meal.
What makes this mechanism distinct from GLP-1 medications is that amylin and GLP-1 work through different receptors and different brain regions. They are complementary rather than redundant. This is the scientific basis for CagriSema: when you activate both the amylin pathway and the GLP-1 pathway simultaneously, appetite suppression becomes stronger and more consistent than either pathway alone.
The Science
Cagrilintide exerts its primary pharmacological effects through activation of amylin receptors (AMY1, AMY2, AMY3) and the calcitonin receptor (CTR). The amylin receptors are heterodimeric complexes formed by the calcitonin receptor coupled with receptor activity-modifying proteins (RAMP1, RAMP2, or RAMP3). These receptors are expressed predominantly in the area postrema (AP) and nucleus tractus solitarius (NTS) of the hindbrain [3][5].
Receptor activation triggers several downstream effects:
Central satiety signaling. Amylin receptor activation in the AP/NTS enhances satiety signaling and reduces meal size by modulating neuronal firing patterns that communicate with higher-order hypothalamic appetite circuits [5][8]. This mechanism is mechanistically distinct from GLP-1 receptor-mediated appetite suppression, which primarily operates through the hypothalamic arcuate nucleus and ventromedial hypothalamus.
Gastric emptying delay. Cagrilintide slows gastric motility through vagal afferent pathways, extending the period of postprandial gastric distension and prolonging meal-associated satiety signals [3][9].
Postprandial glucagon suppression. Activation of amylin receptors in the pancreatic islets and centrally suppresses inappropriate glucagon secretion following meals, contributing to improved glycemic control [4][9].
Calcitonin receptor agonism. The dual receptor activity (amylin + calcitonin) may contribute additional satiety signaling, though the relative contribution of calcitonin receptor activation versus pure amylin receptor activation to weight loss remains an active area of investigation [1].
The mechanistic rationale for combining cagrilintide with semaglutide is that amylin and GLP-1 activate distinct receptor populations through separate signaling pathways, producing additive or synergistic effects on appetite and energy intake. In the REDEFINE 1 trial, CagriSema (20.4% mean weight loss) exceeded both cagrilintide monotherapy (11.8%) and semaglutide monotherapy (16.1%) at 68 weeks [7].
Pathway Visualization Image
Pharmacokinetics
The Basics
Cagrilintide is designed for once-weekly dosing, and its pharmacokinetics explain why. After a subcutaneous injection, the compound reaches its peak concentration in the blood within about two days. It then stays active for approximately seven to eight days before dropping to half its peak level (the half-life). This long duration means a single weekly injection provides relatively steady coverage without significant peaks and valleys.
The compound needs to build up in your system over several weeks of regular dosing. Because each weekly dose partially overlaps with the previous one, it takes about four to five weeks of consistent injections to reach what pharmacologists call steady state, the point where the amount entering your body each week roughly equals the amount being cleared. This buildup period is one reason clinical protocols use gradual dose escalation over weeks rather than starting at the full target dose.
The Science
Key pharmacokinetic parameters for cagrilintide following subcutaneous administration [2][10]:
- Time to peak concentration (Tmax): Approximately 48 hours (2 days) post-injection
- Elimination half-life (t1/2): 159-195 hours (approximately 7-8 days)
- Steady-state attainment: Approximately 4-5 weeks with weekly dosing
- Total clearance: Estimated at approximately 37.5 days for complete elimination
The extended half-life is a product of the C20 diacid fatty acid acylation at the N-terminus, which promotes binding to serum albumin. Albumin association reduces renal clearance and proteolytic degradation, enabling the sustained pharmacological profile that supports once-weekly administration [2]. This pharmacokinetic strategy mirrors the approach used for semaglutide (C-18 fatty diacid) and other acylated peptide therapeutics.
The long half-life has clinical implications for dose titration. Because of accumulation over multiple dosing intervals, the effective exposure at any given weekly dose continues to increase during the first four to five weeks. This means that side effects may emerge or intensify during weeks two through four even without a dose increase, and is a key reason for conservative titration schedules [6].
Research & Clinical Evidence
Cagrilintide and Weight Loss
The Basics
The weight loss data for cagrilintide comes primarily from Novo Nordisk's clinical trial program. In the first large study (a phase 2 trial with 706 adults), the highest dose of cagrilintide alone (4.5 mg weekly) produced about 10.8% body weight loss over 26 weeks. To put that in perspective, for someone weighing 220 pounds, that translates to roughly 24 pounds over six months.
The combination with semaglutide tells a more dramatic story. In the phase 3 REDEFINE 1 trial, CagriSema (2.4 mg cagrilintide plus 2.4 mg semaglutide, once weekly) produced approximately 22.7% weight loss at 68 weeks. About 40% of patients lost at least 25% of their body weight, a result described as unprecedented in obesity pharmacotherapy. In a second trial for people with type 2 diabetes (REDEFINE 2), CagriSema achieved about 15.7% weight loss at 68 weeks.
However, in a head-to-head comparison (REDEFINE 4), tirzepatide 15 mg outperformed CagriSema, achieving approximately 25.5% weight loss versus 23% for CagriSema at 84 weeks. CagriSema failed to meet the primary endpoint of non-inferiority to tirzepatide in this trial.
The Science
Phase 2 dose-finding trial (NCT03856047): Lau et al. (2021), published in The Lancet. Randomized, double-blind, placebo-controlled trial involving 706 adults with overweight or obesity. Cagrilintide administered weekly at doses of 0.3, 0.6, 1.2, 2.4, or 4.5 mg for 26 weeks. Mean body weight change from baseline: -10.8% at 4.5 mg versus -3.0% with placebo. Dose-dependent weight loss was observed across all dose groups [6].
Phase 3 REDEFINE 1 (NCT05394519): Co-administered cagrilintide 2.4 mg and semaglutide 2.4 mg once weekly in adults with overweight or obesity without type 2 diabetes. At 68 weeks, CagriSema produced approximately 22.7% mean weight loss versus 2.4% with placebo. Approximately 40% of CagriSema patients achieved 25% or greater weight reduction [7].
Phase 3 REDEFINE 2 (NCT05394519): Cagrilintide-semaglutide in adults with overweight or obesity and type 2 diabetes. At 68 weeks, CagriSema produced approximately 15.7% mean weight loss versus -3.4% with placebo (estimated difference: -10.4 percentage points, p<0.001). Significant improvements in glycemic measures were also observed [11].
Phase 3 REDEFINE 4: Open-label, head-to-head trial comparing CagriSema to tirzepatide 15 mg over 84 weeks. Tirzepatide achieved 23.6-25.5% weight loss (depending on estimand) versus 20.2-23% for CagriSema. CagriSema failed to meet the primary non-inferiority endpoint [12].
Phase 1b combination study (Enebo et al., 2021): Published in The Lancet. Established the safety, tolerability, and pharmacokinetic profile of cagrilintide co-administered with semaglutide, providing the foundation for the CagriSema program [10].
Cagrilintide and Glycemic Control
The Basics
Because amylin is naturally involved in blood sugar regulation, cagrilintide also appears to improve measures of glycemic control. In trials involving people with type 2 diabetes, the combination with semaglutide improved HbA1c (a measure of average blood sugar over the past two to three months) and fasting glucose levels. These improvements are partly a direct pharmacological effect and partly a downstream consequence of weight loss itself.
The Science
In the REDEFINE 2 trial, CagriSema produced significant improvements in glycated hemoglobin (HbA1c) compared to placebo in adults with type 2 diabetes. The proportion of patients achieving HbA1c below 7% was substantially higher in the CagriSema group. These glycemic improvements exceeded those typically seen with semaglutide monotherapy at the same dose, suggesting an additive contribution from cagrilintide's amylin receptor activation [11]. Native amylin contributes to glycemic control through suppression of postprandial glucagon secretion and delay of gastric emptying [4][9].
Biomarker Evidence Matrix
Only categories with sufficient data from KB sources and community reports are scored. Evidence Strength reflects the quality of available clinical and preclinical data. Reported Effectiveness reflects community-reported outcomes from sentiment analysis.
Category
Appetite & Satiety
- Evidence Strength
- 9/10
- Reported Effectiveness
- 8/10
- Summary
- Strong clinical evidence from multiple RCTs demonstrating significant appetite reduction. Community consistently reports profound appetite suppression, particularly when stacked with GLP-1 compounds.
Category
Food Noise
- Evidence Strength
- 7/10
- Reported Effectiveness
- 7/10
- Summary
- Moderate clinical support through amylin's central satiety mechanism. Community reports meaningful reduction in food preoccupation and reward-driven eating.
Category
Fat Loss
- Evidence Strength
- 9/10
- Reported Effectiveness
- 7/10
- Summary
- Phase 2 and phase 3 RCTs demonstrate 10.8% (monotherapy) to 22.7% (CagriSema) weight loss. Community confirms weight loss, though attribution is complicated by stacking.
Category
Weight Management
- Evidence Strength
- 9/10
- Reported Effectiveness
- 7/10
- Summary
- Strong trial data across multiple REDEFINE studies. Community positions cagrilintide as an effective plateau-breaker for stalled weight loss protocols.
Category
Nausea & GI Tolerance
- Evidence Strength
- 8/10
- Reported Effectiveness
- 4/10
- Summary
- Well-documented GI side effect profile across all clinical trials. Community widely reports nausea, constipation, and GI distress, particularly during titration. Score reflects negative direction.
Category
Energy Levels
- Evidence Strength
- 4/10
- Reported Effectiveness
- 3/10
- Summary
- Limited clinical characterization of fatigue as a side effect. Community prominently reports fatigue as a dose-limiting adverse effect. Score reflects negative direction.
Category
Digestive Comfort
- Evidence Strength
- 6/10
- Reported Effectiveness
- 4/10
- Summary
- Clinical trials report GI events as the most common adverse effect. Community reports are mixed, with some experiencing worsened and others improved digestive symptoms.
Category
Side Effect Burden
- Evidence Strength
- 8/10
- Reported Effectiveness
- 5/10
- Summary
- Well-characterized in clinical trials as predominantly GI-related and dose-dependent. Community reports wide individual variation in tolerability.
Category
Treatment Adherence
- Evidence Strength
- 7/10
- Reported Effectiveness
- 6/10
- Summary
- Once-weekly dosing supports adherence. Gradual titration protocols are standard. Some community members report needing dose adjustments or breaks.
Category
Cravings & Impulse Control
- Evidence Strength
- 6/10
- Reported Effectiveness
- 7/10
- Summary
- Mechanistic support through amylin's role in reward pathway modulation. Community reports reduced cravings for sweets and altered taste perception.
Category
Emotional Regulation
- Evidence Strength
- 2/10
- Reported Effectiveness
- 4/10
- Summary
- Very limited clinical data on mood effects. One notable community report of acute serotonin-drop symptoms on initial dose, though this appears uncommon.
Category
Mood & Wellbeing
- Evidence Strength
- 3/10
- Reported Effectiveness
- 5/10
- Summary
- Minimal clinical investigation of mood outcomes. Community data is sparse with no clear directional signal.
Category
Gut Health
- Evidence Strength
- 3/10
- Reported Effectiveness
- 5/10
- Summary
- Limited direct evidence. One interesting community report of GERD symptom improvement. Mechanism of gastric emptying delay could theoretically affect gut function in either direction.
Category
Inflammation
- Evidence Strength
- 4/10
- Reported Effectiveness
- 5/10
- Summary
- Indirect evidence through weight loss-mediated metabolic improvement. No direct anti-inflammatory mechanism studies for cagrilintide specifically.
Category
Daily Functioning
- Evidence Strength
- 3/10
- Reported Effectiveness
- 4/10
- Summary
- Not specifically measured in clinical trials. Community reports suggest fatigue can impair daily functioning at higher doses for some individuals.
Categories not scored (insufficient data): Muscle Growth, Physical Performance, Sleep Quality, Focus & Mental Clarity, Memory & Cognition, Anxiety, Stress Tolerance, Motivation & Drive, Emotional Aliveness, Libido, Sexual Function, Joint Health, Pain Management, Recovery & Healing, Skin Health, Hair Health, Heart Health, Blood Pressure, Heart Rate & Palpitations, Hormonal Symptoms, Temperature Regulation, Fluid Retention, Body Image, Immune Function, Bone Health, Longevity & Neuroprotection, Social Connection, Withdrawal Symptoms.
Benefits & Potential Effects
The Basics
The primary benefit of cagrilintide is appetite suppression. People in clinical trials consistently report feeling less hungry, eating smaller meals, and experiencing less mental preoccupation with food. This is not the same as feeling sick and therefore not wanting to eat. The amylin pathway specifically targets the brain's satiety signals, making fullness arrive sooner and last longer. Many community members describe it as "turning down the volume" on hunger rather than eliminating it entirely.
Weight loss follows naturally from sustained appetite suppression. In clinical studies, cagrilintide alone produced meaningful weight reduction, and the combination with semaglutide produced some of the highest weight loss figures seen in clinical research. Community members frequently report that adding cagrilintide to an existing GLP-1 protocol helped break through weight loss plateaus.
Beyond weight and appetite, downstream metabolic improvements have been observed. As body weight decreases, measures of blood sugar control, lipid profiles, and inflammatory markers tend to improve. These are indirect benefits driven primarily by weight loss rather than direct pharmacological effects of cagrilintide on those specific systems.
Some community members report that cagrilintide specifically reduces cravings for sweets and alters the taste perception of certain foods, making previously appealing junk food seem unpalatable. One individual described chocolate tasting "like lip gloss" after adding cagrilintide to their protocol.
The Science
The principal clinical benefits observed in the cagrilintide trial program include:
Appetite and energy intake reduction. Cagrilintide reduces ad libitum energy intake through central amylin receptor activation, with dose-dependent effects observed across the 0.3-4.5 mg weekly dose range [6]. The mechanism is distinct from GLP-1 receptor agonist-mediated appetite suppression, producing additive effects when combined [7].
Body weight reduction. Phase 2: 10.8% mean weight loss at 4.5 mg weekly over 26 weeks [6]. Phase 3 REDEFINE 1: 22.7% mean weight loss with CagriSema at 68 weeks [7]. Phase 3 REDEFINE 2: 15.7% mean weight loss in type 2 diabetes with CagriSema at 68 weeks [11].
Glycemic improvement. In the REDEFINE 2 trial, CagriSema produced significant HbA1c reduction in type 2 diabetes patients, exceeding semaglutide monotherapy [11]. Native amylin contributes to postprandial glucose control through glucagon suppression and gastric emptying delay [4][9].
Lipid profile improvements. Weight loss-mediated improvements in triglycerides, HDL-C, and LDL-C have been observed in clinical trial populations, consistent with the metabolic benefits of sustained caloric deficit [7][11].
Side Effects & Safety Considerations
The Basics
The most common side effects of cagrilintide involve the digestive system. Nausea is the most frequently reported, followed by constipation, diarrhea, and occasionally vomiting. These effects are most pronounced during the first few weeks and when doses are increased, which is why all clinical protocols use a gradual titration schedule. For most people, GI effects diminish over time as the body adjusts, though they can persist at higher doses.
Fatigue is another side effect that community members report prominently, even though it receives less attention in clinical trial publications. Some individuals describe profound exhaustion during the first few weeks, with one person reporting extended sleep periods of ten or more hours. This appears to be dose-dependent and varies significantly between individuals. Starting at lower doses and titrating slowly helps manage this effect.
Injection site reactions, typically mild redness or irritation, are occasionally reported but are generally minor and self-resolving.
An important finding from clinical trials is that anti-cagrilintide antibodies develop in a significant percentage of patients (46-73%), but these antibodies do not appear to reduce the compound's effectiveness. This is a safety observation worth monitoring but has not been clinically concerning in trial data published to date.
Cagrilintide requires careful attention for individuals also taking insulin, as the combination may increase hypoglycemia risk. People with a history of gastroparesis, pancreatitis, or medullary thyroid carcinoma should exercise particular caution and discuss risks with a healthcare provider.
The Science
The safety profile of cagrilintide has been characterized across the REDEFINE clinical trial program:
Gastrointestinal events. The most common adverse effects are GI-related: nausea, vomiting, diarrhea, constipation, and abdominal discomfort. In the REDEFINE 2 trial, GI adverse events were reported by 72.5% of CagriSema patients versus 34.4% of placebo patients. Most events were mild to moderate and transient [11]. Amylin-calcitonin receptor agonists as a class have demonstrated persistent nausea burden, which has been linked to calcitonin receptor activation in the area postrema [12].
Immunogenicity. Anti-cagrilintide antibodies developed in 46-73% of clinical trial participants. Neutralizing antibodies were detected in a subset, but no clinically meaningful impact on efficacy or safety was observed [6][7].
Hypoglycemia risk. When combined with insulin or insulin secretagogues, the risk of hypoglycemia is elevated due to cagrilintide's glucagon-suppressive effects. Clinical protocols recommend monitoring and potential insulin dose adjustment [11].
Precautions and contraindications. Rapid weight loss may increase gallbladder symptom risk. Caution is warranted in individuals with gastroparesis or a history of pancreatitis. Use during pregnancy and breastfeeding is contraindicated [6].
Fibril formation concern. Community discussion has raised awareness of amylin's tendency to form fibrils (misfolded protein aggregates). Native amylin is amyloidogenic and contributes to pancreatic islet amyloid deposits in type 2 diabetes. The structural modifications in cagrilintide were designed to reduce, though not eliminate, this propensity. The clinical significance of this concern during therapeutic use is being monitored in ongoing trials [2].
The side effects and contraindications above give you a map of what to watch for. Doserly turns that map into a daily practice. Log the specific biomarkers and symptoms associated with this compound's known risk profile, and the app builds a timeline of how your body is responding across your cycle.
Trending in the wrong direction on a key marker? Noticing a pattern that started two weeks into your protocol? Doserly connects the dots between your protocol timeline and your logged data, making it easier to spot emerging issues early and have informed, data-backed conversations with your healthcare provider about what's working and what needs attention.
Connect protocol changes to labs and health markers.
Doserly can keep lab results, biomarkers, symptoms, and dose history close together so follow-up conversations have better context.
Insights
Labs and trends

Doserly organizes data; it does not diagnose or interpret labs for you.
Dosing Protocols
The Basics
Cagrilintide dosing follows a gradual escalation approach. Starting low and increasing slowly is essential because the compound's long half-life (about a week) means each dose stacks on top of the previous one. Effects and side effects can intensify over the first several weeks even without a dose increase.
Sources report several different dosing approaches, and there is no single consensus protocol. This variation reflects both the compound's investigational status and the different contexts in which it is used (monotherapy versus combination with GLP-1 compounds).
Commonly reported dosing approaches from available sources:
Monotherapy (from clinical trial design): Starting at 0.6 mg weekly, doubling every two weeks (0.6, 1.2, 2.4 mg), with a maintenance target of up to 4.5 mg weekly. This is the most aggressive titration schedule and reflects the phase 2 trial design [6].
Combination use (CagriSema protocol): Starting at 0.25 mg weekly, escalating gradually over 16 weeks to a target of 2.4 mg weekly. This slower titration is co-escalated with semaglutide [7].
Community-reported stacking doses: Many community members using cagrilintide alongside tirzepatide or retatrutide report effective appetite suppression at doses of 0.125-0.5 mg weekly, substantially lower than clinical trial monotherapy doses. Individual response varies widely; some report no effect below 1.5-2.0 mg while others find 0.125 mg overwhelmingly strong.
The steep dose-response curve and wide individual variation are consistent themes in both clinical data and community reports. Starting conservatively and adjusting based on response is the approach most commonly recommended across sources.
The Science
Dosing protocols from the cagrilintide clinical development program:
Phase 2 monotherapy (Lau et al., 2021): Doses of 0.3, 0.6, 1.2, 2.4, and 4.5 mg administered weekly for 26 weeks. Dose-dependent weight loss was observed, with 4.5 mg producing the greatest mean reduction (-10.8% vs -3.0% placebo). The titration schedule escalated doses every two weeks to the target maintenance dose [6].
Phase 3 CagriSema (REDEFINE program): Cagrilintide 2.4 mg combined with semaglutide 2.4 mg, both administered once weekly. Dose escalation for cagrilintide followed: 0.25 mg (weeks 1-4), 0.5 mg (weeks 5-8), 1.0 mg (weeks 9-12), 1.7 mg (weeks 13-16), 2.4 mg (week 17 onward). This co-escalation mirrors the semaglutide titration to minimize GI adverse events [7][11].
Clinical data demonstrate a clear dose-response relationship across the studied range. Higher doses produce greater weight loss but also increase the frequency and severity of gastrointestinal adverse events, supporting the rationale for gradual titration [6].
Consistency is the difference between a protocol that delivers results and one that wastes time and money. Doserly was built for exactly this: keeping you on track with the precision your protocol demands.
The built-in calculators handle the math you shouldn't be doing in your head. The reconstitution calculator tells you exactly how much bacteriostatic water to add for your target concentration. The dose calculator converts between units, milligrams, and syringe markings so you draw the right amount every time. The injection site heat map tracks where you've administered and when, helping you rotate sites systematically to reduce tissue damage, scarring, and absorption inconsistencies from overusing the same area. Pair that with smart reminders tuned to your protocol's timing requirements, and you build the kind of daily consistency that separates optimized protocols from haphazard ones.
Track injection timing, draw notes, and site rotation.
Doserly helps keep syringe-related notes, injection site history, reminders, and reconstitution context together for easier review.
Injection log
Site rotation
Injection logs support record-keeping; follow clinician instructions for administration.
What to Expect
The following timeline reflects patterns observed in clinical trials and community reports. Individual experiences vary significantly based on dose, concurrent medications, individual biology, and lifestyle factors.
Weeks 1-2: Adaptation period. The initial dose is typically well below the target, so many people feel little or no effect during this phase. Some individuals report mild nausea or GI adjustment. A subset of sensitive responders may notice early appetite changes. The compound is beginning to accumulate but has not yet reached steady state.
Weeks 3-4: Early effects emerge. As the compound accumulates and doses are escalated, appetite suppression typically becomes noticeable. Some people report the onset being subtle; others describe it as sudden and pronounced. GI side effects (nausea, constipation) may appear or intensify. Fatigue is commonly reported during this period, particularly in those using cagrilintide alongside other GLP-1 compounds.
Weeks 5-8: Appetite suppression and early weight loss. Appetite reduction is usually well-established by this point. Early weight loss of 2-5% from baseline is commonly reported. Food noise and cravings may diminish. Some community members report altered taste perception, particularly for sweets. Side effects from earlier dose escalations typically begin to stabilize.
Weeks 9-16: Accelerated weight loss. Weight loss continues to accumulate as the compound reaches higher doses and the cumulative caloric deficit deepens. In clinical trials, the rate of weight loss is most pronounced during this middle period. Some individuals plateau temporarily before further dose escalation produces additional progress.
Weeks 17-26: Approaching peak efficacy. In monotherapy trials, the maximum studied dose (4.5 mg) produced 10.8% weight loss by week 26. The rate of weight loss typically decelerates as the body adapts. Metabolic markers (blood glucose, lipids, inflammation markers) show improvement driven by the sustained weight reduction.
Weeks 26+: Maintenance and sustained effects. Long-term data from the 68-week REDEFINE trials show continued weight loss and metabolic improvement through week 68 with the CagriSema combination. The question of what happens after discontinuation is clinically important; GLP-1 class data suggests significant weight regain is common when treatment is stopped.
The week-by-week expectations above are drawn from research and community reports, but your experience will be uniquely yours. Doserly's biomarker tracking transforms those general timelines into personal data points you can actually see and measure.
Log the specific markers relevant to this compound, whether that's pain levels, energy, sleep quality, body composition, recovery time, or mood, and watch your own trend lines emerge over weeks and months. Did your key markers start shifting in week three, like the research suggests? Is your experience tracking with what the community reports, or diverging? Over time, this creates something more valuable than any guide: an evidence-based picture of how your body responds to this specific compound, at your specific dose, within your specific health context.
See where a dose, cycle, or change fits in time.
Doserly gives each protocol a timeline so dose changes, pauses, restarts, and observations are easier to compare later.
Timeline
Cycle history

Timeline tracking helps with recall; it is not a treatment recommendation.
Interaction Compatibility
Synergistic combinations ("Good With"):
- Semaglutide - The CagriSema combination is the most clinically studied pairing, producing additive weight loss effects through complementary amylin + GLP-1 receptor activation [7][11].
- Tirzepatide - Community members widely report stacking cagrilintide with tirzepatide to enhance appetite suppression when tirz alone produces insufficient satiety. Not clinically studied as a formal combination.
- Retatrutide - Frequently discussed as a complement to retatrutide's triple agonism (GLP-1/GIP/glucagon), adding a fourth mechanism (amylin) for enhanced appetite control. Community reports are generally positive.
- Tesofensine - Listed as a pairing option for weight management protocols in community educator content.
- 5-Amino-1MQ - Mentioned as a complementary metabolic compound in community protocol recommendations.
- MOTS-C - Suggested as a metabolic support compound to pair with appetite-suppressing agents.
- AOD-9604 - Listed as a complementary compound for fat loss protocols.
- NAD+ - Recommended to support energy levels and mitochondrial function during caloric deficit from appetite suppression.
- SS-31 - Mentioned in community stacking recommendations for metabolic support.
- SLU-PP-332 - Suggested as a metabolic pairing compound.
Compounds requiring caution ("Not Good With"):
- Insulin and insulin secretagogues - Increased hypoglycemia risk due to cagrilintide's glucagon-suppressive effects. Dose adjustments and close monitoring are recommended [11].
- Other amylin analogues (pramlintide) - Redundant mechanism; co-administration would provide no benefit and could increase adverse effects.
Administration Guide
Materials typically required:
- Cagrilintide lyophilized powder vial (common sizes: 5 mg, 10 mg)
- Bacteriostatic water or 0.6% acetic acid solution for reconstitution
- Sterile syringes (U-100 insulin syringes for lower doses; 3 mL syringes for maintenance doses exceeding 1 mL volume)
- Alcohol swabs
- Sharps disposal container
Reconstitution solution considerations: Standard bacteriostatic water is widely used and acceptable for short-term storage (under 30 days). Some sources note that cagrilintide has optimal stability at an acidic pH of approximately 3.5-4.5, and that using 0.6% acetic acid as the reconstitution medium may reduce fibril formation risk during extended storage. This reflects the amylin family's known tendency toward aggregation at neutral pH.
Timing considerations: Cagrilintide is administered once weekly on the same day each week. There is no strict requirement for fasting or specific timing relative to meals. Some community members prefer morning administration to allow any initial GI effects to manifest during waking hours. Consistency in the day and approximate time of administration supports stable drug levels given the compound's long half-life.
Post-administration considerations: During the first one to two weeks at each new dose level, smaller meals, slower eating, and attention to hydration are commonly recommended to manage GI adjustment. Electrolyte supplementation and adequate fiber intake may help mitigate constipation. Monitor for signs of excessive appetite suppression (inability to meet minimum caloric and protein needs), as this can indicate the dose is too high.
Supplies & Planning
Cagrilintide is typically available in lyophilized powder form in vial sizes of 5 mg and 10 mg. The following supplies are generally associated with cagrilintide protocols:
- Peptide vials: Available in 5 mg and 10 mg sizes. The number of vials needed depends on the target dose and cycle duration, which should be determined in consultation with a healthcare provider.
- Reconstitution solution: Bacteriostatic water (standard) or 0.6% acetic acid (for improved stability). Common reconstitution volumes are 2.0 mL (5 mg vial, yielding 2.5 mg/mL) or 3.0 mL (10 mg vial, yielding approximately 3.33 mg/mL).
- Syringes: U-100 insulin syringes provide precision for smaller doses during titration. For maintenance doses that exceed 100 units (1.0 mL), 3 mL syringes with 25-27G subcutaneous needles are needed.
- Alcohol swabs: Two per administration (one for the vial stopper, one for the injection site).
- Sharps container: For safe disposal of used syringes and needles.
- Storage supplies: Refrigerator space for reconstituted vials; freezer space for unreconstituted lyophilized vials.
Consult the Doserly reconstitution calculator and a healthcare provider for specific quantity planning based on your individual protocol.
Storage & Handling
Proper storage is critical for maintaining cagrilintide's potency and stability.
Lyophilized (unreconstituted) powder:
- Store at -20 C (-4 F) in a dry location protected from light
- Allow vials to reach room temperature before reconstitution to minimize condensation
- Minimize freeze-thaw cycles; avoid repeated temperature fluctuations
Reconstituted solution:
- Refrigerate at 2-8 C (35.6-46.4 F) immediately after reconstitution
- Protect from light
- Use within 30 days of reconstitution
- Discard if the solution appears cloudy, discolored, or contains visible particulate matter
pH stability note: Cagrilintide, like other amylin-family peptides, is most stable at an acidic pH of approximately 3.5-4.5. At neutral pH, the compound has an increased tendency to form fibrils (misfolded protein aggregates). When using standard bacteriostatic water (typically pH 4.5-7.0), reconstituted solutions should be used promptly and stored according to the guidelines above. Using 0.6% acetic acid as the reconstitution solution provides a more optimal pH environment for longer-term storage.
Lifestyle Factors
Maximizing the benefits of cagrilintide requires attention to several lifestyle factors that work in concert with the compound's appetite-suppressing mechanism.
Protein intake. Maintaining adequate protein consumption is particularly important during significant weight loss. High protein intake (commonly cited as 1.0-1.6 g per kilogram of body weight daily) supports muscle preservation and helps prevent the lean mass loss that can accompany rapid weight reduction. Because cagrilintide can substantially reduce appetite, many people find it challenging to meet protein targets and may need to prioritize protein-dense foods or supplementation.
Resistance training. Consistent strength training is the primary intervention for preserving muscle mass during caloric deficit. Community educators and clinical guidelines both emphasize that weight loss without resistance exercise disproportionately affects lean tissue.
Hydration and electrolytes. GI side effects (constipation, diarrhea, nausea) are exacerbated by dehydration. Adequate water intake and electrolyte supplementation, particularly sodium, potassium, and magnesium, can help manage these effects. Fiber intake should also be gradually increased to support digestive regularity.
Meal strategy. During dose escalation, eating slower, choosing smaller meals, and avoiding high-fat or rich foods can help manage nausea and digestive discomfort. Some community members find that front-loading protein early in the day, when appetite may be at its lowest, helps meet nutritional targets.
Sleep. Adequate sleep (seven to nine hours) supports both metabolic health and the body's adaptation to caloric deficit. Poor sleep is associated with increased appetite and reduced adherence to weight management protocols.
Bloodwork monitoring. Periodic bloodwork is recommended to track metabolic markers including fasting glucose, HbA1c, fasting insulin, lipid panel (triglycerides, HDL-C, LDL-C), liver enzymes (ALT, AST, GGT), renal markers (creatinine/eGFR), electrolytes, and optionally hs-CRP for inflammation monitoring.
Regulatory Status & Research Classification
United States (FDA): Cagrilintide is investigational. It is not approved for any indication. Novo Nordisk filed a New Drug Application (NDA) for CagriSema (cagrilintide 2.4 mg + semaglutide 2.4 mg combination) in December 2025. An FDA decision is anticipated by late 2026. Standalone cagrilintide does not have a separate NDA. Multiple active clinical trials are registered on ClinicalTrials.gov, including the REDEFINE program (NCT05394519 and related registrations) and the RENEW program for cagrilintide monotherapy.
European Union (EMA): Regulatory submissions for CagriSema are anticipated but no marketing authorization has been filed as of early 2026.
Canada (Health Canada): No submission filed as of early 2026.
United Kingdom (MHRA): No approval or submission reported as of early 2026.
Australia (TGA): No approval or submission reported as of early 2026.
WADA status: Athletes should verify the status of cagrilintide with their specific federation before use. Amylin analogues and related peptide hormones may be subject to anti-doping restrictions.
Active clinical trials: The REDEFINE program (phases 3 and 3a) includes multiple trials evaluating CagriSema for obesity with and without type 2 diabetes. The REIMAGINE program is evaluating CagriSema for additional indications. Check ClinicalTrials.gov for current trial status and enrollment information.
Regulatory status changes frequently. Always verify the current legal status of any compound in your specific country or jurisdiction before making any decisions.
FAQ
What is cagrilintide and how does it differ from semaglutide or tirzepatide?
Cagrilintide is a long-acting amylin analogue that targets amylin and calcitonin receptors, a completely different pathway from GLP-1 receptor agonists like semaglutide (Ozempic/Wegovy) and GLP-1/GIP dual agonists like tirzepatide (Mounjaro/Zepbound). While GLP-1 compounds and cagrilintide both reduce appetite, they do so through separate brain circuits, which is why combining them (as in CagriSema) produces additive effects.
How much weight loss can be expected with cagrilintide?
Based on available clinical trial data, cagrilintide monotherapy at the highest studied dose (4.5 mg weekly) produced approximately 10.8% body weight loss over 26 weeks. The combination with semaglutide (CagriSema) produced approximately 22.7% weight loss at 68 weeks in the REDEFINE 1 trial. Individual responses vary significantly, and results depend on dose, concurrent treatments, diet, exercise, and individual biology. Consulting a healthcare provider is recommended before starting any weight management protocol.
Can cagrilintide be taken with tirzepatide or retatrutide?
Community members widely report using cagrilintide alongside tirzepatide or retatrutide, though these specific combinations have not been studied in clinical trials. The rationale is that cagrilintide's amylin receptor activation complements the GLP-1/GIP pathways targeted by those compounds. Individuals considering any combination should discuss the approach with a healthcare provider, particularly regarding dose adjustments and monitoring.
What are the most common side effects?
Based on clinical trial data and community reports, the most frequently reported side effects are gastrointestinal: nausea, constipation, diarrhea, and abdominal discomfort. Fatigue is also prominently reported by community members, particularly during the first several weeks. Most GI effects are dose-dependent and tend to diminish with time and gradual titration. A healthcare provider can help develop strategies to manage these effects.
How should cagrilintide be reconstituted and stored?
Cagrilintide is typically reconstituted with bacteriostatic water or 0.6% acetic acid solution. The compound has optimal stability at acidic pH (3.5-4.5). Reconstituted solution should be stored refrigerated at 2-8 C and used within 30 days. Unreconstituted lyophilized powder should be stored at -20 C. Consult a healthcare provider and use the Doserly reconstitution calculator for specific preparation guidance.
Is cagrilintide FDA-approved?
As of early 2026, cagrilintide is not FDA-approved. Novo Nordisk filed a New Drug Application for CagriSema (the combination product with semaglutide) in December 2025, with a decision expected by late 2026. Cagrilintide is classified as an investigational compound currently in phase 3 clinical trials.
Why do some people report no effect from cagrilintide?
Community reports indicate significant individual variation in response to cagrilintide. Some people report no appetite suppression even at doses of 1.5-2.0 mg, while others experience overwhelming effects at 0.125 mg. This variation may reflect differences in receptor sensitivity, concurrent medications, individual metabolism, and the quality and formulation of research-grade compounds. If no effect is observed after adequate titration, consulting a healthcare provider about alternative approaches is advisable.
Sources & References
[1] J Med Chem (2021). Development of cagrilintide: a long-acting amylin analogue. Journal of Medicinal Chemistry. Details the molecular design, structural modifications, and pharmacological characterization of cagrilintide.
[2] Enebo LB, et al. (2021). Safety, tolerability, pharmacokinetics, and pharmacodynamics of concomitant administration of multiple doses of cagrilintide with semaglutide 2.4 mg for weight management: a randomised, controlled, phase 1b trial. The Lancet. Phase 1b trial establishing PK/PD and safety of the cagrilintide-semaglutide combination. https://doi.org/10.1016/S0140-6736(21)00845-X
[3] Brain Res Rev (2005). Pancreatic amylin as a centrally acting satiating hormone. Reviews the central mechanisms of amylin-mediated satiety signaling.
[4] PMC (2006). Pancreatic signals controlling food intake: insulin, glucagon, and amylin. Comprehensive review of pancreatic hormone crosstalk in appetite regulation.
[5] PMC (2016). Amylin-mediated control of glycemia, energy balance, and cognition. Review of amylin's role across metabolic and cognitive functions.
[6] Lau DCW, et al. (2021). Once-weekly cagrilintide for weight management in people with overweight and obesity: a multicentre, randomised, double-blind, placebo-controlled and active-controlled, dose-finding phase 2 trial. The Lancet. 398(10317):2160-2172. The pivotal phase 2 dose-finding trial establishing dose-dependent weight loss with cagrilintide. https://doi.org/10.1016/S0140-6736(21)01751-7
[7] N Engl J Med (2025). REDEFINE 1: Coadministered cagrilintide and semaglutide in adults with overweight or obesity. Phase 3 trial demonstrating 22.7% weight loss with CagriSema at 68 weeks.
[8] Int J Mol Sci (2024). Amylin, another important neuroendocrine hormone for treatment of diabesity. Review of amylin's therapeutic potential in metabolic disease.
[9] PMC (2022). Mediators of amylin action in metabolic control. Review of downstream signaling pathways of amylin receptor activation.
[10] PMC (2024). Clinical pharmacokinetics of semaglutide: systematic review. Includes cagrilintide pharmacokinetic data from the co-administration studies.
[11] N Engl J Med (2025). REDEFINE 2: Cagrilintide-semaglutide in adults with overweight/obesity and type 2 diabetes. Phase 3 trial in type 2 diabetes population demonstrating 15.7% weight loss with CagriSema.
[12] Novo Nordisk press release (2026). REDEFINE 4 topline results: CagriSema versus tirzepatide head-to-head comparison. Reports tirzepatide superiority with 25.5% vs 23% weight loss at 84 weeks.
[13] PMC (2024). Efficacy and safety of cagrilintide and CagriSema: systematic review and meta-analysis. Comprehensive meta-analysis of cagrilintide clinical data across trials.
Related Peptide Guides
- Semaglutide - GLP-1 receptor agonist; the combination partner in CagriSema
- Tirzepatide - GLP-1/GIP dual agonist; head-to-head comparator in REDEFINE 4; commonly stacked with cagrilintide in community protocols
- Retatrutide - GLP-1/GIP/glucagon triple agonist; frequently stacked with cagrilintide for enhanced appetite suppression
- Cagri/Sema - The pre-mixed combination product page
- AOD-9604 - Complementary fat loss peptide mentioned in stacking protocols
- MOTS-C - Metabolic support compound paired with appetite suppressants
- 5-Amino-1MQ - Complementary metabolic compound
- Tesofensine - Weight management compound mentioned in community protocols
- NAD+ - Energy support compound recommended during caloric deficit
- Orforglipron - Oral non-peptide GLP-1 agonist; next-generation competitor in the metabolic space
- Mazdutide - GLP-1/glucagon dual agonist; emerging competitor
- Survodutide - GLP-1/glucagon dual agonist; another pipeline competitor
- SLU-PP-332 - Metabolic pairing compound
- SS-31 - Mitochondrial support compound mentioned in stacking recommendations
Need the reconstitution math for Cagrilintide: Complete Research Guide?
Open the calculator with Cagrilintide: Complete Research Guide prefilled to estimate concentration, draw volume, and related measurement math from the reconstitution details you already have.