Orforglipron: Complete Research Guide
On this page
Quick Reference Card
Attribute
Also Known As
- Detail
- LY3502970, orforglipron (or-for-GLIP-ron)
Attribute
Administration
- Detail
- Oral (once-daily pill); no food or water restrictions
Attribute
Research Status
- Detail
- Investigational. NDA under FDA priority review for obesity (decision expected Q2 2026). Not a peptide. Non-peptide small molecule GLP-1 receptor agonist.
Attribute
Typical Dose Range
- Detail
- 3 mg, 6 mg, 12 mg, or 36 mg once daily (clinical trial doses); dose escalation from 1 mg starting dose
Attribute
Half-Life
- Detail
- Approximately 24 hours (elimination half-life 25-68 hours)
Attribute
Cycle Length
- Detail
- Continuous daily use (72 weeks in Phase 3 trials); intended for long-term treatment
Attribute
Storage
- Detail
- Room temperature; no refrigeration required
Overview / What Is Orforglipron?
The Basics
Orforglipron is an investigational once-daily pill being developed by Eli Lilly for weight management and type 2 diabetes. It belongs to the GLP-1 receptor agonist drug class, the same family as semaglutide (Ozempic/Wegovy) and tirzepatide (Mounjaro/Zepbound). But there is a critical distinction: orforglipron is not a peptide. It is a small molecule.
That difference matters because peptide-based GLP-1 drugs like semaglutide are proteins that get destroyed by stomach acid. Getting them into a pill requires complex engineering and strict fasting protocols. Oral semaglutide (Rybelsus/Wegovy pill) absorbs at roughly 1%, meaning 99% of what you swallow never reaches your bloodstream. Orforglipron sidesteps this problem entirely. As a small molecule, it survives digestion naturally and absorbs at approximately 79%, roughly 80 times better than oral semaglutide. This means it can be taken at any time, with or without food, without water restrictions.
Clinical trials involving over 3,000 participants show weight loss of approximately 10-12% at the highest dose (36 mg) over 72 weeks, with improvements in blood sugar control, blood pressure, and cholesterol markers. These results are somewhat lower than injectable GLP-1 drugs like Wegovy (14.9%) or Zepbound (20-22%), but the trade-off is convenience: a daily pill with no injections, no refrigeration, and no special administration requirements.
Orforglipron was originally discovered by Chugai Pharmaceutical and licensed to Eli Lilly in 2018. Lilly submitted a New Drug Application to the FDA in late 2025 and received priority review designation. A decision is expected in mid-2026.
The Science
Orforglipron (LY3502970) is a synthetic, orally bioavailable nonpeptide agonist of the glucagon-like peptide-1 receptor (GLP-1R), a class B (secretin family) G protein-coupled receptor (GPCR) [1]. Unlike peptide-based GLP-1 RAs such as semaglutide and liraglutide, orforglipron is a small molecule built around a rigid polycyclic heteroaromatic scaffold that confers chemical stability in the gastrointestinal tract without the need for absorption enhancers or formulation engineering [2].
Cryo-electron microscopy (cryo-EM) studies demonstrate that orforglipron binds within the upper helical bundle of the GLP-1R transmembrane domain, partially overlapping with the native GLP-1 binding site but engaging distinct residues [3]. Functionally, orforglipron acts as a partial agonist with biased signaling, preferentially activating cAMP pathways through Gs protein coupling over beta-arrestin recruitment [3]. This signaling bias may contribute to its distinct efficacy and tolerability profile relative to peptide-based full agonists.
Phase 3 clinical programs (ATTAIN for obesity, ACHIEVE for type 2 diabetes) have demonstrated significant reductions in body weight (11.2% at 36 mg over 72 weeks in ATTAIN-1, N=3,127), HbA1c (1.6-2.2% reduction), and cardiovascular risk biomarkers including systolic blood pressure, triglycerides, and non-HDL cholesterol [4][5][6].
Molecular Identity
Property
Drug Class
- Detail
- Non-peptide small molecule GLP-1 receptor agonist
Property
Development Code
- Detail
- LY3502970
Property
Developer
- Detail
- Eli Lilly (licensed from Chugai Pharmaceutical, 2018)
Property
Molecular Type
- Detail
- Synthetic small molecule (not a peptide)
Property
Target
- Detail
- GLP-1 receptor (GLP-1R), class B GPCR
Property
Oral Bioavailability
- Detail
- 79.1% (+/- 16.8%)
Property
Elimination Half-Life
- Detail
- 25-68 hours
Property
Binding Site
- Detail
- Upper helical bundle of GLP-1R transmembrane domain
Note: As a proprietary small molecule, the full molecular formula and structure of orforglipron have not been fully disclosed publicly. CAS number and PubChem ID are not widely available in public databases as of March 2026.
Mechanism of Action
The Basics
Orforglipron works by mimicking a hormone your gut naturally produces after you eat, called GLP-1 (glucagon-like peptide-1). Your body uses this hormone for three important jobs:
First, it tells your pancreas to release insulin when blood sugar rises after a meal. This is glucose-dependent, meaning it only works when blood sugar is actually elevated, which reduces the risk of dangerously low blood sugar.
Second, it slows down how quickly food leaves your stomach (a process called gastric emptying). When food stays in your stomach longer, you feel full for longer, which naturally leads to eating less at your next meal.
Third, it signals your brain's appetite center (the hypothalamus) that you have had enough to eat. This reduces the mental drive to seek food, sometimes described as quieting "food noise."
Natural GLP-1 breaks down in your body within about two minutes. Traditional GLP-1 drugs are modified peptides designed to last much longer. Orforglipron takes a completely different approach: instead of modifying the natural hormone, it is a synthetic molecule designed to fit into the same receptor lock but built from scratch as a conventional drug molecule. This is why it can survive stomach acid and absorb like a regular pill.
The Science
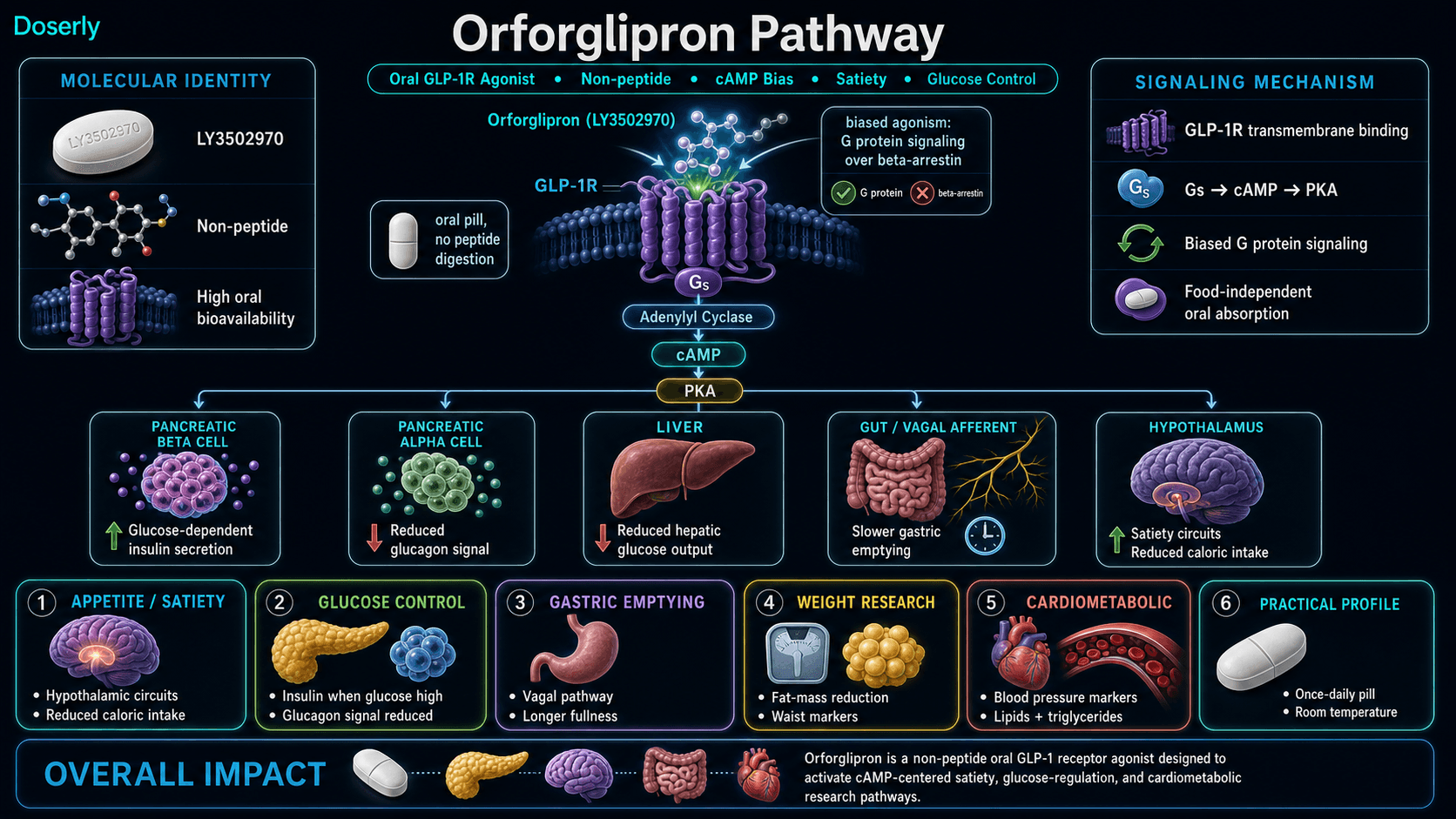
Orforglipron activates the GLP-1 receptor (GLP-1R) on pancreatic beta cells, leading to Gs-protein-mediated activation of adenylyl cyclase, elevation of intracellular cyclic AMP (cAMP), and downstream protein kinase A (PKA) activation [1]. This cascade enhances glucose-dependent insulin secretion while simultaneously suppressing glucagon release from alpha cells, thereby reducing hepatic glucose output [2].
Competition binding experiments using either [125I]GLP-1(7-36)NH2 or [3H]orforglipron demonstrate that orforglipron occupies a partially overlapping but distinct binding pocket compared to native GLP-1 [3]. The molecule exhibits biased agonism at the GLP-1R: it preferentially activates G protein signaling pathways over beta-arrestin recruitment [3]. This pharmacological distinction may account for differences in receptor internalization kinetics and downstream signal duration compared to peptide agonists.
Central nervous system effects include activation of hypothalamic satiety circuits, contributing to appetite suppression and reduced caloric intake. Peripheral effects include delayed gastric emptying through vagal afferent pathways, further contributing to post-prandial satiety [1][2].
Pathway Visualization Image
Pharmacokinetics
The Basics
One of orforglipron's most notable characteristics is how well it absorbs from the gut. While oral semaglutide (the Wegovy pill) absorbs at roughly 1%, orforglipron absorbs at approximately 79%. This 80-fold difference is the core reason orforglipron can be taken without fasting protocols, food timing restrictions, or water volume limits.
After you take a pill, orforglipron reaches its peak blood levels in about 3-5 hours. Its half-life (how long it takes for half the drug to clear your system) is approximately 24 hours, which supports once-daily dosing. The elimination half-life ranges from 25 to 68 hours depending on the study and individual variation, meaning the drug builds up to steady-state levels over several days of daily dosing.
These pharmacokinetic properties also mean orforglipron does not require refrigeration or cold-chain storage. It is stable at room temperature, which is a practical advantage for shipping, travel, and daily use compared to injectable GLP-1 drugs that need refrigeration.
The Science
Phase 1 pharmacokinetic studies in healthy volunteers demonstrated dose-proportional exposure across the clinical dose range [7]. Key parameters:
- Tmax: 3-5 hours post-dose
- Elimination half-life: 25-68 hours (mean approximately 24 hours)
- Oral bioavailability: 79.1% +/- 16.8%
- Food effect: None. Absorption is not affected by food intake, eliminating the need for fasting protocols [7]
- Steady-state: Achieved within approximately 5-7 days of daily dosing
The high oral bioavailability reflects orforglipron's resistance to gastrointestinal proteolysis and acid-mediated degradation, properties inherent to its non-peptide small-molecule structure. Unlike oral semaglutide, which requires the SNAC absorption enhancer (sodium N-[8-(2-hydroxybenzoyl)amino]caprylate) to achieve even 1% bioavailability, orforglipron absorbs through conventional intestinal absorption pathways [2][7].
Research & Clinical Evidence
Obesity (ATTAIN Program)
The Basics
The largest study of orforglipron for weight loss (ATTAIN-1) enrolled 3,127 adults with obesity but without diabetes. Participants took orforglipron at three different doses (6 mg, 12 mg, or 36 mg) or a placebo daily for 72 weeks. The highest dose group lost an average of 11.2% of their body weight (approximately 27.3 pounds), compared to 2.1% with placebo. More than half (54.6%) of those on the highest dose lost at least 10% of their body weight [4].
An earlier Phase 2 study tested a higher dose (45 mg) and found 14.7% weight loss at just 36 weeks, with weight loss still continuing at the end of the study period. However, the 45 mg dose was not included in Phase 3 trials, which capped at 36 mg [8].
Body composition data from Phase 2 showed that approximately 75% of weight lost was fat mass and 25% was lean mass, a ratio comparable to or slightly better than that seen with other GLP-1 drugs [9].
The Science
ATTAIN-1 (Phase 3, NCT05869903): A multinational, randomized, double-blind, placebo-controlled trial in 3,127 adults with obesity (BMI >=30 or >=27 with comorbidity) without diabetes. At 72 weeks, mean percent change in body weight from baseline was -7.5% (6 mg), -8.4% (12 mg), and -11.2% (36 mg) vs -2.1% (placebo), all P<0.001. The proportion achieving >=10% weight loss was 32.2%, 39.2%, and 54.6% for the three doses vs 12.9% for placebo [4].
ATTAIN-2 (Phase 3, NCT05872620): Adults with obesity and type 2 diabetes (N not fully disclosed). The 36 mg dose produced 10.5% weight loss (22.9 lbs) at 72 weeks with HbA1c reduction of 1.3-1.8% across doses [5].
ATTAIN-MAINTAIN (Phase 3): First-of-its-kind trial evaluating switch from injectable to oral GLP-1. Patients switching from semaglutide (Wegovy) to orforglipron 36 mg maintained weight with only 0.9 kg regain at 52 weeks. Patients switching from tirzepatide (Zepbound) showed 5.0 kg regain, suggesting orforglipron may be more effective as a maintenance option for single-agonist GLP-1 users than for dual-agonist users [10].
Phase 2 (GZGI, NCT05051579): 272 adults with obesity, 36 weeks. Weight loss ranged from 9.4% to 14.7% across doses (12-45 mg) vs 2.3% placebo, with weight loss trajectory not yet plateaued at study end [8].
Type 2 Diabetes (ACHIEVE Program)
The Basics
For people with type 2 diabetes, orforglipron has shown strong blood sugar control results. In the ACHIEVE-3 head-to-head trial, orforglipron 36 mg reduced HbA1c (a measure of average blood sugar over three months) by 2.2 percentage points, compared to 1.4 points for oral semaglutide 14 mg. In that same trial, 85% of patients on orforglipron 36 mg achieved blood sugar levels below the standard diabetes threshold (HbA1c below 7%), compared to 66% on oral semaglutide [6].
Weight loss in the diabetes trials was also meaningful: 9.2% (19.7 lbs) with orforglipron 36 mg versus 5.3% (11.0 lbs) with oral semaglutide 14 mg in ACHIEVE-3 [6].
The Science
ACHIEVE-1 (Phase 3, NCT05971940): 559 adults with T2D. At 40 weeks, HbA1c reduction was 1.3-1.6 percentage points (3 mg, 12 mg, 36 mg) vs 0.1 placebo. Over 65% of 36 mg patients achieved HbA1c <=6.5%. Weight loss: 4.7-7.9% vs 1.6% placebo, with no plateau observed at study end [5].
ACHIEVE-3 (Phase 3, NCT06045221): 1,698 adults with T2D inadequately controlled on metformin. 52-week, head-to-head comparison of orforglipron (12 mg, 36 mg) vs oral semaglutide (7 mg, 14 mg). Orforglipron demonstrated noninferiority and superiority to oral semaglutide for mean change in HbA1c. Key results: orforglipron 36 mg reduced HbA1c by 1.91% (treatment regimen estimand) vs 1.47% for semaglutide 14 mg. Weight loss: 9.2% vs 5.3%. Published in The Lancet, February 2026 [6].
Phase 2 (NCT05048719): 383 adults with T2D on metformin, 26 weeks. HbA1c reduction up to 2.1% vs 0.43% placebo and 1.10% dulaglutide. Weight loss: 10.1 kg vs 2.2 kg placebo vs 3.9 kg dulaglutide [11].
Cardiovascular Biomarkers
The Basics
Across clinical trials, orforglipron consistently improved several markers of cardiovascular health, including reductions in blood pressure (5-6 mmHg systolic), triglycerides, and cholesterol levels. However, no dedicated cardiovascular outcomes trial has been completed for orforglipron specifically. The strongest evidence for GLP-1 drugs reducing heart attacks and strokes comes from the SELECT trial with injectable semaglutide, which showed a 20% reduction in major cardiovascular events. Whether orforglipron provides similar cardiovascular protection remains to be determined.
The Science
Cardiovascular risk biomarker improvements observed across the ATTAIN and ACHIEVE programs include reductions in systolic blood pressure (approximately 5-6 mmHg), triglycerides, non-HDL cholesterol, VLDL cholesterol, and total cholesterol [4][5][6]. These improvements appeared as early as week 4 and were sustained through end-of-study [6]. A mean increase in pulse rate was noted in orforglipron-treated groups relative to controls, consistent with the GLP-1 RA class effect [6]. Dedicated cardiovascular outcomes trials (CVOTs) for orforglipron have not been completed as of March 2026.
Biomarker Evidence Matrix
Category
Fat Loss
- Evidence Strength
- 9/10
- Reported Effectiveness
- 7/10
- Summary
- Multiple Phase 3 RCTs demonstrate 10-12% body weight reduction at 36 mg over 72 weeks; Phase 2 showed 14.7% at 45 mg. Body composition: ~75% fat, ~25% lean mass loss.
Category
Weight Management
- Evidence Strength
- 8/10
- Reported Effectiveness
- 7/10
- Summary
- ATTAIN-MAINTAIN trial demonstrates weight maintenance after switching from injectable GLP-1s. Continuous daily use intended for long-term management.
Category
Appetite & Satiety
- Evidence Strength
- 7/10
- Reported Effectiveness
- 6/10
- Summary
- GLP-1 mechanism inherently reduces appetite via hypothalamic signaling and gastric emptying delay. Clinical trial data confirms caloric intake reduction. No direct community user reports.
Category
Nausea & GI Tolerance
- Evidence Strength
- 8/10
- Reported Effectiveness
- 5/10
- Summary
- Detailed side effect data from 3,000+ patient Phase 3 trials. GI events in ~50% of users, roughly half the burden of oral semaglutide.
Category
Side Effect Burden
- Evidence Strength
- 8/10
- Reported Effectiveness
- 6/10
- Summary
- Comprehensive safety data from multiple Phase 3 trials. Better GI tolerability than oral semaglutide; higher discontinuation rates than oral semaglutide at comparable doses.
Category
Treatment Adherence
- Evidence Strength
- 7/10
- Reported Effectiveness
- 8/10
- Summary
- No fasting requirements, no injections, room temperature storage, once-daily dosing. REVISE study data on patient preferences.
Category
Heart Health
- Evidence Strength
- 6/10
- Reported Effectiveness
- 6/10
- Summary
- Improvements in systolic BP, triglycerides, cholesterol observed across trials. No dedicated CVOT.
Category
Blood Pressure
- Evidence Strength
- 6/10
- Reported Effectiveness
- 6/10
- Summary
- Systolic BP reduction of ~5-6 mmHg observed in clinical trials. Being studied for hypertension in obesity.
Category
Mood & Wellbeing
- Evidence Strength
- 2/10
- Reported Effectiveness
- 4/10
- Summary
- Limited data. Broader GLP-1 class literature flags potential psychological effects warranting monitoring.
Category
Daily Functioning
- Evidence Strength
- 3/10
- Reported Effectiveness
- 5/10
- Summary
- Limited direct data. GI side effects during titration may temporarily affect daily functioning.
Categories with community data: 10 (limited; all anticipatory, based on clinical trial discussion)
Categories not scored (insufficient data): Muscle Growth, Food Noise, Energy Levels, Sleep Quality, Focus & Mental Clarity, Memory & Cognition, Anxiety, Stress Tolerance, Motivation & Drive, Emotional Aliveness, Emotional Regulation, Libido, Sexual Function, Joint Health, Inflammation, Pain Management, Recovery & Healing, Physical Performance, Gut Health, Digestive Comfort, Skin Health, Hair Health, Heart Rate & Palpitations, Hormonal Symptoms, Temperature Regulation, Fluid Retention, Body Image, Immune Function, Bone Health, Longevity & Neuroprotection, Cravings & Impulse Control, Social Connection, Withdrawal Symptoms, Other
Benefits & Potential Effects
The Basics
The primary researched benefit of orforglipron is weight loss. In the largest clinical trial (ATTAIN-1), participants on the highest dose lost an average of 11.2% of their body weight over 72 weeks. For someone weighing 240 pounds, that translates to roughly 27 pounds. More than half of participants on the highest dose lost at least 10% of their body weight.
For people with type 2 diabetes, the benefits extend to blood sugar control. Orforglipron reduced HbA1c by up to 2.2 percentage points, and in head-to-head testing it outperformed oral semaglutide on both blood sugar and weight loss measures. More than 85% of patients achieved HbA1c below 7%, a threshold that most diabetes guidelines consider well-controlled.
Beyond weight and blood sugar, clinical trials documented improvements in waist circumference, blood pressure, triglycerides, and cholesterol. These changes collectively reduce cardiovascular risk, though dedicated heart outcomes studies for orforglipron have not been completed.
The convenience factor is significant and should not be underestimated. Orforglipron is a once-daily pill that can be taken any time, with or without food. It does not require refrigeration. For people who are needle-averse, travel frequently, or prefer simplicity in their medication routine, these practical advantages are meaningful.
The Science
Documented benefits from Phase 2 and Phase 3 clinical trials:
- Body weight reduction: -11.2% (36 mg, 72 weeks, ATTAIN-1) [4]; -14.7% (45 mg, 36 weeks, Phase 2, not yet plateaued) [8]
- HbA1c reduction: -1.6% (36 mg, 40 weeks, ACHIEVE-1) [5]; -2.2% (36 mg, 52 weeks, ACHIEVE-3) [6]
- Glycemic targets: 85.4% of patients achieved HbA1c <7% with 36 mg (ACHIEVE-3) [6]
- Systolic blood pressure: reduction of approximately 5-6 mmHg [4][5]
- Triglycerides: significant reduction across trials [4][6]
- Non-HDL, VLDL, total cholesterol: significant improvements in ACHIEVE-3 [6]
- Waist circumference: significant reduction in ATTAIN-1 [4]
- Body composition: approximately 75:25 fat-to-lean mass loss ratio (Phase 2 DEXA data) [9]
The benefits outlined above span multiple body systems, and your experience will be uniquely yours. Rather than guessing which effects are attributable to this compound versus other factors in your life, Doserly helps you log specific outcomes alongside your protocol details, building a clear picture of what's changing and when.
Over weeks and months, this creates something more useful than any anecdotal report: your own evidence-based record of how this compound affects you personally, at your specific dose, within the context of your full health protocol. When it's time to decide whether to continue, adjust, or discontinue, you have real data to inform that conversation with your healthcare provider.
Connect protocol changes to labs and health markers.
Doserly can keep lab results, biomarkers, symptoms, and dose history close together so follow-up conversations have better context.
Insights
Labs and trends

Doserly organizes data; it does not diagnose or interpret labs for you.
Side Effects & Safety Considerations
The Basics
Like all GLP-1 receptor agonists, the most common side effects of orforglipron involve the gastrointestinal system. Nausea, diarrhea, vomiting, and constipation are the most frequently reported effects. In the ATTAIN-1 trial, approximately 50% of participants on orforglipron experienced GI events, compared to roughly 74-80% for oral semaglutide. This makes orforglipron notably more tolerable on the GI front.
An interesting distinction from semaglutide: with orforglipron, diarrhea tends to be the most commonly reported GI symptom, whereas nausea leads for semaglutide. This difference may be relevant for people choosing between the two options.
Most side effects are mild to moderate in severity and tend to occur during the dose escalation period. Starting at a low dose and gradually increasing helps the body adjust. Symptoms typically improve after the first 4-8 weeks. About 10% of participants on the highest dose discontinued treatment due to side effects, compared to about 3% on placebo.
The contraindications for orforglipron align with the broader GLP-1 drug class: personal or family history of medullary thyroid carcinoma, multiple endocrine neoplasia syndrome type 2, known hypersensitivity to the active ingredient, and pregnancy or breastfeeding. A slight increase in resting heart rate has been observed, consistent with the GLP-1 class effect.
The Science
Safety data from the ATTAIN-1 Phase 3 trial (N=3,127) at 36 mg [4]:
Adverse Event
Nausea
- Orforglipron 36 mg
- 33.7%
- Placebo
- 10.4%
Adverse Event
Diarrhea
- Orforglipron 36 mg
- 23.1%
- Placebo
- 9.6%
Adverse Event
Vomiting
- Orforglipron 36 mg
- 24.0%
- Placebo
- 3.5%
Adverse Event
Constipation
- Orforglipron 36 mg
- 25.4%
- Placebo
- 9.3%
Adverse Event
Overall GI events
- Orforglipron 36 mg
- ~50%
- Placebo
- ~30%
Adverse Event
Discontinuation due to AEs
- Orforglipron 36 mg
- 10.3%
- Placebo
- 2.7%
In the ACHIEVE-3 head-to-head trial, treatment discontinuation due to adverse events was 8.7% (12 mg) and 9.7% (36 mg) for orforglipron versus 4.5% (7 mg) and 4.9% (14 mg) for oral semaglutide [6]. This suggests that while orforglipron has lower overall GI event rates, its discontinuation rates are modestly higher than those of oral semaglutide at equivalent therapeutic doses.
A mean increase in pulse rate was noted in the orforglipron groups, consistent with the GLP-1 RA class effect [6]. No hepatic safety signals were identified across trials. Broader GLP-1 class concerns, including reports of potential impact on suicidal behavior from meta-analysis of randomized controlled trials, warrant continued monitoring [12].
Side effect profiles are most useful when you can compare them against your own experience in real time. Doserly lets you log symptoms, severity, and timing alongside your dosing data, creating a side-by-side view of your protocol and your body's response.
This kind of systematic tracking catches things that memory alone misses. A subtle mood shift that began three days after a dose increase. Sleep disruption that correlates with evening administration. These patterns become visible when the data is laid out on a timeline, and they give your healthcare provider actionable information rather than vague concerns. Early detection of emerging side effects means earlier intervention.
Capture changes while they are still fresh.
Log symptoms, energy, sleep, mood, and other observations alongside protocol events so patterns do not live only in memory.
Trend view
Symptom timeline

Symptom tracking is informational and should be interpreted with a qualified clinician.
Dosing Protocols
The Basics
Orforglipron is taken as a once-daily pill. In clinical trials, the doses studied were 3 mg, 6 mg, 12 mg, and 36 mg for approved indications, with 45 mg tested in earlier Phase 2 trials. All trials used a dose escalation approach, starting at 1 mg and gradually increasing over several weeks to the target maintenance dose.
The rationale for gradual dose escalation is to allow the gastrointestinal system to adapt, reducing the severity of nausea, vomiting, and other GI effects that are most common in the early weeks. This approach is standard practice across all GLP-1 receptor agonist medications.
The 36 mg dose has consistently shown the greatest efficacy for both weight loss and blood sugar control across all trials. Lower doses (6 mg, 12 mg) provide intermediate levels of benefit and may be appropriate for individuals who cannot tolerate the full dose.
Orforglipron can be taken at any time of day, with or without food, and without water restrictions. This is a notable difference from oral semaglutide, which requires a 30-minute fast and specific water volume limitations.
The Science
Clinical trial dosing protocols:
ATTAIN-1 (obesity): 6 mg, 12 mg, or 36 mg once daily for 72 weeks. Dose escalation from 1 mg starting dose with incremental increases to target dose [4].
ACHIEVE-1 (T2D): 3 mg, 12 mg, or 36 mg once daily for 40 weeks. Starting dose of 1 mg orforglipron once daily with dose escalation to target [5].
ACHIEVE-3 (T2D, head-to-head): 12 mg or 36 mg once daily for 52 weeks. Starting dose of 1 mg with escalation (including an intermediate step at 3 mg) [6].
Dose-response relationship: A clear dose-dependent relationship has been established. The 36 mg dose consistently produces the greatest weight loss and HbA1c reduction. Phase 2 data at 45 mg showed even greater weight loss (14.7% at 36 weeks) but this dose was not carried forward into Phase 3 [8].
What to Expect
Based on clinical trial data and published outcomes, the following represents a general timeline of what participants experienced. Individual responses vary significantly.
Weeks 1-4 (Dose Escalation Phase):
Starting at 1 mg daily with gradual increases. This is when GI side effects are most common. Nausea, changes in appetite, and altered bowel habits may occur as the body adjusts. Some appetite suppression typically begins. Clinical trials documented improvements in blood sugar markers as early as week 4.
Weeks 4-12 (Adaptation Period):
As the dose escalates toward the target, appetite suppression becomes more pronounced. GI side effects typically begin to diminish. Early weight loss becomes noticeable. For people with diabetes, blood sugar improvements become more consistent.
Weeks 12-36 (Active Response Period):
Weight loss is ongoing and typically has not plateaued at this point. Blood sugar control, blood pressure, and lipid improvements continue to accrue. Most people have adapted to the GI effects by this stage. Phase 2 data showed weight loss still continuing at 36 weeks without plateau.
Weeks 36-72 (Continued Response):
Weight loss continues to accumulate, though the rate may slow as the body approaches a new equilibrium. At 72 weeks in ATTAIN-1, the 36 mg group had achieved 11.2% average weight loss. Metabolic improvements in blood sugar, blood pressure, and cholesterol remain sustained.
After Stopping:
Based on data from other GLP-1 drugs, weight regain of approximately two-thirds of lost weight is expected within one year of discontinuation. The ATTAIN-MAINTAIN trial suggests transitioning from injectable GLP-1 drugs to orforglipron can help maintain most of the weight loss.
Interaction Compatibility
Potentially Complementary
- Semaglutide: Same drug class (GLP-1 RA) but injectable. Orforglipron may serve as a step-down maintenance option after initial weight loss with semaglutide. ATTAIN-MAINTAIN data supports this transition (0.9 kg regain at 52 weeks).
- Tirzepatide: Dual GIP/GLP-1 agonist. More potent for weight loss (20-22%). Orforglipron may serve as a maintenance alternative, though transition data shows more regain (5.0 kg) than from semaglutide.
- Retatrutide: Triple agonist (GLP-1/GIP/Glucagon). Investigational. Different mechanism with potentially complementary approach if sequential use is considered.
- NAD+: Metabolic support. Some community discussion suggests NAD+ supplementation may help with GLP-1-associated fatigue and support fat oxidation.
- MOTS-C: Mitochondrial peptide. May complement metabolic effects through AMPK activation and exercise-mimetic pathways.
- AOD-9604: Fat loss peptide. May provide additional lipolytic support, though evidence for the combination is limited.
- Tesamorelin: Lean mass preservation. May help offset lean mass loss during GLP-1-mediated weight reduction.
- Metformin: ACHIEVE trials included patients on metformin. Additive glycemic benefits without increased hypoglycemia risk [6].
- SGLT2 inhibitors: Early combination data suggests additive benefits without proportional increase in hypoglycemia risk [1].
Use With Caution
- Other GLP-1 receptor agonists (concurrent use): Do not combine orforglipron with other GLP-1 RAs. Same receptor target creates redundancy and increased GI side effect risk.
- Insulin and sulfonylureas: Increased hypoglycemia risk when combined with glucose-lowering agents. Dose adjustments of the companion medication may be necessary.
- Oral medications with narrow therapeutic windows: Orforglipron slows gastric emptying, which may affect the absorption kinetics of other oral medications taken concurrently.
Contraindicated
- Personal or family history of medullary thyroid carcinoma
- Multiple endocrine neoplasia syndrome type 2 (MEN 2)
- Known hypersensitivity to orforglipron
- Pregnancy or breastfeeding
Administration Guide
Orforglipron is administered as a once-daily oral pill. Unlike injectable peptides, no reconstitution, syringes, or sterile technique is required.
Materials required:
- Orforglipron tablets (at prescribed dose)
- Water (any amount; no volume restriction)
Timing considerations:
- Can be taken at any time of day
- No fasting requirement before or after dosing
- No food restrictions at the time of administration
- No water volume restrictions
- Consistency in timing (same time each day) may aid habit formation and adherence but is not pharmacologically required
Dose escalation:
Clinical trials started all participants at 1 mg once daily, with gradual increases over several weeks to the target maintenance dose. This titration approach minimizes GI side effects. The exact escalation schedule has not been fully published for all trials but involves weekly or biweekly dose increases.
Post-administration care:
- Monitor for GI symptoms (nausea, diarrhea, constipation) especially during dose escalation
- No specific post-dose activity restrictions
- If a dose is missed, clinical trial protocols have not published specific guidance. Consult a healthcare provider for recommendations on missed-dose management.
Supplies & Planning
Orforglipron is an oral tablet medication. Supply planning is straightforward compared to injectable peptides.
What is generally needed:
- Orforglipron tablets (available in 3 mg, 6 mg, 12 mg, and 36 mg doses based on clinical trials)
- A pill organizer may be helpful for daily adherence tracking
- No refrigeration equipment required
- No syringes, needles, alcohol swabs, or reconstitution supplies needed
Cost considerations:
Eli Lilly has indicated projected pricing of $149/month for the starting dose and up to $399/month for maintenance doses at self-pay pricing, with insurance coverage expected to reduce costs significantly. These prices reflect pre-approval estimates and may change.
Treatment duration:
Clinical trials evaluated 40-72 week treatment periods. Orforglipron is intended for long-term, continuous use. Weight regain is expected upon discontinuation, consistent with the GLP-1 drug class.
Storage & Handling
Orforglipron is stored at controlled room temperature. This is a significant practical advantage over injectable GLP-1 drugs, which typically require refrigeration.
Storage conditions:
- Room temperature storage (specific temperature range to be defined in prescribing information upon approval)
- No refrigeration required
- No special light protection requirements documented in clinical trial materials
- Shelf-stable oral tablet formulation
Practical advantages:
- No cold chain required for shipping or travel
- No concerns about temperature excursions during transit
- Can be stored alongside other daily medications
- No reconstitution stability concerns (not applicable to oral formulation)
Lifestyle Factors
The effectiveness of any weight management or metabolic medication is significantly influenced by lifestyle factors. Clinical trials of orforglipron required participants to follow "healthy diet and physical activity" alongside the medication.
Nutrition:
High protein intake (1.5-2.3 g/kg of fat-free mass daily) is recommended during any GLP-1-mediated weight loss to help preserve lean body mass. The approximately 75:25 fat-to-lean mass loss ratio observed with orforglipron in Phase 2 trials is favorable, but resistance training and protein intake can further improve this ratio. Adequate hydration is important, particularly if experiencing GI side effects like diarrhea or vomiting.
Exercise:
Resistance training (3-5 sessions per week) is strongly recommended during GLP-1-mediated weight loss. A case series documented patients achieving 13-33% total weight loss with lean mass changes ranging from -6.9% to actual gains of +5.8% when following structured resistance training programs alongside GLP-1 medications. Aerobic exercise complements the metabolic benefits.
Sleep:
Adequate sleep (7-9 hours) supports metabolic function and recovery. GLP-1 drugs can affect energy levels, particularly during dose escalation. Orforglipron is also being studied for obstructive sleep apnea in adults with obesity, suggesting potential sleep-related benefits from weight reduction.
Monitoring:
Regular monitoring of body weight, waist circumference, blood pressure, HbA1c (for people with diabetes), and lipid panels is recommended during treatment. Fasting glucose and HbA1c at baseline, followed by periodic reassessment, helps track metabolic response.
The lifestyle factors above, nutrition, exercise, sleep, stress management, are not just nice-to-haves alongside a peptide protocol. They're force multipliers. Doserly lets you track these inputs alongside your compounds, building a complete picture of what your body is receiving and how it's responding.
When everything lives in one dashboard, patterns emerge. You can see whether training days correlate with better biomarker trends, whether your sleep scores predict next-day recovery quality, or whether stress spikes derail your progress in measurable ways. This kind of integrated tracking turns the lifestyle recommendations in this section from abstract advice into actionable, personalized insight.
Keep sensitive protocol records in a purpose-built app.
Doserly is designed for private health tracking with structured records, offline-ready workflows, and exportable history when you need it.
Privacy
Health records

Privacy controls help you manage records; keep clinical records where required.
Regulatory Status & Research Classification
United States (FDA):
Orforglipron is investigational. Eli Lilly submitted a New Drug Application (NDA) to the FDA in late 2025 for the treatment of adults with obesity or overweight. The FDA granted priority review designation. A decision on the obesity indication is expected in Q2 2026 (potentially as early as March 2026). Submission for type 2 diabetes in the U.S. is planned later in 2026. Orforglipron received a Commissioner's National Priority Review Voucher. Lilly has also submitted regulatory applications to authorities in over 40 countries.
Active Clinical Trials:
- ATTAIN-1 (NCT05869903): Obesity, Phase 3
- ATTAIN-2 (NCT05872620): Obesity with T2D, Phase 3
- ATTAIN-MAINTAIN: Switch from injectable to oral GLP-1, Phase 3
- ATTAIN-OSA: Obstructive sleep apnea with obesity, Phase 3
- ACHIEVE-1 (NCT05971940): T2D monotherapy, Phase 3
- ACHIEVE-3 (NCT06045221): T2D head-to-head vs oral semaglutide, Phase 3
- ACHIEVE-5: T2D add-on to insulin glargine, Phase 3
- ACHIEVE-2: T2D vs dapagliflozin, Phase 3
- Additional trials for hypertension in obesity
Canada (Health Canada): Regulatory status not publicly confirmed as of March 2026.
United Kingdom (MHRA): Regulatory status not publicly confirmed as of March 2026.
Australia (TGA): Regulatory status not publicly confirmed as of March 2026.
European Union (EMA): Regulatory status not publicly confirmed as of March 2026. Lilly has indicated submission to regulators in over 40 countries.
WADA Status: Not listed on the WADA Prohibited List as a named substance. However, GLP-1 receptor agonists as a class may be subject to restrictions depending on the specific sporting authority and anti-doping regulations. Athletes should verify status with their specific governing body.
Regulatory status changes frequently. Always verify the current legal status of any compound in your specific country or jurisdiction before making any decisions.
FAQ
What is orforglipron?
Orforglipron is an investigational once-daily oral medication developed by Eli Lilly that activates GLP-1 receptors to promote weight loss and improve blood sugar control. It is a non-peptide small molecule, not a peptide, which allows it to be taken as a pill without the fasting requirements or absorption limitations of peptide-based oral GLP-1 drugs.
Is orforglipron FDA-approved?
No. As of March 2026, orforglipron has not received FDA approval for any indication. A New Drug Application is under priority review for obesity, with a decision expected in Q2 2026. It is not available for prescription or consumer purchase.
How much weight can you lose on orforglipron?
Based on Phase 3 clinical trial data, participants on the highest dose (36 mg) lost an average of 11.2% of their body weight over 72 weeks (approximately 27 pounds for an average starting weight). About 54.6% of participants lost at least 10% of their body weight, and 18.4% lost 20% or more. Earlier Phase 2 data at a higher dose (45 mg) showed 14.7% weight loss at 36 weeks with no plateau.
How does orforglipron compare to Ozempic or Wegovy?
Based on available trial data (not direct head-to-head comparison in obesity), injectable semaglutide (Wegovy) produces approximately 14.9% weight loss at 68 weeks, compared to orforglipron's 11.2% at 72 weeks. Orforglipron's advantages are oral convenience, no fasting requirement, no injections, and room temperature storage. In the ACHIEVE-3 head-to-head trial (in type 2 diabetes), orforglipron 36 mg outperformed oral semaglutide 14 mg for both weight loss and blood sugar control.
Can orforglipron be taken with food?
Yes. Unlike oral semaglutide (Rybelsus/Wegovy pill), which requires 30 minutes of fasting and limited water, orforglipron can be taken at any time of day with or without food. This is because orforglipron has approximately 79% oral bioavailability compared to oral semaglutide's approximately 1%.
What are the main side effects?
The most common side effects are gastrointestinal: nausea (33.7%), constipation (25.4%), vomiting (24.0%), and diarrhea (23.1%) at the 36 mg dose. These are most common during dose escalation and typically improve over the first 4-8 weeks. About 10% of participants discontinued treatment due to side effects.
Does orforglipron cause muscle loss?
All weight loss, whether from medication, diet, or surgery, involves some loss of lean body mass alongside fat mass. Phase 2 data showed orforglipron produced a 75:25 fat-to-lean mass loss ratio, which is comparable to or slightly better than other GLP-1 medications. Resistance training and adequate protein intake can substantially preserve lean mass during treatment.
What happens when you stop taking orforglipron?
Based on data from other GLP-1 drugs, weight regain of approximately two-thirds of lost weight is expected within one year of discontinuation. The ATTAIN-MAINTAIN trial suggests orforglipron may serve as a maintenance therapy to preserve weight loss achieved with injectable GLP-1 drugs.
How much will orforglipron cost?
Eli Lilly has indicated a self-pay price starting at $149/month for the lowest dose and up to $399/month for maintenance doses, available through their LillyDirect pharmacy channel. Insurance coverage is expected to reduce costs significantly, though specific coverage details will depend on individual plans and formulary decisions after approval.
Sources & References
- Kansakar U, Jankauskas SS, Pande S, Mone P, Varzideh F, Santulli G. "Orforglipron: A Comprehensive Review of an Oral Small-Molecule GLP-1 Receptor Agonist for Obesity and Type 2 Diabetes." Int J Mol Sci. 2026;27(3):1409. doi:10.3390/ijms27031409. PMID: 41683830. https://pmc.ncbi.nlm.nih.gov/articles/PMC12898445/
- Pratt E, Ma X, Liu R, Robins D, Haupt A, Coskun T, Sloop KW, Benson C. "Orforglipron (LY3502970), a novel, oral non-peptide glucagon-like peptide-1 receptor agonist: A Phase 1a, blinded, placebo-controlled, randomized, single- and multiple-ascending-dose study in healthy participants." Diabetes Obes Metab. 2023;25:2634-2641. doi:10.1111/dom.15184.
- Sloop KW, et al. "The pharmacological basis for nonpeptide agonism of the GLP-1 receptor." Science Translational Medicine. 2024. doi:10.1126/scitranslmed.adp5765. https://www.science.org/doi/10.1126/scitranslmed.adp5765
- Wharton S, Aronne LJ, Stefanski A, et al. "Orforglipron, an oral small-molecule GLP-1 receptor agonist for obesity treatment (ATTAIN-1)." New England Journal of Medicine. 2025. doi:10.1056/NEJMoa2511774. https://www.nejm.org/doi/full/10.1056/NEJMoa2511774
- Horn DB, Ryan DH, Giljanovic Kis S, et al. "Orforglipron for the treatment of obesity in people with type 2 diabetes (ATTAIN-2)." The Lancet. 2025. doi:10.1016/S0140-6736(25)02165-8.
- Rosenstock J, Manghi FP, et al. "Efficacy and safety of once-daily oral orforglipron compared with oral semaglutide in adults with type 2 diabetes (ACHIEVE-3)." The Lancet. 2026. doi:10.1016/S0140-6736(26)00202-3. https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(26)00202-3/abstract
- Pratt E, Ma X, Liu R, Robins D, Coskun T, Sloop KW, Haupt A, Benson C. "Orforglipron (LY3502970), a novel, oral non-peptide glucagon-like peptide-1 receptor agonist: A Phase 1b, multicentre, blinded, placebo-controlled, randomized, multiple-ascending-dose study in people with type 2 diabetes." Diabetes Obes Metab. 2023;25:2642-2649.
- Wharton S, Blevins T, Connery L, et al. "Daily Oral GLP-1 Receptor Agonist Orforglipron for Adults with Obesity (Phase 2)." New England Journal of Medicine. 2023. doi:10.1056/NEJMoa2302392.
- Body composition DEXA substudy data from Phase 2 orforglipron trials. Referenced in comparative analyses.
- Eli Lilly. "Lilly's orforglipron helped people maintain weight loss after switching from injectable incretins to oral GLP-1 therapy in first-of-its-kind Phase 3 trial (ATTAIN-MAINTAIN)." Press release, December 2025. https://investor.lilly.com/
- Frias JP, Hsia S, Eyde S, et al. "Efficacy and safety of oral orforglipron in patients with type 2 diabetes: a multicentre, randomised, dose-response, phase 2 study." The Lancet. 2023. doi:10.1016/S0140-6736(23)01302-8.
- GLP-1 receptor agonist class safety monitoring. Meta-analysis of impact on suicidal behavior in randomized controlled trials. Referenced in broader GLP-1 safety literature.
Related Peptide Guides
- Semaglutide — Injectable GLP-1 RA; the established benchmark for GLP-1 efficacy
- Tirzepatide — Dual GIP/GLP-1 agonist with higher weight loss efficacy
- Retatrutide — Investigational triple agonist (GLP-1/GIP/Glucagon)
- Cagrilintide — Amylin analog studied in combination with semaglutide (CagriSema)
- Mazdutide — Dual GLP-1/Glucagon agonist
- Survodutide — Dual GLP-1/Glucagon agonist
- Tesofensine — Triple monoamine reuptake inhibitor for weight management
- AOD-9604 — Fat loss peptide
- NAD+ — Metabolic support, commonly stacked with GLP-1 protocols
- MOTS-C — Mitochondrial peptide, exercise mimetic
- Tesamorelin — GHRH analog for visceral fat reduction and lean mass preservation
- SLU-PP-332 + Orforglipron — Blend available on the platform