Thymosin Alpha-1: Complete Research Guide
On this page
Quick Reference Card
Attribute
Also Known As
- Detail
- Thymalfasin, Zadaxin, Talpha1, Thymosin-alpha-1, TA1
Attribute
Administration
- Detail
- Subcutaneous injection (primary); intramuscular injection (alternative)
Attribute
Research Status
- Detail
- Approved pharmaceutical in 35+ countries (as Zadaxin). Not FDA-approved in the United States. Orphan drug designation for melanoma, hepatitis, DiGeorge syndrome.
Attribute
Typical Dose Range
- Detail
- 1.6 mg twice weekly (clinical standard); 300-500 mcg daily (community protocols); 0.8-1.5 mg 2-3x/week (practitioner protocols)
Attribute
Half-Life
- Detail
- Approximately 2 hours (serum)
Attribute
Cycle Length
- Detail
- 8-24 weeks depending on indication. No cycling protocol established in clinical literature; trials use continuous dosing.
Attribute
Storage
- Detail
- Lyophilized: -20C or below for long-term, 2-8C for short-term. Reconstituted: 2-8C, use within 7 days. Do not freeze reconstituted solution.
Overview / What Is Thymosin Alpha-1?
The Basics
Thymosin Alpha-1 (TA1) is a peptide that your thymus gland naturally produces. The thymus sits behind your breastbone and serves as a training facility for your immune system's T-cells, the specialized cells that learn to recognize and respond to infections, cancers, and other threats. Think of the thymus as a school for immune cells, and TA1 as one of its most important teaching signals.
As you age, your thymus shrinks. By your 50s, it has lost most of its functional tissue, producing less TA1 and fewer well-trained immune cells. This decline contributes to the slower immune responses, increased vulnerability to infections, and reduced vaccine effectiveness that come with aging. Supplementing with synthetic TA1 aims to restore some of the immune training capacity that time naturally erodes.
What makes TA1 unusual among peptides is its clinical pedigree. First isolated in 1977 by Allan Goldstein's laboratory, the synthetic version (thymalfasin, brand name Zadaxin) has been approved in more than 35 countries for treating chronic hepatitis B and C. It has been studied in over 30 clinical trials involving more than 11,000 subjects [1][2]. That track record puts it in rare company; most research peptides have far less human data behind them.
TA1 is not an immune booster in the conventional sense. It does not simply turn your immune system up. It is an immune modulator, meaning it helps your immune system make better decisions about when to attack and when to stand down. This distinction matters because an overactive immune system causes autoimmune damage, while an underactive one leaves you vulnerable to infection. TA1 aims for the sweet spot between those extremes.
The Science
Thymosin Alpha-1 (Talpha1) is a 28-amino acid peptide (molecular weight 3,108.29 Da) originally isolated from thymosin fraction 5, a crude extract of calf thymus tissue [1]. It is endogenously produced by thymic epithelial cells and released into the circulation, where it modulates both innate and adaptive immune responses [2].
The synthetic version, thymalfasin (INN), is manufactured via solid-phase peptide synthesis and is marketed as Zadaxin in multiple jurisdictions. TA1 is distinguished from other thymic peptides (Thymosin Beta-4, Thymulin, Thymalin) by its specific amino acid sequence, mechanism of action, and extensive clinical validation [1][2].
TA1 has accumulated a clinical dataset across viral hepatitis (approved indication in 35+ countries), sepsis, cancer adjunctive therapy, and viral infections including HIV and SARS-CoV-2. Meta-analyses of hepatitis B trials demonstrate improved virological response when TA1 is combined with antiviral therapy [3]. A large multicenter RCT demonstrated approximately 9% mortality reduction in sepsis patients [4].
Molecular Identity
Attribute
Common Names
- Detail
- Thymosin Alpha-1, Thymalfasin, Zadaxin, Talpha1, TA1
Attribute
Amino Acid Sequence
- Detail
- Ac-Ser-Asp-Ala-Ala-Val-Asp-Thr-Ser-Ser-Glu-Ile-Thr-Thr-Lys-Asp-Leu-Lys-Glu-Lys-Lys-Glu-Val-Val-Glu-Glu-Ala-Glu-Asn-OH
Attribute
Single-Letter Code
- Detail
- Ac-SDAAVDTSSEITTKDLKEKKEVVEEAEN
Attribute
Molecular Formula
- Detail
- C129H215N33O55
Attribute
Molecular Weight
- Detail
- 3,108.29 Da
Attribute
CAS Number
- Detail
- 62304-98-7
Attribute
PubChem CID
- Detail
- 16132303 (primary); 16130571 (thymalfasin entry)
Attribute
FDA UNII Code
- Detail
- W0B22ISQ1C
Attribute
Structural Type
- Detail
- Linear polypeptide, 28 amino acids, with N-terminal acetylation
Attribute
Functional Class
- Detail
- Thymic peptide hormone, immunomodulator, biological response modifier
Attribute
Key Features
- Detail
- N-terminal acetylation essential for activity; contains no aromatic amino acids; remarkably thermostable (stable at 80-90C); net charge approximately -5 to -6 at physiological pH
Mechanism of Action
The Basics
Your immune system has two main divisions: a fast-response team (innate immunity) that deals with threats immediately but generically, and a specialized force (adaptive immunity) that learns to recognize specific threats and remember them for next time. TA1 improves the performance of both, but its most consequential effect is on the specialized force.
Within the adaptive immune system, there is a critical balance between attack cells (Th17 cells, which drive inflammation and target threats) and regulatory cells (Tregs, which prevent the immune system from attacking your own tissues). In autoimmune conditions, the balance tips too far toward attack. In immunodeficiency, neither side works properly. TA1 works primarily by expanding the regulatory cell population, adding weight to the Treg side of the balance rather than simply dampening the attack side [5][6].
This is a meaningful distinction. Conventional immunosuppressants work by removing something: corticosteroids turn down the entire immune system, and biologic drugs block specific inflammatory pathways. TA1 works by adding something: more regulatory cells that teach the rest of the immune system when to stand down. The result is an immune system that retains its ability to fight infections while gaining better restraint against attacking the body's own tissues.
TA1 also upgrades the immune system's intelligence-gathering operation. It matures dendritic cells, the "instructors" that teach T-cells what to attack. When dendritic cells are immature, they give poor briefings, and T-cells respond sluggishly or inaccurately. TA1 produces better-trained instructors, which leads to better-trained responders [7].
The Science
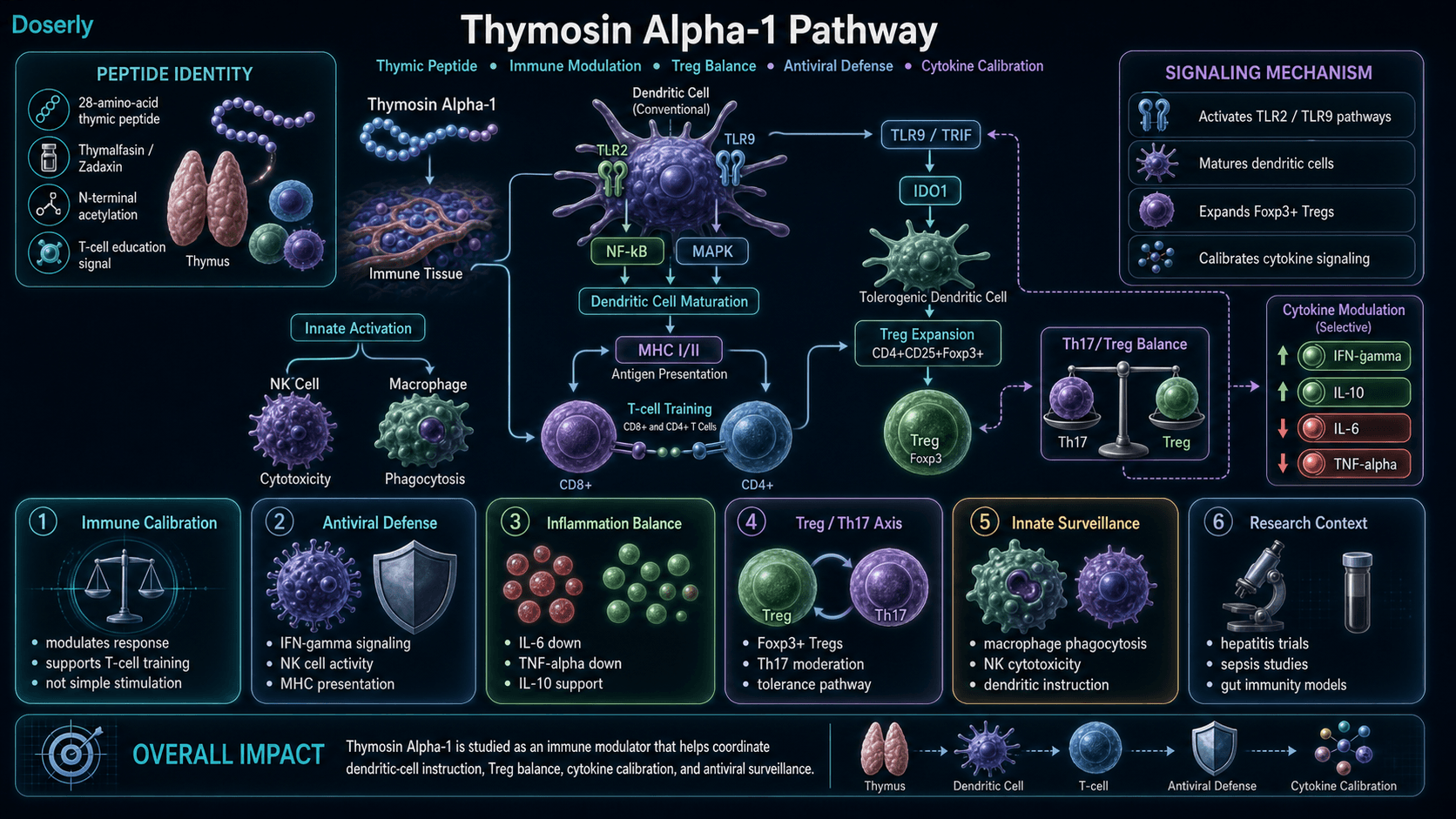
TA1 exerts its immunomodulatory effects through multiple intersecting pathways:
TLR Signaling and Dendritic Cell Activation. TA1 acts as an agonist of Toll-like receptors TLR2 and TLR9 on dendritic cells and macrophages, activating NF-kB and MAPK pathways. This promotes dendritic cell maturation, enhanced antigen presentation via upregulated MHC class I and II expression, and increased production of IL-2, IFN-gamma, and IL-12 [7][8].
Regulatory T-Cell Expansion. TA1 promotes the development and expansion of CD4+CD25+Foxp3+ regulatory T-cells. Li et al. (2014) demonstrated that TA1 suppressed Th17 cell responses while simultaneously expanding Treg populations in rheumatoid arthritis models, shifting the Th17/Treg balance decisively toward immune regulation [5].
IDO1 Tolerance Pathway. Romani et al. (2007) demonstrated that TA1 activates dendritic cells through the TLR-9/TRIF signaling pathway, promoting expression of indoleamine 2,3-dioxygenase 1 (IDO1) [7]. IDO1 establishes tolerogenic environments where dendritic cells train new Tregs instead of arming effector cells. Renga et al. (2020) showed context-dependent behavior: TA1 induced IDO1-dependent tolerance in gut tissue while preserving aggressive immune surveillance in tumor tissue, increasing CD8+ T-cell infiltration and decreasing Tregs at tumor sites [9].
Selective Cytokine Modulation. TA1 reduces IL-6 and TNF-alpha while preserving or enhancing IFN-gamma production and promoting IL-10, an anti-inflammatory cytokine. This selectivity pattern (pro-inflammatory cytokines down, antiviral and anti-inflammatory cytokines up or maintained) is the molecular signature of immune modulation rather than suppression [2][5].
NK Cell and Macrophage Enhancement. TA1 increases natural killer cell cytotoxicity and enhances macrophage phagocytic activity, strengthening innate immune surveillance [2][8].
Pathway Visualization
Pharmacokinetics
The Basics
TA1 has a short working life in your bloodstream. After a subcutaneous injection, it reaches peak levels within about two hours and then clears relatively quickly, with blood levels returning to baseline within 24 hours. This short presence in the blood does not mean the effects are equally short-lived. TA1 triggers changes in immune cell populations and cytokine signaling that persist well beyond the peptide's physical presence.
Think of it like a coach at a training session. The coach may only be present for two hours, but the skills the players learned last for the entire game. TA1's influence on T-cell maturation, Treg expansion, and dendritic cell programming continues after the peptide itself has been cleared.
This pharmacokinetic profile explains why clinical trials use twice-weekly dosing rather than daily administration: the immune system needs time to implement the instructions TA1 delivers before the next "coaching session." Some community protocols use daily dosing at lower amounts, operating on the theory that more frequent, smaller signals may produce different or complementary effects.
The Science
Following subcutaneous administration, TA1 is rapidly absorbed with peak serum concentrations (Tmax) achieved within approximately 2 hours [10]. The serum elimination half-life is approximately 2 hours in humans. Blood levels return to baseline within 24 hours of a single dose [10].
Pharmacokinetic parameters:
- Tmax: ~2 hours (subcutaneous)
- t1/2: ~2 hours (serum elimination)
- Steady state: ~9 hours with regular dosing
- Clearance: ~3% remaining at 10.1 hours post-dose
- Bioavailability: Excellent subcutaneous bioavailability; limited oral bioavailability due to GI degradation
The short serum half-life represents the primary pharmacokinetic limitation. Fc-fusion protein variants (Talpha1-Fc) have been developed to extend the half-life to approximately 25 hours through conjugation with human IgG4 Fc domain [11]. These modified forms have shown enhanced efficacy in preclinical breast cancer models [11].
N-terminal acetylation at the serine residue is essential for biological activity and provides protection against proteolytic degradation. The absence of aromatic amino acids contributes to the peptide's remarkable thermal stability, remaining structurally stable at temperatures up to 80-90C [10].
Research & Clinical Evidence
Chronic Hepatitis B and C
The Basics
This is TA1's strongest clinical application and the basis for its approval in 35+ countries. When combined with antiviral therapy, TA1 helps the immune system clear hepatitis B and C infections more effectively than antivirals alone. The benefit comes not from TA1 directly killing the virus, but from improving the immune system's ability to identify and eliminate virus-infected liver cells.
While direct-acting antiviral drugs have since largely replaced TA1 for hepatitis treatment (they achieve higher cure rates), the hepatitis data remains valuable because it established TA1's safety profile across thousands of patients and proved that immune modulation, not direct antiviral activity, was the mechanism of benefit.
The Science
Yang et al.'s 2013 meta-analysis of randomized controlled trials evaluating thymalfasin for chronic hepatitis B found that TA1 combined with antivirals produced a complete virological response rate of approximately 40.6% at the standard dose of 1.6 mg subcutaneously twice weekly [3]. Liu et al. (2020) confirmed these findings in a meta-analysis of TA1 combined with pegylated interferon alpha [12].
A separate meta-analysis (You et al., 2006) evaluating 8 randomized trials found significantly higher complete response rates versus controls, improved HBV DNA clearance, enhanced HBeAg seroconversion, and synergistic effects with interferon therapy [13].
Sepsis and Critical Care
The Basics
Sepsis is a life-threatening condition where the immune system's response to infection spirals out of control, damaging organs and threatening survival. TA1 has shown promise in this setting because sepsis involves both immune overactivation (too much inflammation) and immune exhaustion (T-cells burning out), and TA1 addresses both problems through its modulatory mechanism.
The Science
A large multicenter RCT in China demonstrated approximately 9% lower mortality in the TA1 treatment group among sepsis patients. The protocol used 1.6 mg subcutaneously twice daily for five days, then once daily [4]. TA1 treatment was associated with improved lymphocyte recovery, increased monocyte HLA-DR expression, and reduced secondary infection rates [4][14].
Cancer Immunotherapy
The Basics
TA1 has been studied as a supporting treatment alongside standard cancer therapies including chemotherapy and radiation. The evidence suggests it may help the immune system recover from the immunosuppressive effects of cancer treatment, potentially reducing side effects and improving quality of life during therapy. Its role appears to be supportive rather than primary.
The Science
TA1 has been evaluated as an adjunct in melanoma (combined with dacarbazine), hepatocellular carcinoma, non-small cell lung cancer, and breast cancer [1][15]. Maio et al. (2010) conducted a large randomized study showing that thymosin alpha-1 combined with dacarbazine and interferon showed increased progression-free survival in metastatic melanoma with no increase in toxicity [15]. A long-acting Talpha1-Fc fusion protein demonstrated enhanced efficacy against breast cancer cells in preclinical models, boosting CD4 and CD8 cell levels while increasing IFN-gamma and IL-2 [11].
Costantini et al. (2019) reviewed TA1 as a cancer immunotherapy agent, noting its capacity to enhance tumor-infiltrating lymphocyte activity and improve treatment response when combined with chemotherapy or checkpoint inhibitors [16]. Wei et al. (2022) demonstrated that TA1 reverses M2 polarization of tumor-associated macrophages during efferocytosis, shifting the tumor microenvironment toward anti-tumor immunity [17].
COVID-19 and Viral Infections
The Basics
During the pandemic, TA1 was tested in COVID-19 patients. The pattern that emerged was instructive: it appeared most helpful when given early or during moderate illness, helping the immune system recover faster and reducing inflammatory markers. In patients already in the ICU with organ failure, it did not show consistent benefit. This aligns with TA1's nature as an immune educator; it works best when the immune system is still recoverable, not after catastrophic failure.
The Science
Observational data and meta-analyses demonstrated a timing-dependent response pattern. Soeroto et al. (2023) conducted a meta-analysis showing significant mortality reduction in moderate-to-critical COVID-19 patients receiving TA1 [18]. Early administration was associated with improved lymphocyte recovery and reduced progression to severe illness. A study of 25 critically ill patients showed daily TA1 for one week prevented lymphopenia versus untreated controls [2].
A University of Rome "Tor Vergata" open study of Long COVID (PASC) patients found persistent depletion of naive B and T cells, with TA1 improving restoration of appropriate immune response. The greatest benefit was seen in those who had more severe acute illness [19].
Gut Immunity (Preclinical)
The Basics
Some of the most intriguing recent research shows TA1 may help calm inappropriate immune attacks in gut tissue while leaving the immune system's cancer-fighting ability intact elsewhere. In animal models of both ulcerative colitis and Crohn's disease, TA1 reduced all measured markers of inflammation in the gut. However, this research comes from a single laboratory group, and no human trials for inflammatory bowel disease have been conducted despite over a decade of compelling animal data.
The Science
Renga et al. (2020) demonstrated that TA1 protected mice from both DSS-induced colitis (modeling ulcerative colitis) and TNBS-induced colitis (modeling Crohn's disease). TA1 reduced MPO activity, TNF-alpha, IL-1beta, IL-17A, and IL-17F while increasing IL-10 in both models [9]. The mechanism was IDO1-dependent, with TA1 promoting IDO1 expression specifically in colon tissue, increasing the kynurenine-to-tryptophan ratio, and expanding Foxp3+ regulatory T-cells in mesenteric lymph nodes [9].
Critically, this same study showed context-dependent behavior: TA1 induced IDO1-dependent tolerance in gut tissue but preserved aggressive immune surveillance in tumor tissue, where it increased CD8+ T-cell infiltration and decreased Tregs [9]. A patent (US20100004174A1) claimed TA1 for prevention and treatment of Crohn's disease and ulcerative colitis but was later abandoned, likely reflecting commercial rather than scientific considerations.
Limitation: All gut-specific evidence originates from a single research group (Romani, Garaci, and colleagues at the University of Perugia). While this group is the leading authority on TA1 research, the absence of independent replication is a meaningful limitation.
Additional Research Areas
The Basics
TA1 research extends into several additional areas including nerve growth promotion, antifungal immune support, blood pressure modulation via ACE inhibition, inflammatory pain reduction, and cystic fibrosis. These areas are at earlier stages of investigation with varying levels of evidence.
The Science
Neurodevelopment: Wang et al. (2017) demonstrated that TA1 promotes neurogenesis and cognition in developing mice through systemic Th1 bias, with 4-week-old mice showing improved maze-learning performance [20].
Antifungal Immunity: Romani et al. (2004) showed TA1 activates dendritic cells for antifungal Th1 resistance through Toll-like receptor signaling, with demonstrated efficacy in Aspergillus infection models [21].
ACE Inhibition: Kharazmi-Khorassani et al. (2019) identified ACE-inhibitory and antioxidant activity in TA1, suggesting potential cardiovascular applications [22].
Inflammatory Pain: Xu et al. (2019) demonstrated that TA1 inhibits CFA-induced pain and microglia-mediated pro-inflammatory cytokine production in spinal cord, acting directly at inflammation sites through a mechanism distinct from conventional analgesics [23].
Cystic Fibrosis: Romani et al. (2017) showed TA1 can reduce inflammation and improve CFTR protein function in CF models, representing a potential single-molecule therapeutic approach [24].
Autoimmune Depletion: Pica et al. (2016) found significantly depleted serum TA1 levels in patients with chronic inflammatory autoimmune diseases (median 18.38 ng/ml vs. 53.08 ng/ml in healthy controls, p<0.0001), with psoriatic arthritis patients showing the most severe depletion at 6.93 ng/ml [25].
Antidepressant Effect: Aynekulu Mersha et al. (2025) reported an antidepressive effect of thymosin alpha-1 in a small open-label proof-of-concept study in common variable immune deficiency patients with depression [26].
Biomarker Evidence Matrix
Category
Immune Function
- Evidence Strength
- 9/10
- Reported Effectiveness
- 8/10
- Summary
- Strongest evidence base. Multiple RCTs in hepatitis, sepsis, COVID-19. Approved in 35+ countries. Community reports consistently positive for immune resilience.
Category
Inflammation
- Evidence Strength
- 7/10
- Reported Effectiveness
- 7/10
- Summary
- Selective cytokine modulation (IL-6, TNF-alpha reduction) documented in clinical studies. Community reports reduced inflammatory markers.
Category
Energy Levels
- Evidence Strength
- 4/10
- Reported Effectiveness
- 7/10
- Summary
- No direct clinical energy studies, but community reports from Long COVID and chronic illness populations report significant energy restoration.
Category
Focus & Mental Clarity
- Evidence Strength
- 3/10
- Reported Effectiveness
- 6/10
- Summary
- Preclinical neurodevelopment data only. Community reports of brain fog clearance, primarily in Long COVID context.
Category
Mood & Wellbeing
- Evidence Strength
- 3/10
- Reported Effectiveness
- 6/10
- Summary
- One small open-label proof-of-concept study showing antidepressive effects in CVID patients [26]. Community reports general wellbeing improvement.
Category
Pain Management
- Evidence Strength
- 4/10
- Reported Effectiveness
- 5/10
- Summary
- Animal data showing direct anti-inflammatory pain mechanism [23]. Limited community reports.
Category
Gut Health
- Evidence Strength
- 5/10
- Reported Effectiveness
- 5/10
- Summary
- Compelling preclinical colitis data from single research group [9]. No human IBD trials. No substantial community gut-specific reports.
Category
Recovery & Healing
- Evidence Strength
- 3/10
- Reported Effectiveness
- 5/10
- Summary
- Limited direct evidence; primarily theoretical based on immune support mechanism.
Category
Sleep Quality
- Evidence Strength
- 2/10
- Reported Effectiveness
- 5/10
- Summary
- No direct clinical data. Anecdotal community reports of improved sleep, likely secondary to reduced fatigue.
Category
Longevity & Neuroprotection
- Evidence Strength
- 4/10
- Reported Effectiveness
- 6/10
- Summary
- Preclinical neurodevelopment data. Thymic restoration mechanism has theoretical longevity implications. Practitioner protocols include longevity as use case.
Category
Daily Functioning
- Evidence Strength
- 3/10
- Reported Effectiveness
- 7/10
- Summary
- No formal clinical trials measuring daily functioning. Strong community reports from severely immunocompromised populations.
Category
Hair Health
- Evidence Strength
- 1/10
- Reported Effectiveness
- 4/10
- Summary
- Single anecdotal report of hair regrowth during Long COVID treatment. No clinical evidence.
Category
Blood Pressure
- Evidence Strength
- 3/10
- Reported Effectiveness
- 4/10
- Summary
- Preclinical ACE inhibition data [22]. No community-reported outcomes.
Category
Side Effect Burden
- Evidence Strength
- 8/10
- Reported Effectiveness
- 7/10
- Summary
- Excellent safety profile across 11,000+ study subjects. Community reports confirm tolerability. Mild injection site reactions and transient flu-like symptoms are the most common effects.
Benefits & Potential Effects
The Basics
The primary benefit of TA1 is better-calibrated immune function. Rather than simply amplifying immune activity (which can cause problems), TA1 helps the immune system make smarter decisions about what to attack and what to leave alone. People most likely to notice benefits are those with compromised immune function: frequent infections, slow recovery from illness, poor vaccine responses, or immune challenges associated with aging.
Community members consistently report improved immune resilience (fewer colds, faster recovery), increased energy levels (particularly those with chronic fatigue conditions), and reduced brain fog. Some users describe the effect as getting a "software update" for their immune system rather than a hardware upgrade.
An important pattern in community reports: benefits tend to require ongoing administration. Multiple independent users note that improvements do not persist after discontinuing TA1. This is consistent with TA1's mechanism as an immune modulator rather than a curative agent. It maintains improved immune function while present but does not permanently reprogram the immune system.
The Science
TA1's documented benefits are downstream consequences of Treg expansion, selective cytokine rebalancing, and IDO1 activation [2][5][9]:
Immune Modulation Without Suppression. TA1 rebalances immune populations toward measured response while preserving pathogen-fighting capacity. IFN-gamma production, NK cell activity, and MHC class I presentation remain intact or are enhanced, while autoimmune-driving pathways (excessive Th17, elevated IL-6) are dampened [2][5].
Antiviral Defense Enhancement. TA1 increases interferon-gamma production, activates NK cells, enhances macrophage phagocytosis, and increases MHC class I presentation for improved identification and elimination of virus-infected cells [2][8].
Selective Anti-Inflammatory Effects. TA1 reduces IL-6 and TNF-alpha while preserving or increasing IL-10. This selectivity pattern overlaps functionally with NAD+ precursors, which achieve similar downstream modulation through a different pathway [2][5].
Oxidative Stress Protection. TA1 amplifies the activity of endogenous antioxidant enzymes including catalase, superoxide dismutase (SOD), and glutathione peroxidase (GPx) [2].
Vaccine Response Enhancement. TA1 has been studied for improving vaccine immunogenicity, particularly in elderly and immunocompromised populations who typically mount suboptimal responses. Gravenstein et al. (1989) demonstrated augmentation of influenza antibody response in elderly men [27].
Reading about potential benefits is the starting point. Knowing whether you're actually experiencing them is where real value begins. Doserly lets you track the specific health markers that matter for your protocol, from body composition and energy levels to sleep quality, mood, and recovery time, building a personal dataset that goes beyond subjective impressions.
The app's proactive monitoring doesn't wait for you to notice a problem. It surfaces patterns in your logged data that might suggest suboptimal timing, flags potential interactions with other items in your health stack, and helps you identify which benefits are tracking with what the research suggests and which aren't materializing. Think of it as a second set of eyes on your protocol, always watching the trends.
Capture changes while they are still fresh.
Log symptoms, energy, sleep, mood, and other observations alongside protocol events so patterns do not live only in memory.
Trend view
Symptom timeline

Symptom tracking is informational and should be interpreted with a qualified clinician.
Side Effects & Safety Considerations
The Basics
TA1 has one of the most reassuring safety profiles among research peptides, backed by decades of clinical use across more than 11,000 study subjects. The most common side effects are mild and predictable: redness or soreness at the injection site, and occasional flu-like symptoms (low-grade fever, mild fatigue) that typically resolve within hours.
The flu-like response, particularly after early doses, is worth understanding rather than fearing. Community members and practitioners describe it as an "immune activation wave," where the immune system generates temporary noise as it recalibrates. This typically fades by the first or second dose and is generally considered a sign that the immune system is responding rather than a reason for concern.
The most important safety consideration involves autoimmune conditions. Because TA1 modulates immune activity, it can potentially trigger flares in people with active autoimmune diseases. One community report described significant worsening of MCAS (mast cell activation syndrome) symptoms. Practitioners recommend conservative dosing and close monitoring for anyone with autoimmune history, with immediate discontinuation if symptoms worsen.
TA1 should not be used by organ transplant recipients on immunosuppression, as its immunomodulatory activity could conflict with anti-rejection medications. Pregnancy and breastfeeding are also contraindications due to lack of safety data.
The Science
Safety data across clinical programs demonstrates an excellent tolerability profile [1][4]:
Common effects (reported in clinical trials):
- Local injection-site reactions (redness, mild irritation)
- Transient fatigue or myalgia
- Low-grade fever, particularly during initial doses
Rare adverse effects:
- Headache
- Mild, transient transaminase elevation
No dose-limiting toxicity identified: Doses up to 16 mg subcutaneously over 12 months showed no significant TA1-specific toxicity [28]. Standard clinical doses of 1.6 mg twice weekly for 6-12 months have been well-tolerated across multiple trials [1][3].
Autoimmune considerations: Despite its immunomodulatory profile suggesting potential benefit in autoimmune conditions, TA1 can exacerbate autoimmune flares in predisposed individuals. Chronic overstimulation has not been observed, but prolonged use should be monitored for autoimmune exacerbation [14].
Contraindications:
- Known hypersensitivity to thymic peptides
- Organ transplant recipients on immunosuppressive regimens
- Active autoimmune disease flares (use with extreme caution; conservative dosing recommended)
- Pregnancy and breastfeeding (no safety data)
- Concurrent live vaccines
The side effects and contraindications above give you a map of what to watch for. Doserly turns that map into a daily practice. Log the specific biomarkers and symptoms associated with this compound's known risk profile, and the app builds a timeline of how your body is responding across your cycle.
Trending in the wrong direction on a key marker? Noticing a pattern that started two weeks into your protocol? Doserly connects the dots between your protocol timeline and your logged data, making it easier to spot emerging issues early and have informed, data-backed conversations with your healthcare provider about what's working and what needs attention.
Keep side effects, flags, and follow-up notes visible.
Doserly helps you document safety observations, side effects, medication changes, and follow-up questions so important context is not scattered.
Safety log
Flags and notes

Safety notes are not emergency guidance; seek medical help when appropriate.
Dosing Protocols
The Basics
TA1 dosing is one area where clinical trials and community practice diverge significantly. Three distinct approaches are commonly referenced, and there is no established consensus on which is optimal for general immune support:
The clinical standard, established through hepatitis and sepsis trials, is 1.6 mg administered subcutaneously twice per week (for example, Monday and Thursday). This is the most studied protocol, with decades of safety data behind it.
Community protocols typically use lower daily doses, most commonly 300-500 mcg once daily. The 500 mcg daily dose yields approximately 3.5 mg per week, which is comparable to the clinical standard of 3.2 mg per week (1.6 mg x 2), just distributed differently. Proponents of this approach suggest that more frequent, lower doses may provide more consistent immune signaling.
Practitioner protocols from peptide-focused clinicians commonly cite 1.5 mg two to three times per week, with a sensitive or low-BMI starting dose of 0.8 mg twice weekly. Some protocols include an "intensive start" of 1.5 mg three times per week for two weeks before transitioning to the standard twice-weekly schedule.
Cycle lengths reported in the literature range from 8 weeks to 24 weeks, with some clinical trials using continuous dosing for 6-12 months. Common community practice is 8-16 weeks on with a 2-4 week break.
The Science
Clinical trial protocols (Tier 1 evidence):
- Chronic hepatitis B: 1.6 mg SC twice weekly for 6-12 months, often combined with interferon-alpha [3][12]
- Hepatitis C (adjunct to IFN-alpha): 1.6 mg SC twice weekly for 6 months
- Sepsis: 1.6 mg SC twice daily for 5 days, then once daily [4]
- Cancer adjuvant: 1.6 mg SC twice weekly for up to 12 months [15]
- COVID-19: 1.6 mg SC twice daily for 5 days in acute illness [18]
Community/practitioner protocols (Tier 3 evidence):
- Standard daily: 300-500 mcg SC once daily, 8-12 weeks [10]
- Clinical-standard biweekly: 1.5-1.6 mg SC twice weekly, 8-24 weeks
- Intensive start: 1.5 mg SC three times per week for 2 weeks, then twice weekly
- Sensitive start: 0.8 mg SC twice weekly
- Longevity maintenance: 500 mcg daily
Dose range in literature: 0.8-6.4 mg SC per administration, with 1.6 mg being the most commonly studied single dose [1].
Monitoring parameters suggested by practitioners:
- CBC with differential (absolute lymphocytes, neutrophils, NLR)
- hs-CRP
- Vitamin D, B12/folate, ferritin
- Zinc/copper
- Thyroid panel
- Timeline: baseline, 6-8 weeks, 12-16 weeks
Consistency is the difference between a protocol that delivers results and one that wastes time and money. Doserly was built for exactly this: keeping you on track with the precision your protocol demands.
The built-in calculators handle the math you shouldn't be doing in your head. The reconstitution calculator tells you exactly how much bacteriostatic water to add for your target concentration. The dose calculator converts between units, milligrams, and syringe markings so you draw the right amount every time. The injection site heat map tracks where you've administered and when, helping you rotate sites systematically to reduce tissue damage, scarring, and absorption inconsistencies from overusing the same area. Pair that with smart reminders tuned to your protocol's timing requirements, and you build the kind of daily consistency that separates optimized protocols from haphazard ones.
Turn symptom and safety notes into a clearer timeline.
Doserly helps you log doses, symptoms, and safety observations side by side so patterns are easier to discuss with a qualified clinician.
Pattern view
Logs and observations

Pattern visibility is informational and should be reviewed with a clinician.
What to Expect
Week 1-2: Some users report a transient flu-like response after the first few doses: mild fever, fatigue, or cold-like symptoms lasting hours to a few days. This "immune activation wave" is commonly reported and generally resolves after the first or second dose. Energy improvements may begin to appear by the end of week 2 in some individuals, particularly those with significant immune compromise.
Week 2-4: Immune marker shifts begin to appear in bloodwork (improved lymphocyte counts, better CD4/CD8 ratios). Some community members report noticeable reductions in brain fog and improved energy. Those with chronic fatigue conditions may notice the most dramatic changes during this period.
Week 4-8: Clinical benefits build over the full treatment course. Community reports suggest this is when immune resilience becomes most apparent: fewer infections, faster recovery from minor illness, and stabilization of energy levels. Inflammatory markers may begin to normalize.
Week 8-16+: With continued administration, overall immune competence typically improves. Better responses to vaccines and infections are reported. Some users describe a cumulative sense of improved wellbeing and reduced susceptibility to seasonal illness.
On discontinuation: Multiple community members independently report that benefits do not persist indefinitely after stopping TA1. The immune modulation appears to require ongoing administration to maintain, with most reporting gradual return to baseline within weeks of discontinuation.
Interaction Compatibility
Good With (Reported Synergistic)
- KPV — KPV blocks NF-kB directly for targeted anti-inflammatory action, complementing TA1's Treg expansion. Frequently paired in immune protocols.
- VIP — VIP orchestrates broad immune tolerance across multiple tissue types, working through a different pathway than TA1's dendritic cell education mechanism.
- BPC-157 — BPC-157 promotes gut tissue repair through angiogenesis, complementing TA1's immune modulation for gut-immune axis support.
- Glutathione — Immune cells cannot multiply effectively without adequate antioxidant capacity. TA1's immune expansion may stall if glutathione levels are depleted.
- NAD+ — NAD+ provides the metabolic foundation (cellular energy) that fuels TA1-driven immune cell expansion and function.
- Selank — Cortisol normalization supports the hormonal environment needed for optimal immune modulation.
- MOTS-C — Mitochondrial peptide that supports metabolic homeostasis, complementing TA1's immune effects in post-viral recovery protocols.
- Epithalon — Telomerase activator paired with TA1 for "healthy aging / thymic drift" protocols targeting immune senescence.
- SS-31 — Mitochondrial-targeted peptide for cellular energy optimization, often included in comprehensive immune recovery stacks.
- Pinealon — Neurological bioregulator included in some practitioner immune support protocols.
- GHK-Cu — Copper peptide for tissue regeneration, sometimes combined in comprehensive healing protocols.
- TB-500 — Tissue repair peptide. One community report noted TB-500 helped with cardiovascular symptoms and exercise recovery alongside TA1 for immune support.
Not Good With (Contraindicated or Caution)
- Immunosuppressive drugs (corticosteroids, biologics, anti-rejection medications) — TA1's immunomodulatory activity could conflict with immunosuppressive regimens. Organ transplant recipients should not use TA1.
- Live vaccines — TA1's immune activation could theoretically amplify live vaccine responses unpredictably. Inactivated vaccines are compatible and may benefit from TA1's adjuvant effect.
Administration Guide
Materials required:
- Thymosin Alpha-1 lyophilized vial (commonly available in 5 mg and 10 mg vials)
- Bacteriostatic water for reconstitution
- U-100 insulin syringes (29-31G, 1/2 inch)
- Alcohol swabs
- Sharps container
Recommended reconstitution solution: Bacteriostatic water (0.9% benzyl alcohol preserved). For a 5 mg vial, reconstitution with 3.0 mL yields approximately 1.67 mg/mL. For a 10 mg vial, 3.0 mL yields approximately 3.33 mg/mL. Use the reconstitution calculator for precise measurements at your target concentration.
Timing considerations: Morning or early afternoon administration is commonly preferred by practitioners and community members. There are no strict fasting requirements. TA1 can be administered at any consistent time; consistency matters more than the specific time of day.
Post-administration care: Monitor for injection site reactions (redness, mild irritation), which are the most common side effect. During the first 1-2 doses, be aware of possible transient flu-like symptoms (mild fever, fatigue) which typically resolve within hours. If significant fever, rash, unusual bruising, chest pain, or new neurological symptoms occur, discontinue and seek medical attention.
Supplies & Planning
Vial sizes commonly available:
- 5 mg lyophilized vials
- 10 mg lyophilized vials
General supplies:
- Bacteriostatic water (10 mL bottles)
- U-100 insulin syringes (29-31G, 5/16 to 1/2 inch)
- Alcohol swabs (one for vial stopper, one for injection site per administration)
- Sharps container for needle disposal
Reconstitution solution volume depends on the target concentration, which in turn depends on the dosing protocol being followed. Use the reconstitution calculator to determine the appropriate bacteriostatic water volume for your specific vial size and target dose per injection.
Supply duration varies significantly based on protocol choice (daily vs. twice weekly) and dose amount. Consult with a healthcare provider regarding protocol selection and plan supplies accordingly.
Storage & Handling
Lyophilized (powder) form:
- Long-term: Store at -20C (-4F) or below. Stable for years under these conditions.
- Short-term: Refrigerate at 2-8C (35.6-46.4F) for weeks to months.
- TA1 is remarkably thermostable compared to most peptides, remaining structurally stable at elevated temperatures up to 80-90C. However, standard cold storage is still recommended for maintaining maximum potency.
- Keep in original sealed packaging with desiccant. Store in a dry, dark environment.
- Allow vials to reach room temperature before opening to prevent condensation.
Reconstituted (liquid) form:
- Refrigerate immediately at 2-8C (35.6-46.4F).
- Use within 7 days when reconstituted with bacteriostatic water.
- Do not freeze reconstituted solution.
- Inspect before each use; do not use if cloudy or discolored.
- Label vials with reconstitution date.
Handling best practices:
- Swab vial stopper with alcohol before each draw.
- Use sterile syringes for each administration.
- Protect from direct light exposure during storage.
Lifestyle Factors
The following lifestyle factors are commonly cited by practitioners and community sources as supporting TA1 protocol outcomes:
Nutrition: Maintain a diet rich in vitamins C and D, as both play established roles in immune function. Zinc (15-30 mg/day with 1-2 mg copper) is frequently recommended alongside TA1. Adequate protein intake (1.6-2.2 g/kg/day) supports the immune cell proliferation that TA1 promotes.
Sleep: Ensure 7-9 hours of quality sleep. The immune system enters its peak surveillance and repair phase during sleep, and this phase is influenced by TA1 signaling. Poor sleep directly impairs the immune function TA1 aims to optimize.
Exercise: Moderate physical activity supports healthy circulation and immune cell migration throughout the body. Practitioners note that TA1 may be particularly relevant during athlete deload and rebuild periods to reduce inflammatory drag and support training quality.
Avoid: Excessive alcohol consumption and smoking both impair immune responses and generate oxidative stress that can counteract TA1's effects. Processed foods contribute to systemic inflammation.
Monitoring: Practitioners recommend a simple symptom scorecard tracking infections, days to recovery, energy, brain fog, sleep quality, training capacity, and side effects. Core labs at baseline, 6-8 weeks, and 12-16 weeks provide objective markers of immune function changes.
Regulatory Status & Research Classification
United States (FDA):
TA1 is not FDA-approved for general therapeutic use. It has received orphan drug designation for specific conditions (melanoma, hepatitis, DiGeorge syndrome). Access has historically been through compounding pharmacies, with over 370,795 prescriptions dispensed through this channel. In September 2024, TA1 was removed from the FDA's Category 2 bulk drug substance list after the original nominator withdrew their nomination. In December 2024, the Pharmacy Compounding Advisory Committee (PCAC) reviewed both thymosin alpha-1 acetate and free base forms. Current access depends on the FDA's final ruling regarding compounding eligibility.
International Approvals:
Thymalfasin (Zadaxin) is approved as a licensed pharmaceutical product in more than 35 countries including Italy, Singapore, and China, primarily for treatment of chronic hepatitis B. This represents one of the most extensive international approval records among peptides commonly discussed in research contexts.
Canada (Health Canada): No DIN or NPN approval identified.
United Kingdom (MHRA): No marketing authorization identified.
Australia (TGA): Not scheduled for general therapeutic use.
European Union (EMA): No centralized marketing authorization, though individual EU member states (notably Italy) have national approvals.
WADA Status: Not currently listed on the WADA Prohibited List.
Active Clinical Trials:
- NCT04487444: Thymalfasin (Thymosin Alpha 1) to Treat COVID-19 Infection
- NSCLC study: SBRT combined with rhGM-CSF and Thymosin Alpha 1 for stage IV NSCLC patients
Regulatory status changes frequently. Always verify the current legal status of any compound in your specific country or jurisdiction before making any decisions.
FAQ
What is Thymosin Alpha-1?
Thymosin Alpha-1 is a 28-amino acid peptide originally produced by the thymus gland. Its synthetic version, thymalfasin (brand name Zadaxin), is approved in more than 35 countries as an immune modulator for conditions including chronic hepatitis B and C. It has been studied in over 30 clinical trials involving more than 11,000 subjects.
Is Thymosin Alpha-1 FDA-approved?
TA1 is not FDA-approved for general use in the United States, though it has received orphan drug designation for specific conditions. It is approved in 35+ countries internationally. US access has historically been through compounding pharmacies, but the regulatory landscape is under review following 2024 PCAC proceedings.
What are the most common side effects?
Based on available clinical data across 11,000+ study subjects, the most commonly reported side effects are mild injection-site reactions (redness, soreness) and occasional transient flu-like symptoms. No major safety signals have been identified in published trials. The principal contraindication noted in reviews is use in organ transplant recipients.
How does Thymosin Alpha-1 differ from other immune-modulating peptides?
Based on available research, TA1 operates through regulatory T-cell expansion and the IDO1 tolerance pathway, which is mechanistically distinct from KPV (which blocks NF-kB directly) and BPC-157 (which promotes tissue repair through angiogenesis). TA1 works upstream of both by expanding the regulatory cells that govern immune decision-making.
How long does it take to see effects?
Community reports suggest immune marker shifts may appear within 2-4 weeks, with clinical benefits building over the full treatment course. Some users report energy improvements within the first two weeks, while others require 4-8 weeks. The timeline varies based on baseline immune status and the specific condition being addressed.
Do the effects last after stopping?
Based on community reports, benefits generally require ongoing administration. Multiple independent users note that improvements do not persist indefinitely after discontinuation, with gradual return to baseline within weeks of stopping.
Is Thymosin Alpha-1 safe with autoimmune conditions?
This is an area requiring particular caution. While TA1's mechanism (Treg expansion) theoretically supports autoimmune rebalancing, it can also trigger flares in predisposed individuals. Practitioners recommend conservative dosing (starting at 0.8 mg twice weekly), close monitoring, and immediate discontinuation if symptoms worsen. Always discuss with a healthcare provider who understands your specific autoimmune history.
What is the difference between Thymosin Alpha-1 and Thymosin Beta-4 (TB-500)?
Despite sharing the "thymosin" name, these are completely different peptides with different mechanisms. TA1 is a 28-amino acid immune modulator working through T-cell maturation and TLR signaling. TB-500/Thymosin Beta-4 is a 43-amino acid tissue repair peptide working through actin sequestration and cell migration. They address different systems (immune function vs. tissue repair) and can be used together.
Sources & References
[1] Garaci E et al. "Thymosin alpha1: from bench to bedside." Int Immunopharmacol. 2012. PMID: 22546505
[2] Dominari A et al. "Thymosin alpha 1: A comprehensive review of the literature." World J Virol. 2020. PMID: 33362999
[3] Yang Y et al. "Thymalfasin therapy in treating chronic hepatitis B patients: a meta-analysis." J Viral Hepat. 2013. PMID: 23458517
[4] Pei F, Guan X, Wu J. "Thymosin alpha 1 treatment for patients with sepsis." Expert Opin Biol Ther. 2018. PMID: 30063866
[5] Li J et al. "Thymosin alpha 1 suppresses Th17 cell responses and promotes regulatory T cells in rheumatoid arthritis." Int Immunopharmacol. 2014. PMID: 25261745
[6] Yang X et al. "Effect of thymosin alpha-1 on subpopulations of Th1, Th2, Th17, and regulatory T cells (Tregs) in vitro." Braz J Med Biol Res. 2012;45(1):25-32.
[7] Romani L et al. "Thymosin alpha1 activates dendritic cell tryptophan catabolism and establishes a regulatory environment." Blood. 2007. PMID: 17332247
[8] King R, Tuthill C. "Immune Modulation with Thymosin Alpha 1 Treatment." Vitam Horm. 2016;102:151-178. PMID: 27450734
[9] Renga G et al. "Thymosin alpha1 protects from CTLA-4 intestinal immunopathology." Life Sci Alliance. 2020. PMID: 32817121
[10] Annals of the New York Academy of Sciences. "Thymosin Alpha-1: biological activities, clinical applications, and pharmacokinetics review."
[11] Shen X et al. "Generation of a novel long-acting thymosin alpha1-Fc fusion protein and its efficacy for the inhibition of breast cancer in vivo." Biomed Pharmacother. 2018;108:610-617.
[12] Liu Y et al. "Therapeutic effectiveness of thymosin alpha1 combined with pegylated interferon alpha in chronic hepatitis B: meta-analysis." J Immunol Res. 2020. PMID: 32908936
[13] You J, Zhuang L, Cheng HY et al. "Thymalfasin for chronic hepatitis B: A meta-analysis." J Viral Hepat. 2006. PMID: 16970600
[14] Matteucci C et al. "Thymosin alpha 1 and HIV-1: recent advances and future perspectives." Future Microbiol. 2017;12:141-155.
[15] Maio M et al. "Large randomized study of thymosin alpha 1, interferon alfa, or both in combination with dacarbazine in patients with metastatic melanoma." J Clin Oncol. 2010;28(10):1780-1787.
[16] Costantini C et al. "A Reappraisal of Thymosin Alpha1 in Cancer Therapy." Front Oncol. 2019. DOI: 10.3389/fonc.2019.00873
[17] Wei YT et al. "Thymosin alpha-1 Reverses M2 Polarization of Tumor-Associated Macrophages during Efferocytosis." 2022.
[18] Soeroto AY et al. "Meta-analysis of thymosin alpha-1 in COVID-19: significant mortality reduction in moderate-to-critical patients." Inflammopharmacology. 2023.
[19] University of Rome "Tor Vergata" open study. PASC patients showing persistent naive B/T cell depletion; TA1 improved immune restoration.
[20] Wang G et al. "Immunopotentiator Thymosin Alpha-1 Promotes Neurogenesis and Cognition in the Developing Mouse via a Systemic Th1 Bias." Neurosci Bull. 2017;33(6):675-684.
[21] Romani L et al. "Thymosin alpha1 activates dendritic cells for antifungal Th1 resistance through Toll-like receptor signaling." Blood. 2004;103(11):4232-4239.
[22] Kharazmi-Khorassani J, Asoodeh A. "Antioxidant and angiotensin-converting enzyme (ACE) inhibitory activity of thymosin alpha-1." Bioorganic Chem. 2019;87:743-752.
[23] Xu Y et al. "Thymosin Alpha-1 Inhibits Complete Freund's Adjuvant-Induced Pain and Production of Microglia-Mediated Pro-inflammatory Cytokines in Spinal Cord." Neurosci Bull. 2019.
[24] Romani L et al. "Thymosin alpha1 represents a potential potent single-molecule-based therapy for cystic fibrosis." Nat Med. 2017;23(5):590-600.
[25] Pica F et al. "Serum thymosin alpha 1 levels in patients with chronic inflammatory autoimmune diseases." Clin Exp Immunol. 2016;186(1):39-45. PMID: 27350088
[26] Aynekulu Mersha DG et al. "Indications for an antidepressive effect of thymosin alpha-1 in a small open-label proof of concept study in common variable immune deficiency patients with depression." Brain Behav Immun Health. 2025;43:100934. PMID: 39867848
[27] Gravenstein S et al. "Augmentation of influenza antibody response in elderly men by thymosin alpha one." J Am Geriatr Soc. 1989;37(1):1-8. PMID: 2642497
[28] FDA Peptide Advisory Committee (2024). Safety data: TA1 doses up to 16 mg SC for 12 months showed no significant toxicity.
[29] Severa M et al. "Thymosins in multiple sclerosis and its experimental models: moving from basic to clinical application." Mult Scler Relat Disord. 2019;27:52-60. PMID: 30317071
[30] Goldstein AL. "From lab to bedside: emerging clinical applications of thymosin alpha 1." Expert Opin Biol Ther. 2009;9(5):593-608.
[31] Tuthill C, Rios I et al. "Thymosin alpha 1: a comprehensive review of the literature." Expert Opin Biol Ther. 2010. PMID: 20696559
[32] Simonova MA et al. "Aging and Thymosin Alpha-1." 2025.
Related Peptide Guides
- KPV — Anti-inflammatory peptide that blocks NF-kB directly; frequently paired with TA1 in immune protocols
- VIP — Vasoactive intestinal peptide for broad immune tolerance; complements TA1's targeted Treg expansion
- BPC-157 — Tissue repair peptide; paired with TA1 for gut-immune axis support
- TB-500 — Thymosin Beta-4 fragment for tissue repair; different thymosin family member with distinct mechanism
- Glutathione — Essential antioxidant that supports TA1-driven immune cell expansion
- NAD+ — Cellular energy substrate that fuels immune cell proliferation
- Selank — Cortisol-modulating peptide for stress normalization alongside immune protocols
- MOTS-C — Mitochondrial peptide for metabolic support in recovery protocols
- Epithalon — Telomerase activator paired with TA1 in longevity/immune senescence protocols
- SS-31 — Mitochondrial-targeted peptide for cellular energy optimization
- Pinealon — Neurological bioregulator included in comprehensive immune support protocols
- GHK-Cu — Copper peptide for tissue regeneration in comprehensive healing stacks
- Humanin — Mitochondrial-derived peptide referenced in community recovery protocols
Need the reconstitution math for Thymosin Alpha-1: Complete Research Guide?
Open the calculator with Thymosin Alpha-1: Complete Research Guide prefilled to estimate concentration, draw volume, and related measurement math from the reconstitution details you already have.