VIP (Vasoactive Intestinal Peptide): Complete Research Guide
On this page
Quick Reference Card
Attribute
Also Known As
- Detail
- Vasoactive Intestinal Peptide, Vasoactive Intestinal Polypeptide, Aviptadil (synthetic form), VIP-28
Attribute
Administration
- Detail
- Intranasal spray (primary research route); subcutaneous injection; intravenous (clinical trial settings); inhaled/nebulized (clinical trial settings)
Attribute
Research Status
- Detail
- Research Compound. Not FDA-approved for any indication. Phase 2 and Phase 3 clinical trials completed for respiratory conditions. Aviptadil has been evaluated in multiple human trials.
Attribute
Typical Dose Range
- Detail
- Intranasal: 50-100 mcg per dose, 1-4x daily. Subcutaneous: 25-150 mcg, 1-2x daily. IV (clinical trials only): escalating infusions up to 6 mcg/kg/day.
Attribute
Half-Life
- Detail
- Approximately 1 minute (plasma). Biological effects persist longer than plasma clearance.
Attribute
Cycle Length
- Detail
- 2-12 weeks commonly reported; some CIRS protocols extend to 18 months.
Attribute
Storage
- Detail
- Lyophilized: -20C or below for long-term storage, 2-8C for short-term. Reconstituted: 2-8C, use promptly. Protect from light. VIP degrades rapidly at room temperature.
Overview / What Is VIP?
The Basics
VIP stands for Vasoactive Intestinal Peptide, though its name is misleading. Despite being discovered in the gut and initially studied for its blood vessel effects, VIP's most significant functions have nothing to do with either. It is better understood as an immune system coordinator that also supports gut barrier health and helps synchronize your body's internal clock.
Your body produces VIP naturally. It is a 28-amino acid neuropeptide found throughout your nervous system, immune tissues, and digestive tract. It belongs to the same family as other signaling molecules your brain and gut use to communicate with each other.
What makes VIP unique is how it handles immune responses. Rather than simply turning inflammation up or down, VIP teaches your immune system when to attack and when to stand down. It creates specialized immune cells called regulatory T-cells that act as peacekeepers, preventing your immune system from overreacting to harmless triggers while still allowing it to fight genuine threats.
VIP has more human clinical trial data than most research peptides. This includes a 471-patient Phase 3 trial, several Phase 2 studies, and large observational cohorts. It is primarily studied for pulmonary conditions, chronic inflammatory response syndrome (CIRS), and immune dysregulation. Its plasma half-life of roughly one minute makes delivery route selection critically important, and much of the research story around VIP involves understanding why certain delivery methods work while others do not.
The Science
Vasoactive Intestinal Peptide (VIP) is a 28-amino acid neuropeptide of the secretin-glucagon superfamily, first isolated from porcine intestinal extracts in 1970 [1]. VIP functions as a neurotransmitter, neuromodulator, and immunomodulator through two class B G-protein coupled receptors: VPAC1 and VPAC2 [2][3].
VIP is endogenously expressed throughout the central nervous system, the enteric nervous system (the largest source of VIP in the body), thymic tissue, lung parenchyma, and immune organs [2]. The peptide's widespread distribution reflects its pleiotropic signaling roles, extending far beyond the vasodilatory and intestinal secretory functions implied by its name.
The synthetic pharmaceutical form, aviptadil, has been evaluated in multiple clinical contexts including COVID-19-associated respiratory failure (Phase 3, n=471; Phase 2b/3, n=196; Phase 2 RCT, n=80), pulmonary sarcoidosis (Phase 2, n=20), and pulmonary arterial hypertension (n=20) [4][5][6][7]. A long-acting VIP analog (pemziviptadil) is under investigation for cardiopulmonary disease using once-weekly subcutaneous dosing [8].
VIP shares structural homology with PACAP (pituitary adenylate cyclase-activating peptide), reflecting deep evolutionary conservation of this signaling architecture within the secretin-glucagon superfamily [2].
Molecular Identity
Attribute
Common Names
- Detail
- VIP, Vasoactive Intestinal Peptide, Vasoactive Intestinal Polypeptide, Aviptadil (synthetic)
Attribute
Amino Acid Sequence
- Detail
- His-Ser-Asp-Ala-Val-Phe-Thr-Asp-Asn-Tyr-Thr-Arg-Leu-Arg-Lys-Gln-Met-Ala-Val-Lys-Lys-Tyr-Leu-Asn-Ser-Ile-Leu-Asn-NH2
Attribute
Sequence Length
- Detail
- 28 amino acids
Attribute
Molecular Formula
- Detail
- C147H237N43O43S
Attribute
Molecular Weight
- Detail
- 3,326 Da
Attribute
Structural Type
- Detail
- Linear peptide with C-terminal amidation
Attribute
Functional Class
- Detail
- Neuropeptide, immunomodulator, vasodilator, neurotransmitter
Attribute
Receptor Targets
- Detail
- VPAC1, VPAC2 (class B GPCRs)
Attribute
Superfamily
- Detail
- Secretin-glucagon superfamily
Mechanism of Action
The Basics
VIP works through two different receptors on your immune cells, called VPAC1 and VPAC2. What makes VIP special is that these receptors switch roles depending on what your immune system is doing at the time.
When your immune system is at rest, VPAC1 is the dominant receptor. VIP binding to VPAC1 acts like a fire extinguisher, dampening acute inflammatory responses by reducing the production of inflammatory signaling molecules.
When your immune cells become activated (because they have detected a threat or are in the middle of an immune response), something remarkable happens. VPAC1 expression drops and VPAC2 expression rises. This "receptor switching" changes VIP's job entirely. Now, instead of just putting out inflammatory fires, VIP begins programming the immune system for long-term tolerance. It generates regulatory T-cells that help prevent the immune system from overreacting in the future.
Think of the difference this way: VPAC1 puts out the fire; VPAC2 redesigns the building so it does not catch fire again. This two-phase response is why researchers describe VIP as an immune tolerance orchestrator rather than simply an anti-inflammatory compound.
VIP also plays a critical role in gut health. It helps maintain the integrity of your intestinal lining, supports the mucus layer that protects it, and influences the composition of your gut microbiome. In the brain, VIP-expressing neurons in the suprachiasmatic nucleus (your body's master clock) help synchronize your daily rhythms.
The Science
VIP exerts its immunomodulatory effects through differential receptor engagement:
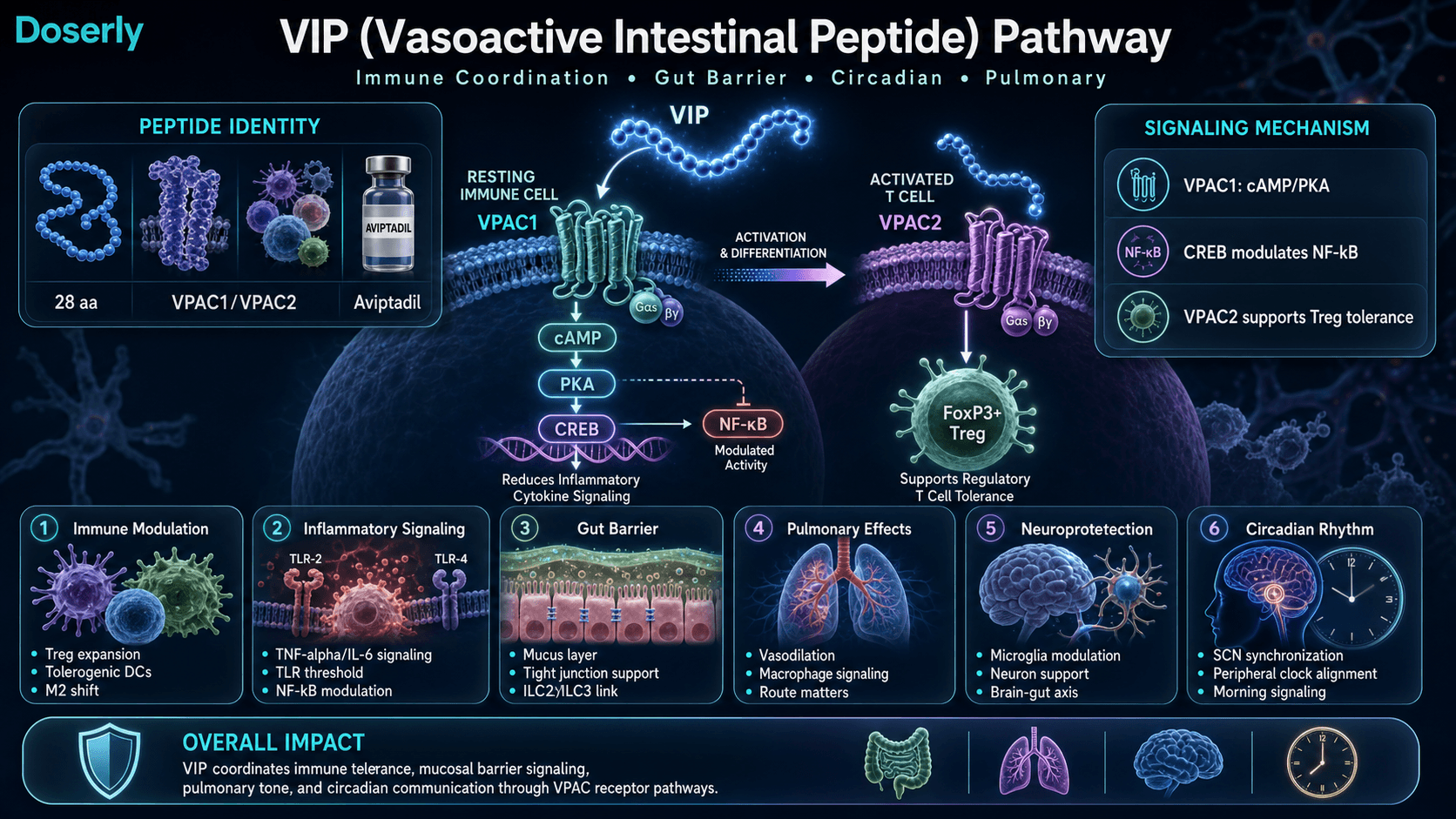
VPAC1 Signaling (Acute Anti-Inflammatory Phase). VPAC1 is constitutively expressed on resting T cells, monocytes, and neutrophils. VIP binding activates the cAMP/PKA signaling cascade, driving CREB to compete with NF-kB for the shared transcriptional coactivator CBP while simultaneously stabilizing cytoplasmic IkB/NF-kB complexes to prevent nuclear translocation [3]. This suppresses pro-inflammatory cytokine output including TNF-alpha, IL-6, and IL-12.
VPAC2 Signaling (Tolerance Programming Phase). Upon T cell activation, VPAC1 expression downregulates while VPAC2 expression upregulates, a receptor switching mechanism documented by Juarranz et al. (2019) [9]. VPAC2 on activated T cells drives expansion and maintenance of CD4+CD25+FoxP3+ regulatory T cells. VPAC2-knockout mice develop exacerbated experimental autoimmune encephalomyelitis with strikingly reduced Treg abundance and impaired suppressive function [10]. Human mast cells express only VPAC2, while resting monocytes and neutrophils express only VPAC1, enabling context-dependent signaling calibrated to each immune cell population's activation state [2].
Tolerogenic Dendritic Cell Generation. VIP generates tolerogenic dendritic cells characterized by low costimulatory molecule expression (CD40, CD80, CD86), reduced pro-inflammatory cytokine output, and elevated IL-10 production. These tolerogenic DCs induce both CD4+ and CD8+ regulatory T cells with a distinctive CD28-negative/CTLA4-positive phenotype [11][12].
Macrophage Polarization. VIP biases macrophage differentiation from the classically activated M1 phenotype (high TNF-alpha, IL-1beta, IL-12, ROS) toward the alternatively activated M2 phenotype associated with tissue repair and resolution of inflammation [3].
TLR Downregulation. VIP reduces expression of toll-like receptors TLR-2 and TLR-4 through inhibition of the PU.1 transcription factor, raising the activation threshold at mucosal surfaces where the immune system must tolerate commensal organisms [3].
Gut-Brain-Immune Axis. VIP-deficient mice develop distorted crypt architecture, reduced goblet cell numbers, altered Firmicutes-to-Bacteroidetes ratios, and increased intestinal permeability [13]. Enteric neuron VIP release in response to feeding activates innate lymphoid cells (ILC2 and ILC3), coupling nutritional status directly to mucosal immune surveillance [14].
Circadian Synchronization. VIP functions as the primary synchronizing neuropeptide in the suprachiasmatic nucleus (SCN), coordinating firing patterns across SCN cell populations and aligning peripheral tissue clocks with the central light-dark cycle [2].
Pathway Visualization
Pharmacokinetics
The Basics
VIP has one of the shortest half-lives of any research peptide: roughly one minute in your bloodstream. That means after you administer it, the peptide itself is broken down almost immediately by enzymes in your blood. This does not mean the effects are equally brief. VIP triggers changes in immune cell populations, gene expression, and inflammatory signaling that persist well after the molecule itself has been cleared.
This ultrashort plasma life creates a critical delivery challenge. Intravenous VIP was used in the largest clinical trial (471 patients) and the trial was stopped for futility. Meanwhile, inhaled VIP in a smaller trial showed clear positive results. The difference was not the molecule. It was the route. Intranasal and inhaled delivery concentrate VIP at the target tissues (lungs, CNS) and bypass the rapid plasma degradation that makes IV dosing pharmacokinetically impractical.
For research contexts, intranasal delivery is the most commonly reported route. It provides direct access to the central nervous system through olfactory and trigeminal nerve pathways. Subcutaneous injection is also studied, primarily for systemic immune effects with morning (AM) timing to align with the body's natural cortisol awakening response.
The Science
Plasma Half-Life. Free VIP has a plasma elimination half-life of approximately one minute, subject to rapid enzymatic degradation by dipeptidyl peptidase IV (DPP-IV), neutral endopeptidase, and aminopeptidases [2][4].
Route-Dependent Efficacy. The contrast between clinical trial outcomes across routes is the most instructive pharmacokinetic finding. The TESICO Phase 3 trial using IV aviptadil in critically ill patients was stopped for futility [4], while an 80-patient Phase 2 RCT of inhaled aviptadil significantly reduced hospital stay and improved oxygenation [5]. Intranasal delivery bypasses first-pass hepatic metabolism and concentrates the molecule at CNS-proximal tissue [7].
Subcutaneous Pharmacokinetics. Limited data exist for subcutaneous native VIP pharmacokinetics. Bioavailability is unknown for this route. Community-reported subcutaneous protocols (25-150 mcg) operate on empirical observation rather than established PK parameters. The long-acting VIP analog pemziviptadil achieves once-weekly subcutaneous dosing through structural modifications that resist enzymatic degradation [8].
Nanomedicine Advances. VIP-SSM (sterically stabilized phospholipid micelles) demonstrated superior efficacy at 0.25 nmol single doses compared to free peptide in colitis models while eliminating hypotensive toxicity [15]. Oral colonic capsule formulations have shown preclinical feasibility [16]. Neither is clinically available.
The half-life and clearance data above tells you how long the compound stays active, but what does that mean for your daily schedule? Doserly's pharmacokinetic tools let you plug in your dose and frequency to see a projected concentration timeline, helping you understand when you're at peak levels and when the compound has largely cleared.
This becomes especially useful when titrating. If you're increasing your dose gradually, the estimator shows how each step changes your projected peak and trough levels, giving you and your healthcare provider concrete data to discuss at check-ins rather than relying on subjective feel alone.
See how each compound fits into the whole protocol.
Doserly organizes compounds, supplements, peptides, medications, and hormone protocols together so overlapping routines are easier to understand.
Stack view
Connected protocol

Stack views improve organization; they do not determine compatibility.
Research & Clinical Evidence
VIP and Pulmonary Conditions
The Basics
VIP's strongest clinical evidence comes from lung-related conditions. In studies of pulmonary sarcoidosis (a chronic inflammatory lung disease), patients who received nebulized VIP for four weeks showed reduced inflammation and increased regulatory T-cell counts. For pulmonary hypertension (high blood pressure in the lungs), inhaled VIP reduced pressure in the lung arteries and improved heart output over three to six months of treatment.
The COVID-19 pandemic generated the largest VIP trials to date. Results were mixed, but the pattern was instructive. When VIP was given intravenously to critically ill patients, it did not outperform placebo. When it was inhaled directly into the lungs of moderately ill patients, it reduced hospital stays and improved breathing. The lesson was not that VIP does not work for lungs, but that delivery route matters enormously for a peptide that lasts only one minute in the blood.
The Science
Sarcoidosis (Phase II, n=20). Nebulized VIP over 4 weeks significantly reduced TNF-alpha production by bronchoalveolar lavage macrophages and increased CD4+CD25+FoxP3+ regulatory T cells, providing the first controlled human demonstration of VIP's immunoregulatory effect [6].
Pulmonary Arterial Hypertension (n=20). Inhaled VIP produced significant temporary pulmonary vasodilation and decreased right heart load without systemic side effects. Extended treatment over 3-6 months reduced mean pulmonary artery pressure from 59 to 46 mmHg and increased cardiac output [19].
COVID-19 ARDS. TESICO (NCT04843761, n=471): Phase 3 IV aviptadil, stopped for futility [4]. Phase 2b/3 (NCT04311697, n=196): primary endpoint not met, but pre-specified subgroup analysis showed statistically significant increase in 60-day survival (OR 2.0) with reduced IL-6 levels [4]. Phase 2 RCT (inhaled aviptadil, n=80): significantly reduced hospital stay (7.8 vs 10 days), improved blood oxygenation, and superior radiological scores vs placebo [5]. A case series of 6 patients with severe viral ARDS showed significant oxygenation improvement and radiological clearance within 3 days of IV aviptadil [4].
VIP and CIRS / Mold Illness
The Basics
Chronic Inflammatory Response Syndrome (CIRS) is a condition where the immune system becomes stuck in an overactive state, often triggered by exposure to mold or other biotoxins. VIP nasal spray is the final step in the Shoemaker CIRS protocol, used after the underlying inflammatory triggers have been addressed.
In a study of 20 CIRS patients treated with VIP nasal spray over 18 months, inflammatory markers normalized, brain imaging showed structural improvements, and regulatory T-cell counts increased. A larger dataset of over 10,000 patients has been reported with consistent findings, though this data comes from a single practitioner-researcher and has not been independently replicated in a randomized controlled trial.
The Science
An 18-month open-label trial administered VIP nasal spray to 20 CIRS patients refractory to other interventions. TGF-beta1, C4a, and MMP-9 normalized. NeuroQuant MRI demonstrated structural brain improvements. Regulatory T-cell levels increased [7]. A larger observational cohort exceeding 10,000 patients has been reported with consistent inflammatory marker normalization. The single-center, single-practitioner limitation is significant and must be acknowledged alongside the cohort size [7].
VIP and Gut Health
The Basics
VIP plays a natural role in maintaining your gut's protective barrier. In animal studies, mice engineered to lack VIP developed leaky gut, lost protective mucus-producing cells, and showed changes in their gut bacteria composition. When VIP was restored, these problems reversed.
A particularly interesting finding is that your gut releases VIP after meals. This feeding-triggered release activates immune cells in the gut lining that help defend against infections, directly linking what you eat to how well your gut defenses function.
No human clinical trials for VIP in inflammatory bowel disease have been completed, despite strong preclinical evidence. The main barrier is pharmacokinetic: VIP's rapid degradation and dose-limiting blood pressure effects make it difficult to deliver effective concentrations to the gut.
The Science
VIP-knockout mice demonstrate distorted crypt architecture, reduced goblet cell numbers, altered Firmicutes-to-Bacteroidetes ratios, reduced microbial biodiversity, and increased intestinal permeability [13]. Exogenous VIP rescues the phenotype.
In TNBS-induced colitis (Crohn's disease model), VIP reduced clinical severity, downregulated TNF-alpha and IL-6, and promoted epithelial repair [17][18]. Feeding-triggered VIP release from enteric neurons activates ILC2 and ILC3, increasing resistance to helminth and enterobacterial infection [14].
No human efficacy trials for VIP in IBD have been completed. The pharmacokinetic barrier (rapid degradation, dose-limiting hypotension) is fundamental. VIP-SSM nanomedicine showed superior efficacy at lower doses in preclinical colitis models while eliminating hypotensive toxicity [15].
VIP and Neuroprotection
The Basics
In animal models of Parkinson's disease, VIP and VIP-related compounds preserved nerve cells and reduced the brain inflammation that drives neurodegeneration. VIP's role as the master synchronizing signal for your body's internal clock also positions it as relevant to brain health more broadly, since circadian disruption is increasingly linked to neurodegenerative conditions.
The Science
In MPTP mouse models of Parkinson's disease, VIP and VIP-mimetics preserved dopaminergic neurons and inhibited microglial activation (reduced iNOS, IL-1beta, TNF-alpha) [2]. VIP's neuroprotective effects are mediated through both direct VPAC receptor activation on neurons and indirect reduction of neuroinflammatory signaling.
Gozes et al. (1996) demonstrated that intranasal administration of a fatty acid-conjugated VIP analog provided neuroprotective effects in Alzheimer's disease models [20]. Human circadian intervention trials with exogenous VIP have not been conducted.
Biomarker Evidence Matrix
The following table presents evidence-based scores for VIP's effects across relevant biomarker categories. Evidence Strength reflects the quality of published research. Reported Effectiveness reflects community-reported outcomes from the sentiment analysis.
Category
Inflammation
- Evidence Strength
- 7/10
- Reported Effectiveness
- 7/10
- Summary
- Phase 2 human data showing TNF-alpha reduction and inflammatory marker normalization. Consistent community reports of improvement in CIRS patients.
Category
Immune Function
- Evidence Strength
- 7/10
- Reported Effectiveness
- 6/10
- Summary
- Human trial demonstrated Treg expansion and tolerogenic DC generation. Community reports describe immune normalization in CIRS contexts.
Category
Gut Health
- Evidence Strength
- 6/10
- Reported Effectiveness
- 6/10
- Summary
- Strong preclinical evidence (knockout models, colitis models). No human IBD trials. Community reports describe calmer gut function.
Category
Focus & Mental Clarity
- Evidence Strength
- 5/10
- Reported Effectiveness
- 7/10
- Summary
- Limited formal evidence for cognitive effects, but NeuroQuant MRI data in CIRS cohort is notable. Brain fog clearing is the most consistent community-reported benefit.
Category
Energy Levels
- Evidence Strength
- 4/10
- Reported Effectiveness
- 6/10
- Summary
- No direct clinical evidence for energy effects. Community reports describe improved energy in CIRS and ME/CFS populations.
Category
Sleep Quality
- Evidence Strength
- 5/10
- Reported Effectiveness
- 5/10
- Summary
- Mechanistic basis through SCN synchronization is strong. Limited human data. Mixed community reports.
Category
Blood Pressure
- Evidence Strength
- 7/10
- Reported Effectiveness
- 5/10
- Summary
- Vasodilatory effects well-documented in clinical trials. Community reports note this as both beneficial and a side effect concern.
Category
Heart Health
- Evidence Strength
- 6/10
- Reported Effectiveness
- N/A
- Summary
- Cardioprotection demonstrated in preclinical ischemia-reperfusion models. Pulmonary hypertension trials showed improved hemodynamics. Community data not yet collected.
Category
Mood & Wellbeing
- Evidence Strength
- 3/10
- Reported Effectiveness
- 5/10
- Summary
- No direct clinical evidence. Community reports describe improved wellbeing as secondary benefit.
Category
Longevity & Neuroprotection
- Evidence Strength
- 5/10
- Reported Effectiveness
- 5/10
- Summary
- Preclinical neuroprotection data in Parkinson's models. SCN synchronization well-characterized. No human longevity-specific trials.
Category
Recovery & Healing
- Evidence Strength
- 4/10
- Reported Effectiveness
- 5/10
- Summary
- Preclinical evidence for tissue repair via M2 macrophage polarization. Limited community reports.
Category
Pain Management
- Evidence Strength
- 3/10
- Reported Effectiveness
- 5/10
- Summary
- No direct clinical pain studies. Community reports of migraine improvement in CIRS patients.
Category
Side Effect Burden
- Evidence Strength
- 6/10
- Reported Effectiveness
- 6/10
- Summary
- Safety data from multiple clinical trials. Generally well-tolerated at intranasal doses. Dose-limiting hypotension at higher systemic doses.
Category
Temperature Regulation
- Evidence Strength
- 5/10
- Reported Effectiveness
- 4/10
- Summary
- Flushing is the most commonly reported side effect, consistent with vasodilatory mechanism.
Benefits & Potential Effects
The Basics
VIP's potential benefits center on three interconnected systems: immune regulation, gut health, and circadian rhythm support.
For immune regulation, VIP does not simply suppress inflammation. It reprograms how your immune system responds to threats, shifting it toward more measured, tolerant responses. This makes it particularly interesting for conditions where the immune system is overactive or dysregulated, such as CIRS, autoimmune conditions, and chronic inflammation.
For gut health, VIP supports the integrity of your intestinal lining, promotes healthy mucus production, and may influence the composition of your gut bacteria. Since the gut contains the body's largest source of VIP-producing neurons, supplementation aims to restore a signaling environment that supports barrier function.
For circadian support, VIP is the master synchronizing signal in the brain's clock center. Consistent AM administration in research contexts reflects the goal of reinforcing the morning cortisol peak and the daily immune cycling pattern that VIP coordinates.
Community reports most frequently describe improvements in brain fog, energy, and overall inflammation, particularly among CIRS patients who have completed prior protocol steps.
The Science
VIP's benefit profile is mechanistically broad, spanning multiple organ systems through VPAC1/VPAC2 receptor engagement:
Immune Tolerance Reprogramming. VIP induces tolerogenic DCs, expands CD4+ and CD8+ Tregs, polarizes macrophages toward M2 repair phenotype, and downregulates TLR expression at mucosal surfaces [3][11][12]. This coordinated reprogramming distinguishes VIP from conventional anti-inflammatory agents.
Pulmonary Protection. Phase 2 data demonstrates pulmonary vasodilation, hemodynamic improvement, and anti-inflammatory effects in sarcoidosis and pulmonary hypertension models [6][19]. Inhaled aviptadil reduced hospital stay in COVID-19 patients [5].
Gut Barrier Maintenance. VIP maintains intestinal epithelial barrier integrity through tight junction assembly, mucus secretion stimulation, and innate lymphoid cell recruitment [13][14]. VIP deficiency in animal models produces phenotypic gut damage reversible with exogenous VIP.
Circadian Orchestration. VIP-expressing SCN neurons coordinate central and peripheral clock synchronization [2]. Circadian disruption is increasingly recognized as a driver of metabolic, immune, and neurodegenerative pathology.
Neuroprotection. VIP preserves dopaminergic neurons and inhibits microglial activation in preclinical Parkinson's models [2][20]. NeuroQuant MRI improvements in CIRS cohorts suggest potential structural brain benefits [7].
Side Effects & Safety Considerations
The Basics
VIP is generally considered well-tolerated at intranasal doses based on available clinical and community data. The most commonly reported side effect is mild, transient flushing (warmth and redness), which is consistent with VIP's natural blood vessel-relaxing activity. This typically resolves within minutes and often diminishes with continued use.
Other reported effects include lightheadedness, mild headache, and gastrointestinal looseness (looser stools). These are dose-dependent and generally manageable by reducing the dose or adjusting timing. Most practitioners recommend starting at the lowest effective dose and titrating slowly.
The primary safety concern is hypotension (low blood pressure). Individuals who are already prone to low blood pressure or who are taking blood pressure-lowering medications should exercise particular caution. Practitioners recommend monitoring blood pressure when starting VIP, especially during the first few doses. Using VIP seated or lying down during initial administration is a common precaution.
VIP should not be used after mid-afternoon (approximately 3 PM) due to mild stimulatory effects that could interfere with sleep. It is also important to note that VIP is contraindicated in the presence of many GI-related malignancies, as its vasodilatory and immunomodulatory effects could potentially interfere with cancer treatment.
The Science
Clinical Safety Data. The sarcoidosis Phase II trial reported no serious adverse events with nebulized VIP over 4 weeks [6]. The COVID-19 trials documented dose-limiting hypotension and tachycardia at higher IV doses, consistent with VIP's vasodilatory activity at supratherapeutic plasma concentrations [4]. No dependency or withdrawal phenomena have been reported across published datasets.
Dose-Dependent Vasodilation. Flushing, hypotension, and tachycardia are pharmacologically predicted consequences of VPAC receptor-mediated smooth muscle relaxation and vasodilation. These effects are dose-dependent, with intranasal doses (50-100 mcg) producing minimal systemic hemodynamic effects compared to IV administration [2][4].
Theoretical Immune Susceptibility. VIP's tolerance programming can theoretically increase susceptibility to intracellular pathogens. This has been documented in preclinical Salmonella models [3]. This is mechanistically consistent: a molecule that biases immune responses toward tolerance necessarily reduces some aspects of pathogen-directed immunity.
Contraindications. VIP is contraindicated in the setting of many GI-related malignancies. Evaluation by an oncologist is required to determine appropriateness in the context of any malignancy [8]. Individuals with migraine history or baseline hypotension should start at very low doses and avoid concurrent vasodilators (high-dose niacin, PDE-5 inhibitors) until individual response is established.
Side effect profiles are most useful when you can compare them against your own experience in real time. Doserly lets you log symptoms, severity, and timing alongside your dosing data, creating a side-by-side view of your protocol and your body's response.
This kind of systematic tracking catches things that memory alone misses. A subtle mood shift that began three days after a dose increase. Sleep disruption that correlates with evening administration. These patterns become visible when the data is laid out on a timeline, and they give your healthcare provider actionable information rather than vague concerns. Early detection of emerging side effects means earlier intervention.
Capture changes while they are still fresh.
Log symptoms, energy, sleep, mood, and other observations alongside protocol events so patterns do not live only in memory.
Trend view
Symptom timeline

Symptom tracking is informational and should be interpreted with a qualified clinician.
Dosing Protocols
The Basics
VIP dosing is complicated by two factors: the ultrashort half-life and the variety of delivery routes. There is no single established human dosing protocol for daily subcutaneous VIP, and the available data comes from different clinical contexts using different routes.
For intranasal use, commonly reported ranges are 50 to 100 mcg per dose, administered one to four times daily. Most practitioners recommend starting at the lower end and titrating up based on tolerance. In CIRS protocols, a common approach is 50 mcg per spray with four sprays (200 mcg total) three to four times daily, though this represents a single-practitioner protocol rather than a randomized trial dosage.
For subcutaneous use, community sources report ranges of 25 to 150 mcg, one to two times daily, with morning administration preferred to align with circadian rhythms. Some practitioners suggest a weight-based approach starting at approximately 1 mcg/kg per day.
Sources vary significantly on subcutaneous dosing because no evidence-based daily subcutaneous protocol exists in the peer-reviewed literature. The closest clinical evidence for subcutaneous administration uses a long-acting analog (pemziviptadil), dosed once weekly, not daily. All daily subcutaneous VIP protocols are therefore theoretical, extrapolated from IV trial exposure levels or based on empirical practitioner experience.
Cycle lengths typically range from 2 to 12 weeks, with a reassessment point at 4 weeks. Some CIRS protocols extend VIP use for many months, but these represent a specific disease context rather than a general recommendation. Most sources agree that indefinite use without a defined objective benefit endpoint is not advisable.
The Science
Intranasal Protocols. The CIRS protocol (Shoemaker) uses VIP nasal spray at 50 mcg per spray, with reported dosing of 4 sprays (200 mcg) 3-4 times daily [7]. The sarcoidosis Phase II trial used nebulized VIP for 4 weeks at protocol-specific doses [6]. Research contexts commonly report 50-100 mcg intranasal with gradual titration [2].
Subcutaneous Protocols (Theoretical). No human clinical literature establishes a daily subcutaneous regimen of native VIP for general outpatient use [8]. Weight-based extrapolation from IV aviptadil trial data suggests a starting dose of 1 mcg/kg SQ once daily (approximately 300 pmol/kg/day), representing roughly 50% of the lowest IV daily exposure, with a proposed ceiling of 3 mcg/kg/day (approximately 900 pmol/kg/day) [8].
IV Protocols (Clinical Trial Context). COVID-19 ARDS trials used escalating 12-hour IV infusions over 3 days at 600-1200-1800 pmol/kg, with the highest dose translating to approximately 6 mcg/kg/day [4][8].
Titration and Monitoring. All sources emphasize gradual titration. Blood pressure monitoring is recommended during initiation. Hemodynamic assessment (BP, HR, symptoms of vasodilation including flushing and presyncope) is standard across protocols [2][8].
The dosing protocols above involve numbers that matter: specific microgram amounts, reconstitution ratios, and timing windows. Getting any of these wrong compounds across every subsequent dose from that vial.
Doserly's dose and reconstitution calculators eliminate the guesswork. Enter your vial size, peptide amount, and target dose, and get the exact bacteriostatic water volume, units per tick mark, and doses per vial. The injection site tracker maps your administration history as a visual heat map across your body, flagging areas that need rest and suggesting rotation patterns. Combined with dose reminders that include compound name, amount, and route, every aspect of your daily protocol is handled with the precision it requires.
Turn symptom and safety notes into a clearer timeline.
Doserly helps you log doses, symptoms, and safety observations side by side so patterns are easier to discuss with a qualified clinician.
Pattern view
Logs and observations

Pattern visibility is informational and should be reviewed with a clinician.
What to Expect
VIP's timeline of effects varies significantly based on the delivery route, the condition being addressed, and individual biology. The following timeline reflects commonly reported experiences, primarily from CIRS and chronic inflammation contexts.
Weeks 1-2. Some individuals report early improvements in energy and brain fog. Others notice nothing initially. Side effects during this period may include mild headaches, nasal irritation (for intranasal use), or temporary flushing. These typically diminish with continued use. Blood pressure monitoring during this early phase is important.
Weeks 2-6. Progressive improvement in fatigue, cognitive function, and respiratory symptoms is commonly reported. For those tracking inflammatory biomarkers, C4a and TGF-beta1 levels may begin trending downward. Sleep patterns may begin to stabilize, particularly with consistent morning administration.
Months 2-6. More significant symptom improvement for most responders. In the CIRS context, grey matter volume changes may be detectable on specialized brain imaging. Downstream effects on cortisol patterns, thyroid function, and hormone regulation may become apparent as hypothalamic function normalizes.
Months 6-12+. Protocol completion point for many users. Some discontinue with sustained improvement. Others continue at reduced frequency for maintenance. The CIRS literature describes protocol completion at this stage, with some patients maintaining benefits after discontinuation.
It is important to note that VIP has the highest reported failure rate when patients skip prerequisite steps in the Shoemaker CIRS protocol. The compound was designed as a final restoration step, not a first-line intervention. Patience is also critical; VIP works on a timeline of months, not days.
Interaction Compatibility
Potentially Synergistic Combinations
- Selank — Complementary autonomic rebalancing through distinct anxiolytic and immunomodulatory pathways. Selank provides evening anxiolytic support paired with VIP's morning circadian role.
- BPC-157 — Gut barrier support alongside VIP's immune tolerance programming. BPC-157 operates on overlapping gut barrier targets through distinct receptor pathways.
- DSIP — Nighttime sleep architecture support following VIP's daytime circadian synchronization. DSIP promotes deep sleep where growth hormone pulses and immune clearance occur.
- TB-500 — Tissue repair support. TB-500's repair mechanisms complement VIP's M2 macrophage polarization and anti-inflammatory programming.
- GHK-Cu — Tissue remodeling and skin/wound healing. Complementary to VIP's barrier repair mechanisms.
- KPV — Complementary NF-kB inhibition for mucosal inflammation. KPV addresses mucosal inflammation through a distinct pathway with more favorable oral bioavailability.
- Thymosin Alpha-1 — Immune consolidation support. TA1's TLR-mediated immune training complements VIP's tolerance programming through distinct pathways.
- LL-37 — Antimicrobial peptide that provides infection defense alongside VIP's immune modulation.
- Semax — BDNF upregulation and cognitive clarity. Morning co-administration with VIP for cognitive and neuroprotective synergy.
- Glutathione — Antioxidant support complementing VIP's anti-inflammatory and barrier-repair mechanisms.
- ARA-290 — Innate repair receptor activation for neuroprotection and tissue repair.
Combinations Requiring Caution
- PDE-5 Inhibitors (sildenafil, tadalafil) — Combined vasodilatory effects may potentiate hypotension. Avoid stacking until individual VIP response is established.
- High-Dose Niacin — Vasodilatory overlap may increase flushing and hypotensive risk.
- Other Vasodilators — Any compound with significant vasodilatory activity should be introduced cautiously alongside VIP.
- Immunosuppressants — VIP's immune modulation combined with pharmaceutical immunosuppression could create excessive immune tolerance. Medical supervision required.
Administration Guide
VIP is administered through multiple routes depending on the research context and clinical goals.
Intranasal Administration. The most commonly reported research route. Materials typically include a nasal spray device or atomizer, bacteriostatic water or sterile saline for reconstitution, and the lyophilized VIP peptide. Administration is performed with the head slightly tilted forward, spraying into one nostril while closing the other. Avoid blowing your nose for at least 30 minutes after administration.
Subcutaneous Injection. Used in some research and practitioner protocols. Standard subcutaneous injection supplies are required: insulin syringes, alcohol swabs, and bacteriostatic water for reconstitution. The abdominal area is the most common injection site.
Timing Considerations. Morning administration (around 6:00 AM or within the first hour of waking) is consistently recommended across sources. This aligns with the cortisol awakening response and VIP's role in circadian synchronization. Most sources advise against administration after 3:00 PM due to mild stimulatory effects that could interfere with sleep onset.
Post-Administration Monitoring. During the initial doses, sit or lie down for 15-30 minutes after administration to monitor for flushing, lightheadedness, or blood pressure changes. Blood pressure monitoring is recommended for the first several doses and whenever the dose is increased.
Supplies & Planning
Materials typically associated with VIP protocols depend on the chosen route of administration.
For Intranasal Use:
- VIP lyophilized peptide (commonly available in 5 mg or 10 mg vials)
- Nasal spray device or atomizer
- Bacteriostatic water or sterile saline for reconstitution
- Syringes for reconstitution (to transfer solution from vial to nasal spray device)
- Blood pressure monitor (recommended for initial monitoring)
For Subcutaneous Use:
- VIP lyophilized peptide (commonly available in 5 mg or 10 mg vials)
- Bacteriostatic water for reconstitution
- Insulin syringes (29-31 gauge, 0.5 mL or 1 mL)
- Alcohol swabs
- Sharps disposal container
- Blood pressure monitor (recommended for initial monitoring)
Due to VIP's very low dose ranges (mcg level), precise reconstitution calculations are essential to ensure accurate dosing. Consult the Doserly reconstitution calculator or a healthcare provider for vial-specific preparation details.
Storage & Handling
VIP is a particularly fragile peptide that requires careful storage and handling.
Lyophilized (Powder Form). Store at -20C or below for long-term storage. Acceptable at 2-8C (refrigerator temperature) for short-term storage of several weeks. Protect from light. Keep the vial sealed and dry until ready for reconstitution.
Reconstituted (Solution Form). Store at 2-8C (refrigerator). Use promptly. VIP degrades more rapidly in solution than most peptides due to its susceptibility to enzymatic degradation and chemical instability. Avoid repeated freeze-thaw cycles. If the solution becomes cloudy or discolored, discard it.
Handling Notes. VIP degrades quickly at room temperature, both in powder and solution form. Minimize time outside refrigeration. For nasal spray preparations, the spray device should be refrigerated between uses. VIP serum testing specimens also require careful handling (plasma collection on ice, rapid processing) because the peptide degrades quickly ex vivo, producing falsely low results from mishandled specimens.
Lifestyle Factors
Several lifestyle practices can complement VIP's mechanisms of action and may influence outcomes.
Circadian Hygiene. Since VIP is the primary synchronizing signal in the brain's master clock, supporting your circadian rhythm through behavioral strategies amplifies what VIP does biochemically. This includes consistent sleep-wake times, morning sunlight exposure within 30-60 minutes of waking, avoiding bright screens in the evening, and maintaining regular meal timing.
Diet and Nutrition. VIP release from enteric neurons is triggered by feeding, so regular meal patterns (rather than irregular or severely restricted eating) support endogenous VIP signaling. Anti-inflammatory dietary patterns (rich in omega-3 fatty acids, colorful vegetables, and fermented foods) may complement VIP's immune-modulatory effects.
Vagal Tone. VIP functions as a co-transmitter in parasympathetic pathways. Practices that enhance vagal tone, such as controlled breathing exercises, cold exposure protocols, and meditation, activate the pathways where VIP operates naturally.
Exercise. Regular aerobic activity supports circadian entrainment and immune function. Avoid intense exercise immediately after VIP administration, particularly during the titration phase, due to potential additive vasodilatory effects.
Monitoring. Key biomarkers to track include hs-CRP (inflammation), CBC with differential (eosinophils in allergic contexts), CMP (sodium, potassium, creatinine for hydration status), ALT/AST (liver function), and lipid panel (TG, HDL-C, LDL-C or ApoB for metabolic/vascular markers). For CIRS patients, additional markers include TGF-beta1, C4a, MMP-9, MSH, and VEGF.
Blood Pressure. Regular blood pressure monitoring is particularly important with VIP due to its vasodilatory effects. Track both seated and standing blood pressure, especially during the first two weeks of use and after any dose adjustments.
Regulatory Status & Research Classification
United States (FDA). VIP (aviptadil) is not FDA-approved for any indication. Aviptadil has been studied in FDA-registered clinical trials for COVID-19-associated respiratory failure (TESICO, NCT04843761; NCT04311697), pulmonary sarcoidosis, and pulmonary hypertension. VIP nasal spray is available through compounding pharmacies as a research compound. The long-acting VIP analog pemziviptadil is in ongoing clinical trials for cardiopulmonary indications.
WADA Status. VIP is not currently listed on the World Anti-Doping Agency Prohibited List.
Active Clinical Trials. Multiple trials have been registered on ClinicalTrials.gov for aviptadil, primarily in respiratory and cardiopulmonary contexts. Pemziviptadil trials are ongoing with once-weekly subcutaneous dosing protocols.
General Classification. VIP is classified as a research peptide in most jurisdictions. It is available from research peptide suppliers and through compounding pharmacies in some regions. Regulatory status changes frequently. Always verify the current legal status of any compound in your specific country or jurisdiction before making any decisions.
FAQ
What is VIP and what does it do?
VIP (Vasoactive Intestinal Peptide) is a naturally occurring 28-amino acid neuropeptide that modulates immune responses, supports gut barrier integrity, and synchronizes circadian rhythms. Despite its name, its primary modern relevance is as an immune tolerance orchestrator rather than a vasodilator.
How is VIP typically administered?
Based on available sources, intranasal spray is the most commonly reported route in research contexts, typically at 50-100 mcg per dose. Subcutaneous injection and inhaled/nebulized forms are also used in various protocols. The choice of route significantly affects outcomes due to VIP's approximately one-minute plasma half-life. Consult a qualified healthcare provider for guidance on administration.
What is VIP nasal spray used for in research?
VIP nasal spray is primarily studied in CIRS (chronic inflammatory response syndrome) and immune modulation research contexts. It provides direct CNS access through olfactory and trigeminal nerve pathways while avoiding the rapid plasma degradation that limits other routes.
What is aviptadil?
Aviptadil is the pharmaceutical name for synthetic VIP. It has been studied in multiple clinical trials, including a 471-patient Phase 3 COVID-19 trial and several Phase 2 studies in respiratory conditions.
What are the main side effects of VIP?
Based on clinical trial and community data, the most commonly reported side effects are mild transient flushing, lightheadedness, and gastrointestinal looseness. These are dose-dependent and typically manageable. Dose-limiting hypotension and tachycardia occur at higher systemic doses, consistent with VIP's vasodilatory mechanism. Consult a healthcare professional regarding individual risk factors.
Why did the largest VIP clinical trial fail?
The TESICO Phase 3 trial (471 patients) used intravenous aviptadil in critically ill COVID-19 patients and was stopped for futility. VIP has a plasma half-life of approximately one minute, so IV delivery may not sustain adequate tissue concentrations. The positive results from the 80-patient inhaled aviptadil trial suggest that route selection, rather than mechanism failure, may explain the divergence.
Can VIP levels be tested through blood work?
Yes. Serum VIP testing is available through standard reference laboratories. Elevated VIP may suggest a VIPoma (a rare neuroendocrine tumor) or counter-regulatory release during active inflammation. Low VIP in the context of chronic inflammatory symptoms is observed in CIRS cohorts. Specimens require plasma collection on ice with rapid processing, as VIP degrades quickly ex vivo.
How long does it take to see results from VIP?
Based on community reports, some individuals report early improvements in energy and cognitive clarity within 1-2 weeks. More substantial improvements are commonly reported at 2-6 weeks, with inflammatory biomarker normalization occurring over months. VIP is generally described as working on a timeline of months rather than days.
Is VIP safe with other peptides?
Sources frequently mention VIP being combined with peptides like Selank, BPC-157, DSIP, and KPV. However, caution is warranted with any vasodilatory compounds, and combinations should be discussed with a healthcare professional who can assess individual risk factors and potential interactions.
What is the relationship between VIP and CIRS/mold illness?
VIP nasal spray is the final step in the Shoemaker CIRS protocol, used after biotoxin sources have been removed and preceding protocol steps completed. Research suggests VIP helps normalize inflammatory markers and restore regulatory immune function in CIRS patients. Based on available data, VIP has the highest reported failure rate when patients skip prerequisite protocol steps.
Sources & References
[1] Said SI, Mutt V. "Polypeptide with broad biological activity: isolation from small intestine." Science. 1970;169(3951):1217-1218.
[2] Delgado M, Ganea D. "Vasoactive intestinal peptide: a neuropeptide with pleiotropic immune functions." Amino Acids. 2013;45(1):25-39. PMC3883350.
[3] Smalley SG, Barrow PA, Foster N. "Immunomodulation of innate immune responses by vasoactive intestinal peptide (VIP): its therapeutic potential in inflammatory disease." Brain Behav Immun. 2009;23(6):1361-1370. PMC2730848.
[4] Youssef JG, Lavin P, Schoenfeld DA, et al. "The Use of IV Vasoactive Intestinal Peptide (Aviptadil) in Patients With Critical COVID-19 Respiratory Failure: Results of a 60-Day Randomized Controlled Trial." Crit Care Med. 2022;50(11):1545-1554. PMID: 36044317. doi:10.1097/CCM.0000000000005660.
[5] NeuroRx/Relief Therapeutics. Phase 2 RCT of inhaled aviptadil in COVID-19. 80-patient trial demonstrating reduced hospital stay (7.8 vs 10 days).
[6] Prasse A, Zissel G, Lutzen N, et al. "Inhaled vasoactive intestinal peptide exerts immunoregulatory effects in sarcoidosis." Am J Respir Crit Care Med. 2010;182(4):540-548. PMID: 20442436.
[7] Shoemaker RC, House D, Ryan JC. "Vasoactive intestinal polypeptide (VIP) corrects chronic inflammatory response syndrome (CIRS) acquired following exposure to water-damaged buildings." Health. 2013;5(3):396-401.
[8] Practitioner-derived dosing protocols extrapolated from IV aviptadil trial exposure levels. No peer-reviewed publication establishes daily subcutaneous native VIP dosing. Long-acting analog pemziviptadil is under investigation in clinical trials.
[9] Juarranz Y, Gutierrez-Canas I, Carrion M, et al. "Th lymphocyte activation alters VPAC1/VPAC2 expression pattern and cellular location." Sci Rep. 2019;9(1):7016. PMC6517580.
[10] Tan YV, Abad C, Lopez R, et al. "VPAC2 receptor deficiency exacerbates experimental autoimmune encephalomyelitis with reduced Treg abundance." J Immunol. 2015;194(1):31-40. PMID: 25305591.
[11] Gonzalez-Rey E, Chorny A, Fernandez-Martin A, et al. "VIP generates human tolerogenic dendritic cells that induce CD4 and CD8 regulatory T cells." Blood. 2006;107(9):3632-3638. PMID: 16397133.
[12] Chorny A, Gonzalez-Rey E, Fernandez-Martin A, et al. "VIP induces regulatory dendritic cells with therapeutic effects on autoimmune disorders." J Immunol. 2005;175(11):7271-7280. PMID: 16301637.
[13] Bains M, Laney C, Wolfe AE, et al. "VIP deficiency and gut microbiota restructuring." Front Microbiol. 2019;10:2689. PMC6900961.
[14] Talbot J, Hahn P, Kroehling L, et al. "Feeding-dependent enteric neuron VIP release activates innate lymphoid cells." Mucosal Immunol. 2022;15(6):1111-1120. PMID: 35501356.
[15] Jayawardena D, Anbazhagan AN, Guzman G, et al. "VIP nanomedicine for colitis." Mol Pharm. 2017;14(11):3698-3708. PMID: 28991483.
[16] Vu TT, Ilio KY, Bhatt H, et al. "Colonic delivery of VIP nanomedicine alleviates colitis." J Control Release. 2020;328:278-291. PMC7713900.
[17] Abad C, Martinez C, Juarranz MG, et al. "Therapeutic effects of vasoactive intestinal peptide in the trinitrobenzene sulfonic acid mice model of Crohn's disease." Gastroenterology. 2003;124(4):961-971. PMID: 12671893.
[18] Abad C, Juarranz Y, Martinez C, et al. "cDNA array analysis of cytokines, chemokines, and receptors involved in the development of TNBS-induced colitis." Inflamm Bowel Dis. 2005;11(7):674-684. PMID: 18667799.
[19] Petkov V, et al. "Vasoactive intestinal peptide as a new drug for treatment of primary pulmonary hypertension." J Clin Invest. 2003;111(9):1339-1346. PMID: 12727926.
[20] Gozes I, Bardea A, Reshef A, et al. "Neuroprotective strategy for Alzheimer disease: intranasal administration of a fatty neuropeptide." Proc Natl Acad Sci USA. 1996;93(1):427-432. PMID: 8552653. doi:10.1073/pnas.93.1.427.
[21] Martinez C, Juarranz Y, Gutierrez-Canas I, et al. "A Clinical Approach for the Use of VIP Axis in Inflammatory and Autoimmune Diseases." Int J Mol Sci. 2020;21:65. doi:10.3390/ijms21010065.
[22] Linden A, Hansson L, Andersson A, et al. "Bronchodilation by an inhaled VPAC(2) receptor agonist in patients with stable asthma." Thorax. 2003;58(3):217-221. PMID: 12612296. doi:10.1136/thorax.58.3.217.
[23] Verma AK, Manohar M, Mishra A. "Role of VIP in allergic diseases." Cytokine Growth Factor Rev. 2017;38:37-48. PMC5705463.
Related Peptide Guides
- Selank — Anxiolytic peptide for autonomic rebalancing; evening complement to VIP's morning circadian role
- BPC-157 — Tissue repair and gut barrier support through complementary receptor pathways
- TB-500 — Tissue repair peptide with complementary wound healing mechanisms
- DSIP — Delta sleep-inducing peptide for nighttime sleep architecture; pairs with VIP's daytime synchronization
- KPV — Anti-inflammatory tripeptide for gut and mucosal inflammation through NF-kB inhibition
- Thymosin Alpha-1 — Immune modulator with complementary TLR-mediated immune training
- LL-37 — Antimicrobial peptide for infection defense alongside VIP's immune modulation
- GHK-Cu — Tissue remodeling peptide for skin and wound healing
- Semax — Neuroprotective peptide for cognitive support; morning co-administration partner
- ARA-290 — Innate repair receptor activator for neuroprotection and tissue repair
- Glutathione — Antioxidant support complementing VIP's anti-inflammatory mechanisms
- Pinealon — Neurological bioregulator for circadian rhythm and cognitive support
Need the reconstitution math for VIP (Vasoactive Intestinal Peptide): Complete Research Guide?
Open the calculator with VIP (Vasoactive Intestinal Peptide): Complete Research Guide prefilled to estimate concentration, draw volume, and related measurement math from the reconstitution details you already have.