Gabapentin for Menopause: The Complete HRT Guide
On this page
Quick Reference Card
Attribute
Brand Name(s)
- Value
- Neurontin (US, UK, AU, EU); Gralise (US, gastroretentive); Horizant (US, gabapentin enacarbil prodrug); generic widely available worldwide
Attribute
Generic Name
- Value
- Gabapentin
Attribute
Drug Class / Type
- Value
- Anticonvulsant; gamma-aminobutyric acid (GABA) analog; alpha-2-delta calcium channel ligand
Attribute
FDA-Approved Indications
- Value
- Postherpetic neuralgia (adults); adjunctive therapy for partial onset seizures (adults and pediatric patients 3+)
Attribute
Menopause Use Status
- Value
- Off-label; recommended by NAMS (2023), ACOG, and Endocrine Society for vasomotor symptoms
Attribute
Common Doses (for VMS)
- Value
- 300 mg three times daily (most studied); range 100-900 mg at bedtime to 2400 mg/day in divided doses
Attribute
Route(s) of Administration
- Value
- Oral (capsules, tablets, oral solution, gastroretentive tablets)
Attribute
Dosing Schedule
- Value
- Typically divided doses (TID) or single bedtime dose for VMS; titrate over 3-7 days
Attribute
Key Monitoring Requirements
- Value
- Renal function (dose adjustment needed for CrCl <60 mL/min); CNS side effects; suicidal ideation screening; taper on discontinuation
Attribute
Key Differentiator
- Value
- No CYP enzyme interactions (safe with tamoxifen); sleep-promoting properties make it particularly useful for nighttime VMS; no hormonal activity
Overview / What Is Gabapentin for Menopause?
The Basics
Gabapentin is a prescription medication originally developed to treat epilepsy and nerve pain. Over time, clinicians noticed that women taking gabapentin for other conditions were experiencing fewer hot flashes, which led to formal research into its use for menopause symptoms. Today, gabapentin is one of the recommended non-hormonal options for managing hot flashes and night sweats in women who cannot or prefer not to use hormone therapy.
This medication is not FDA-approved specifically for menopause. It is prescribed "off-label," meaning your provider is using it for a purpose supported by clinical evidence even though the drug's official label doesn't list that use. Off-label prescribing is common, legal, and well-established in medicine. The Menopause Society (formerly NAMS) included gabapentin in its 2023 list of recommended non-hormonal therapies for vasomotor symptoms.
Gabapentin occupies a particular niche in menopause management: it is especially useful for women dealing with nighttime hot flashes and sleep disruption, because its sedative properties help with both symptoms simultaneously. It is also one of the few non-hormonal options that does not interfere with tamoxifen, making it valuable for breast cancer survivors experiencing hot flashes from hormone-blocking cancer treatments.
That said, gabapentin is not as effective as hormone therapy (HRT) for managing vasomotor symptoms. Multiple clinical trials and meta-analyses have shown it reduces hot flash frequency by roughly 20-50%, compared to the 75-90% reduction typically seen with estrogen. For women who have the option, HRT remains the most effective treatment. Gabapentin is best understood as a meaningful alternative when HRT is not appropriate.
The Science
Gabapentin (1-(aminomethyl)cyclohexaneacetic acid; C9H17NO2; MW 171.24) is a structural analog of gamma-aminobutyric acid (GABA) that was initially synthesized to mimic GABA's ability to cross the blood-brain barrier. Despite its structural similarity, gabapentin does not bind to GABA-A or GABA-B receptors, is not converted to GABA or a GABA agonist, and does not inhibit GABA uptake or degradation [1].
First approved by the FDA in 1993 for adjunctive treatment of partial seizures (NDA 020235, Pfizer/Parke-Davis), gabapentin's potential for vasomotor symptom management was first described by Guttuso in 2000 in a case series of six women with refractory hot flashes [2]. Subsequent randomized controlled trials and three independent systematic reviews/meta-analyses have established gabapentin as a modestly effective non-hormonal therapy for vasomotor symptoms [3][4][5].
The 2023 Nonhormone Therapy Position Statement of The Menopause Society recommends gabapentin alongside SSRIs/SNRIs, oxybutynin, and fezolinetant as evidence-based non-hormonal treatments for vasomotor symptoms [6]. Notably, the same position statement does NOT recommend clonidine or pregabalin, despite their historical use for hot flashes.
Medical / Chemical Identity
Property
Generic Name
- Value
- Gabapentin
Property
Chemical Name
- Value
- 1-(aminomethyl)cyclohexaneacetic acid
Property
Molecular Formula
- Value
- C9H17NO2
Property
Molecular Weight
- Value
- 171.24 g/mol
Property
CAS Number
- Value
- 60142-96-3
Property
Drug Class
- Value
- Anticonvulsant; GABA analog; alpha-2-delta ligand
Property
Initial FDA Approval
- Value
- 1993 (NDA 020235)
Property
Original Manufacturer
- Value
- Parke-Davis (now Pfizer)
Property
Current Manufacturers
- Value
- Pfizer (Neurontin); Depomed (Gralise); numerous generic manufacturers
Property
Controlled Substance Status
- Value
- Not federally scheduled; Schedule V in some US states
Available Formulations:
Formulation
Capsules (Neurontin, generics)
- Strengths
- 100 mg, 300 mg, 400 mg
- Notes
- Most commonly prescribed for VMS
Formulation
Tablets (generics)
- Strengths
- 100 mg, 300 mg, 400 mg, 600 mg, 800 mg
- Notes
- Scored tablets available
Formulation
Oral Solution
- Strengths
- 250 mg/5 mL
- Notes
- Useful for precise dose titration
Formulation
Gastroretentive Tablets (Gralise)
- Strengths
- 300 mg, 600 mg
- Notes
- Extended absorption; studied in Phase 3 hot flash trial
Formulation
Gabapentin Enacarbil (Horizant)
- Strengths
- 600 mg
- Notes
- Prodrug; approved for RLS and PHN, not typically used for VMS
Brand Names by Country:
- United States: Neurontin, Gralise, Horizant (enacarbil)
- United Kingdom: Neurontin, generics
- Canada: Neurontin, generics
- Australia: Neurontin, generics
- European Union: Neurontin, generics (widely available)
Mechanism of Action
The Basics
Despite decades of use, exactly how gabapentin reduces hot flashes is still not fully understood. What researchers do know is that gabapentin crosses into the brain and binds to specific sites on nerve cells called alpha-2-delta subunits of voltage-gated calcium channels. By binding there, it reduces the release of certain excitatory chemical messengers between nerve cells.
Think of it this way: during menopause, the brain's thermostat (located in a region called the hypothalamus) becomes overly sensitive. Small temperature fluctuations that would normally be ignored instead trigger the body's cooling response, leading to a hot flash. Gabapentin appears to calm this oversensitive thermostat by reducing the excitatory nerve signals in that region.
The fact that gabapentin also promotes drowsiness and calmness helps explain why it works particularly well for nighttime hot flashes and sleep disruption. It essentially reduces the brain's excitability across several systems at once, calming both the thermal trigger point and the arousal circuits that keep you awake.
Importantly, gabapentin has no hormonal activity whatsoever. It does not provide estrogen, progesterone, or any other hormone. This is precisely why it is useful for women who cannot take hormones. However, it also means gabapentin does not provide the broader systemic benefits of HRT, such as bone protection, cardiovascular health support, or genitourinary symptom relief.
The Science
Gabapentin's primary molecular target is the alpha-2-delta (alpha2delta) subunit of voltage-gated calcium channels, specifically the alpha2delta-1 isoform. Binding to this subunit reduces calcium influx at presynaptic nerve terminals, decreasing the release of excitatory neurotransmitters including glutamate, norepinephrine, and substance P [7].
The precise mechanism by which this calcium channel modulation reduces vasomotor symptoms is not definitively established. The leading hypothesis involves the thermoregulatory center in the preoptic area of the anterior hypothalamus. Declining estrogen levels narrow the thermoneutral zone, and elevated noradrenergic signaling in the hypothalamus is implicated in triggering inappropriate heat-dissipation responses. By reducing norepinephrine release at hypothalamic synapses, gabapentin may widen the thermoneutral zone and raise the threshold for triggering vasomotor events [8].
Additional proposed mechanisms include:
- Modulation of GABAergic interneuron activity (indirect, not via direct GABA receptor binding)
- Reduction of calcitonin gene-related peptide (CGRP) release, which is implicated in vasodilation during hot flashes
- Possible interaction with the neurokinin B/kisspeptin/dynorphin (KNDy) neuronal pathway, though gabapentin's mechanism is upstream and less specific than NK3 receptor antagonists like fezolinetant [9]
Gabapentin does not bind to GABA-A or GABA-B receptors, does not interact with benzodiazepine binding sites, and does not inhibit GABA transporters. It is not metabolized to GABA [1]. The drug has no activity at estrogen receptors, progesterone receptors, or any other steroid hormone receptors.
Pathway & System Visualization
Pharmacokinetics / Hormone Physiology
The Basics
Gabapentin is taken by mouth and absorbed through the intestines, but its absorption has an unusual quirk: the body can only absorb so much at a time. At lower doses (100-300 mg), your body absorbs about 60% of the drug. At higher doses (1600 mg), absorption drops to about 35%. This is because gabapentin relies on a specific transport system in the gut (the same one that moves the amino acid L-leucine) that becomes saturated at higher doses.
This saturable absorption is why gabapentin is typically given in divided doses throughout the day rather than one large dose. For menopause-related hot flashes, many women find a single dose at bedtime works well, since the sedative effect aligns with sleep. Others benefit from two or three doses spread through the day.
Once absorbed, gabapentin is not processed by the liver. Unlike many medications, it does not interact with the liver's cytochrome P450 enzyme system at all. This is one of its major practical advantages: it does not affect or get affected by most other medications. It is eliminated unchanged through the kidneys, with a half-life of about 5-7 hours.
For women with kidney problems, dose adjustments are necessary because the drug clears more slowly. Your provider will calculate the appropriate dose based on your kidney function.
The Science
Absorption: Gabapentin is absorbed from the GI tract via the L-amino acid transport system (LAT1, system b0,+). This carrier-mediated process is saturable, resulting in dose-dependent bioavailability: approximately 60% at 300 mg, 47% at 600 mg, 34% at 900 mg, and 33% at 1600 mg [1]. The gastroretentive formulation (Gralise) uses a polymer matrix to extend gastric residence time, improving bioavailability at higher doses. Tmax is approximately 2-3 hours for immediate-release formulations.
Distribution: Volume of distribution is approximately 58 L (0.65 L/kg). Gabapentin does not bind to plasma proteins. It crosses the blood-brain barrier.
Metabolism: Gabapentin is not appreciably metabolized in humans. It does not induce or inhibit CYP1A2, CYP2A6, CYP2C9, CYP2C19, CYP2D6, CYP2E1, or CYP3A4 [1]. This lack of hepatic metabolism eliminates drug-drug interactions via the CYP system, a significant clinical advantage.
Elimination: Eliminated unchanged by renal excretion and renal tubular secretion. Terminal half-life: 5-7 hours. Renal clearance is approximately 190 mL/min. Dose adjustment required for CrCl <60 mL/min [1].
PK Parameter
Bioavailability
- Value
- 60% (300 mg) to 33% (1600 mg)
PK Parameter
Tmax
- Value
- 2-3 hours (IR); 8 hours (Gralise)
PK Parameter
Protein Binding
- Value
- None (<3%)
PK Parameter
Metabolism
- Value
- None (no CYP involvement)
PK Parameter
Half-life
- Value
- 5-7 hours
PK Parameter
Elimination
- Value
- Renal (unchanged)
Research & Clinical Evidence
The Basics
The evidence that gabapentin helps with hot flashes comes from multiple randomized controlled trials and three independent meta-analyses. The research consistently shows gabapentin is better than placebo and helpful for many women, but not as effective as estrogen therapy.
In clinical trials, gabapentin at doses of 900 mg per day (300 mg three times daily) typically reduces hot flash frequency by 45-50% compared to about 29% for placebo. At higher doses (2400 mg/day), one small study found gabapentin nearly matched estrogen, reducing hot flash severity by 71% compared to 72% for estrogen and 54% for placebo. However, that particular study was very small, so the results should be interpreted cautiously.
One of the largest and most rigorous trials was a Phase 3 study of 600 women using a gastroretentive gabapentin formulation (1800 mg/day). After 12 weeks, significantly more women on gabapentin reported being "much" or "very much" improved compared to placebo (58% vs 44%). The improvement was maintained through 24 weeks. This trial also showed meaningful improvement in sleep quality.
For breast cancer survivors experiencing hot flashes from tamoxifen or aromatase inhibitors, gabapentin is a particularly important option. Unlike some antidepressants (particularly paroxetine and fluoxetine), gabapentin does not interfere with the CYP2D6 enzyme that converts tamoxifen to its active form. Both meta-analyses confirmed gabapentin benefits both natural menopause and treatment-induced menopause equally.
When compared to antidepressants like venlafaxine, gabapentin appears roughly similar in reducing hot flash severity, though the studies are limited. Estrogen remains clearly more effective than either.
The Science
Systematic Reviews and Meta-Analyses:
Shan et al. (2020) conducted the most comprehensive meta-analysis, including 19 RCTs and 2 randomized crossover trials (n=3,519). Results showed gabapentin significantly reduced hot flash frequency (mean difference -1.62, 95% CI: -1.98 to -1.26 at 4 weeks; -2.77, 95% CI: -4.29 to -1.24 at 12 weeks) and composite score (SMD -0.47, 95% CI: -0.71 to -0.23 at 4 weeks; -0.77, 95% CI: -1.15 to -0.40 at 12 weeks) versus placebo [3].
Liu et al. (2020) analyzed 7 RCTs comparing single-agent gabapentin with placebo and found significant reductions in hot flush frequency (SMD 2.99, 95% CI: 2.01-3.98), duration (SMD 0.89, 95% CI: 0.49-1.30), and composite score (SMD 2.31, 95% CI: 1.50-3.11), all with P < 0.001 [4].
Toulis et al. (2009) conducted an earlier meta-analysis finding 20-30% reductions in frequency and severity, noting significant between-study heterogeneity (I2 = 97.8%) [5].
Phase 3 RCT (Pinkerton et al., 2014):
The largest randomized controlled trial enrolled 600 women with 7+ moderate-to-severe hot flashes per day. Gastroretentive gabapentin (G-GR; 600 mg AM/1200 mg PM) was compared to placebo over 24 weeks [10]:
- Hot flash frequency reduction vs placebo: -1.7 (P < 0.0001) at week 4; -1.14 (P = 0.0007) at week 12
- Patient Global Impression of Change: 76% "much/very much improved" at week 24 vs 55% placebo (P < 0.0001)
- Sleep interference significantly reduced at week 12 (P = 0.0056) and week 24 (P = 0.0084)
- Dropout for adverse events: 16.7% G-GR vs 11.5% placebo
Comparative Efficacy:
Gabapentin versus estrogen: Shan et al. found estrogen was more effective than gabapentin for hot flash frequency reduction [3]. Reddy et al. (small RCT, n=60) found gabapentin 2400 mg/day reduced hot flash composite scores by 71% versus 72% for conjugated estrogen 0.625 mg/day and 54% for placebo, suggesting high-dose gabapentin may approach estrogen efficacy, though the study was underpowered [11].
Gabapentin versus antidepressants: No statistically significant difference in hot flash severity score reduction between gabapentin and antidepressants was found in the Shan meta-analysis [3].
Breast cancer population: Both meta-analyses confirmed benefit in breast cancer patients experiencing treatment-induced vasomotor symptoms, with efficacy comparable to that seen in natural menopause populations [3][4].
Evidence & Effectiveness Matrix
Category
Vasomotor Symptoms
- Evidence Strength
- 9/10
- Reported Effectiveness
- 8/10
- Summary
- Three meta-analyses, multiple RCTs, Phase 3 trial. Consistent 20-50% hot flash frequency reduction vs placebo. 84% positive Drugs.com rating for hot flashes.
Category
Sleep Quality
- Evidence Strength
- 7/10
- Reported Effectiveness
- 8/10
- Summary
- Phase 3 RCT demonstrated significant sleep interference reduction. Community reports overwhelmingly positive for sleep. Sedative properties are a co-benefit.
Category
Mood & Emotional Wellbeing
- Evidence Strength
- 3/10
- Reported Effectiveness
- 4/10
- Summary
- Limited clinical trial data for mood in menopause context. Community reports divided: some report mood stabilization, others report depression and suicidal ideation (AED class warning applies).
Category
Anxiety & Stress Response
- Evidence Strength
- 4/10
- Reported Effectiveness
- 6/10
- Summary
- Gabapentin has some evidence for anxiety disorders (off-label). Community reports of anxiety reduction during menopause are positive but limited.
Category
Cognitive Function
- Evidence Strength
- 3/10
- Reported Effectiveness
- 3/10
- Summary
- Known CNS depressant. Clinical trials report dizziness and somnolence. Community reports raise concern about memory and cognitive impairment, particularly with long-term use.
Category
Energy & Fatigue
- Evidence Strength
- 3/10
- Reported Effectiveness
- 4/10
- Summary
- Drowsiness/fatigue is a known adverse effect. Community experience is mixed: better sleep leads to more energy for some, but daytime sedation is problematic for others.
Category
Joint & Musculoskeletal Health
- Evidence Strength
- 4/10
- Reported Effectiveness
- 6/10
- Summary
- Gabapentin is an established analgesic. Some community reports of menopause-related joint pain improvement. Not studied specifically for menopause-related musculoskeletal symptoms.
Category
Headache & Migraine
- Evidence Strength
- 5/10
- Reported Effectiveness
- 6/10
- Summary
- Gabapentin has evidence for migraine prophylaxis (off-label). Some community reports of menopause-related headache improvement. May be particularly useful for women with comorbid migraines.
Categories not scored (insufficient data for gabapentin in menopause context): Sexual Function & Libido, Genitourinary Health (GSM), Bone Health & Osteoporosis, Cardiovascular Health, Metabolic Health & Insulin Sensitivity, Body Composition & Weight, Skin/Hair/Appearance, Breast Cancer Risk, Endometrial Safety, Thrombotic Risk, Menstrual & Reproductive, Other Physical Symptoms.
Benefits & Therapeutic Effects
The Basics
Gabapentin's primary benefit in menopause management is the reduction of hot flashes and night sweats. For many women, particularly those taking it at bedtime, the improvement can be substantial. Clinical trials show roughly half the women who try gabapentin experience meaningful improvement in their vasomotor symptoms.
Beyond hot flashes, gabapentin offers several secondary benefits that make it particularly suited for certain women:
Sleep improvement is the most consistently reported co-benefit. Because gabapentin promotes drowsiness, taking it at bedtime can address both night sweats and the sleep disruption they cause. This two-for-one effect is a genuine advantage over some other non-hormonal options.
Pain relief is another potential benefit. Women experiencing menopause-related joint pain, neuropathy, or chronic pain conditions may find gabapentin addresses multiple symptoms simultaneously. It is FDA-approved for postherpetic neuralgia and has established evidence for other pain conditions.
Anxiety reduction has been reported by some women, though the evidence base is thinner here. The calming effect of gabapentin may help with the heightened anxiety that often accompanies perimenopause and menopause.
Migraine prevention is another off-label use with supporting evidence. Women whose migraines worsen during the menopausal transition may benefit from gabapentin's migraine prophylactic properties.
It is important to be clear about what gabapentin does not do. It does not provide estrogen or any hormonal activity. It does not protect bone density, improve vaginal dryness, support cardiovascular health, or provide the systemic benefits associated with HRT. If those outcomes are important and HRT is not contraindicated, gabapentin alone would not address them.
The Science
Primary Efficacy (Vasomotor Symptoms):
Across three meta-analyses, gabapentin at 900 mg/day demonstrates a statistically significant and clinically meaningful reduction in hot flash frequency and severity compared to placebo [3][4][5]. The Phase 3 trial of gastroretentive gabapentin (1800 mg/day) showed sustained efficacy through 24 weeks, with 76% of treated women reporting meaningful improvement [10].
Dose-response data from Guttuso et al. show progressive benefit: 21% severity reduction at 300 mg/day, 33% at 600 mg/day, and 49% at 900 mg/day [12]. This dose-response relationship has been replicated in subsequent trials.
Secondary Benefits (Evidence Level):
- Sleep quality: Supported by Phase 3 RCT data (P = 0.0056 at week 12) [10] and consistent community reports. The GABAergic effect on sleep architecture likely contributes alongside VMS reduction.
- Analgesic effect: Well-established for neuropathic pain (FDA-approved indication). Mechanistically plausible for menopause-related joint pain via alpha-2-delta-mediated inhibition of pain signaling [7].
- Anxiolytic effect: Some RCT evidence for generalized anxiety disorder; less studied in menopause-specific anxiety. Mechanism likely involves reduction of excitatory neurotransmission in amygdala circuits [13].
- Migraine prophylaxis: Level B evidence per American Academy of Neurology guidelines. Useful for women with comorbid menopause-exacerbated migraines [14].
Risks, Side Effects & Safety
The Basics
Gabapentin is generally well tolerated, but it does have a meaningful side effect profile that every woman considering it should understand. The most common side effects are drowsiness, dizziness, and fatigue. For many women taking gabapentin at bedtime for hot flashes, the drowsiness is actually helpful. But for those needing daytime doses, it can interfere with daily activities, driving, and work.
Common side effects (occurring in more than 5% of users in clinical trials):
- Drowsiness/somnolence (the most common)
- Dizziness
- Fatigue
- Peripheral edema (swelling in hands and feet)
- Headache
Less common but notable side effects:
- Weight gain (reported by some long-term users)
- Blurred vision
- Dry mouth
- Nausea
- Coordination problems (ataxia)
- Difficulty concentrating or memory problems
Serious concerns to be aware of:
Suicidal thoughts and behavior: All anti-seizure medications, including gabapentin, carry an FDA-mandated warning about increased risk of suicidal thoughts and behavior. In community reports, a small but notable number of women have reported dark thoughts or suicidal ideation while on gabapentin. If you experience any changes in mood, increased anxiety, depression, or thoughts of self-harm, contact your healthcare provider immediately.
Withdrawal symptoms: Gabapentin should never be stopped suddenly. Abrupt discontinuation can cause anxiety, insomnia, nausea, pain, and sweating. In people taking it for seizures, stopping suddenly can trigger seizures. Always taper gradually under your provider's guidance.
Respiratory depression: Gabapentin can suppress breathing, especially when combined with opioids or other CNS depressants, or in people with underlying respiratory conditions like COPD or sleep apnea.
Cognitive effects: Some long-term users report significant impacts on memory, concentration, and mental clarity. These reports are more prominent in community discussions than in clinical trials, but they are consistent enough to warrant attention.
Abuse potential: While gabapentin is not a federally controlled substance, several US states have reclassified it as a Schedule V controlled substance due to reports of misuse. This is more relevant for individuals with a history of substance use disorder.
The Science
Clinical Trial Safety Data:
In the Phase 3 hot flash trial (Pinkerton et al., n=600), the most common adverse events with gastroretentive gabapentin versus placebo were [10]:
- Dizziness: 12.7% vs 3.4%
- Headache: 9.3% vs 8.1%
- Somnolence: 6.0% vs 2.7%
- Dropout due to adverse events: 16.7% vs 11.5%
Meta-analysis safety data (Shan et al.) confirmed significantly elevated risk of dizziness (RR 4.45, 95% CI: 2.50-7.94) and somnolence (RR 3.29, 95% CI: 1.97-5.48) with gabapentin versus placebo [3].
Suicidality Risk:
The FDA's 2008 meta-analysis of 199 placebo-controlled trials of 11 AEDs (including gabapentin) found an estimated suicidality risk of 0.43% in AED-treated patients versus 0.24% in placebo-treated patients, yielding an odds ratio of approximately 1.80 [15]. The absolute risk increase is small (approximately 2 additional cases per 1,000 patients), but monitoring is recommended.
Withdrawal and Dependence:
Physical dependence can develop with chronic use. The prescribing information recommends tapering over at least one week when discontinuing [1]. Community reports suggest that longer tapers (over 2-4 weeks or more, especially at higher doses) may be better tolerated. Withdrawal symptoms include anxiety, insomnia, nausea, pain, diaphoresis, and in patients with seizure disorders, potential seizure exacerbation.
Renal Considerations:
Gabapentin is eliminated unchanged by the kidneys. Dose adjustment is required for renal impairment. Age-related decline in renal function is relevant for postmenopausal women, particularly those over 65 [1].
Contraindications:
- Known hypersensitivity to gabapentin
- Relative: severe respiratory impairment; concomitant high-dose opioids; history of substance use disorder (increased abuse risk)
Understanding your personal risk profile isn't a one-time calculation; it evolves as your treatment progresses. Doserly helps you see the bigger picture by analyzing side effect patterns over time, showing whether issues are resolving, persisting, or emerging as your body adjusts to therapy.
The app's analytics can reveal connections between side effects and specific aspects of your protocol, like whether symptoms correlate with a particular dose change or timing adjustment. This kind of insight helps you and your provider make informed adjustments based on your actual experience, not just population-level averages.
Connect protocol changes to labs and health markers.
Doserly can keep lab results, biomarkers, symptoms, and dose history close together so follow-up conversations have better context.
Insights
Labs and trends
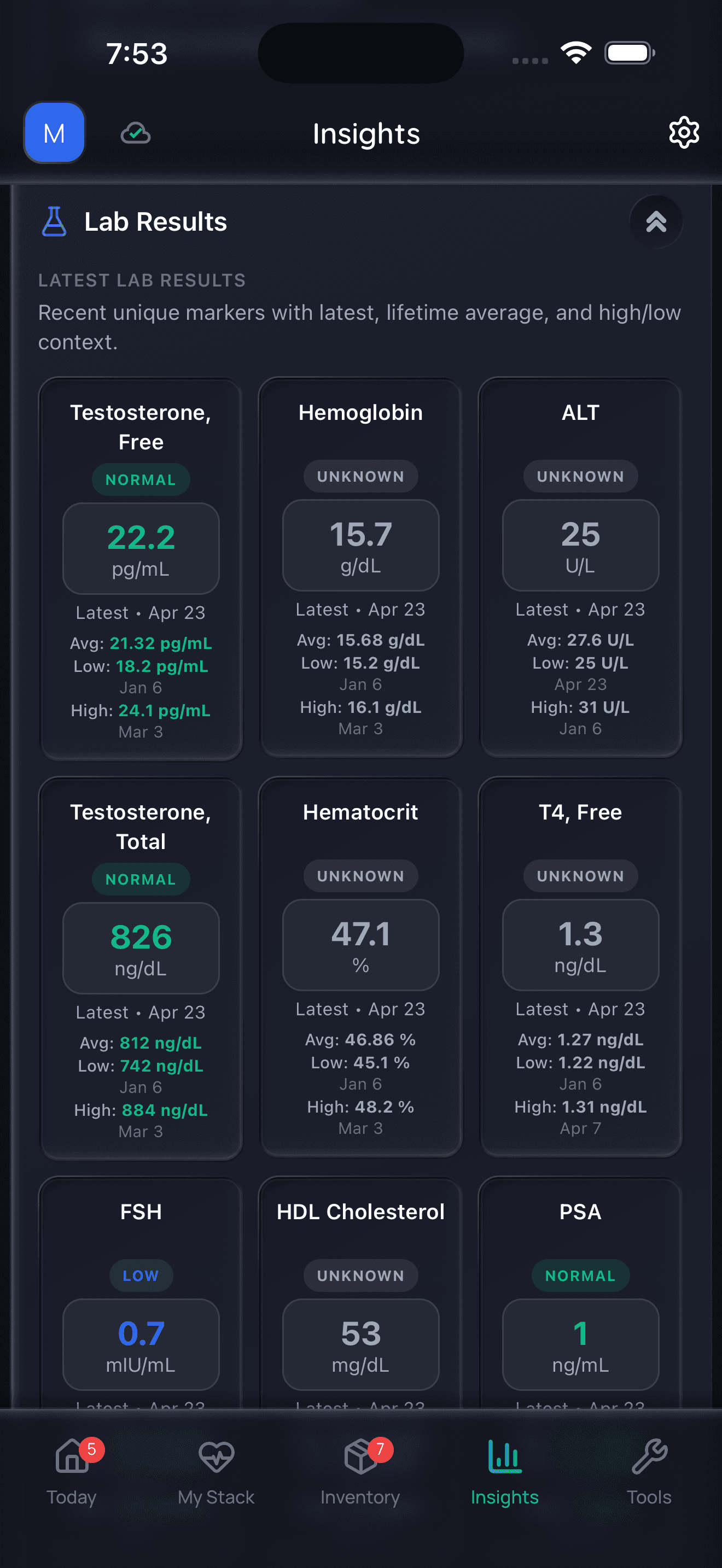
Doserly organizes data; it does not diagnose or interpret labs for you.
Dosing & Treatment Protocols
The Basics
Gabapentin dosing for hot flashes is different from its dosing for seizures or nerve pain. Most providers start with a low dose and increase gradually, a process called titration. This approach minimizes side effects, particularly the drowsiness and dizziness that are most noticeable in the first days of treatment.
A common starting approach:
- Start with 100-300 mg at bedtime for 3-5 days
- If needed and tolerated, increase to 300 mg twice daily
- Can further increase to 300 mg three times daily (900 mg/day total)
The most commonly studied dose for hot flashes is 900 mg per day (300 mg three times daily). However, many women find lower doses effective, particularly for nighttime symptoms. Community reports suggest that some women do well on as little as 100 mg at bedtime.
For the gastroretentive formulation (Gralise), the Phase 3 trial used 600 mg in the morning and 1200 mg in the evening, for a total of 1800 mg/day. This formulation was designed to improve absorption at higher doses.
Key dosing principles:
- Start low, go slow
- Bedtime dosing leverages the sedative effect
- Divided doses may be needed for all-day coverage
- The lowest effective dose is the goal
- Higher doses (up to 2400 mg/day) may provide additional benefit but also more side effects
- Always taper when stopping (never quit abruptly)
If you have kidney concerns: Your provider should adjust the dose based on your kidney function. This is particularly relevant for women over 65, where age-related kidney changes are common.
The Science
Evidence-Based Dosing:
Dose
300 mg/day
- Evidence Level
- RCT data
- Hot Flash Reduction
- ~21% severity reduction
- Notes
- Minimal effective dose [12]
Dose
900 mg/day (300 mg TID)
- Evidence Level
- Multiple RCTs, meta-analyses
- Hot Flash Reduction
- 45-49% frequency/severity reduction
- Notes
- Most commonly studied [3][4][5]
Dose
1800 mg/day (G-GR)
- Evidence Level
- Phase 3 RCT
- Hot Flash Reduction
- Significant vs placebo through 24 weeks
- Notes
- Gastroretentive formulation [10]
Dose
2400 mg/day
- Evidence Level
- Small RCT
- Hot Flash Reduction
- ~71% composite reduction
- Notes
- Approaches estrogen efficacy; small study [11]
Renal Dose Adjustment:
CrCl (mL/min)
≥60
- Maximum Daily Dose
- Standard dosing
- Frequency
- TID or as directed
CrCl (mL/min)
30-59
- Maximum Daily Dose
- 200-700 mg
- Frequency
- Twice daily
CrCl (mL/min)
15-29
- Maximum Daily Dose
- 200-700 mg
- Frequency
- Once daily
CrCl (mL/min)
<15
- Maximum Daily Dose
- 100-300 mg
- Frequency
- Once daily
Titration Protocol:
Clinical practice typically follows a 3-7 day titration:
- Day 1: 300 mg at bedtime
- Day 3-4: 300 mg in evening, 300 mg at bedtime (or 300 mg twice daily)
- Day 7+: 300 mg three times daily if needed
For women whose primary complaint is nighttime VMS and insomnia, remaining at 300 mg (or less) at bedtime is a reasonable approach before escalating to divided daytime doses, which carry higher daytime sedation risk [10].
Dosing protocols often change over the course of treatment, as starting doses get adjusted, timing gets refined, and response is evaluated. Doserly maintains a complete history of every protocol change, giving you and your provider a clear picture of what's been tried and how each adjustment affected your symptoms.
The app's adherence analytics show your consistency patterns and can highlight whether missed doses or timing variations correlate with symptom changes. When your provider is considering a dose adjustment, having this data available makes the conversation more productive and the decision more informed.
Turn symptom and safety notes into a clearer timeline.
Doserly helps you log doses, symptoms, and safety observations side by side so patterns are easier to discuss with a qualified clinician.
Pattern view
Logs and observations

Pattern visibility is informational and should be reviewed with a clinician.
What to Expect (Timeline)
Days 1-7: Initial Adjustment
- Drowsiness and dizziness are most pronounced in the first few days
- Some women notice hot flash improvement within the first few nights, particularly for nighttime symptoms
- Side effects typically diminish as the body adjusts
- If titrating, you will be increasing the dose during this period
Weeks 2-4: Early Response
- Most clinical trials show statistically significant hot flash reduction by week 4
- Sleep improvement often becomes apparent during this period
- Daytime drowsiness typically settles for most women
- If your hot flashes have not improved at all by week 4, discuss a dose increase with your provider
Months 1-3: Therapeutic Effect
- Full therapeutic effect for vasomotor symptoms is typically established by week 12
- In the Phase 3 trial, 58% of women reported being "much" or "very much" improved at week 12
- Side effects that have not resolved by this point are unlikely to improve with continued use
- This is a reasonable timeframe for evaluating whether gabapentin is working for you
Months 3-6: Sustained Benefit
- Benefit appears to be maintained; the Phase 3 trial showed continued improvement from week 12 to week 24
- 76% of women reported meaningful improvement at week 24
- Annual reassessment is recommended to determine whether continued use is appropriate
Ongoing Maintenance
- There is no established maximum duration for gabapentin use for hot flashes
- Regular reassessment (at least annually) should include: symptom status, side effect evaluation, kidney function check, and discussion of whether menopause symptoms have resolved naturally
- When ready to stop, taper gradually over at least 1-2 weeks (longer for higher doses)
Timelines in clinical literature describe averages. Your own timeline is what matters. Doserly's trend analysis turns your daily symptom entries into visual trajectories, showing you how each symptom is progressing over weeks and months of treatment.
The app helps you see patterns that day-to-day experience can obscure, like a gradual improvement in sleep quality that started two weeks after a dose increase, or hot flash frequency dropping steadily even when individual bad days make it feel like nothing has changed. These insights give both you and your provider a clearer picture of treatment response.
See where a dose, cycle, or change fits in time.
Doserly gives each protocol a timeline so dose changes, pauses, restarts, and observations are easier to compare later.
Timeline
Cycle history
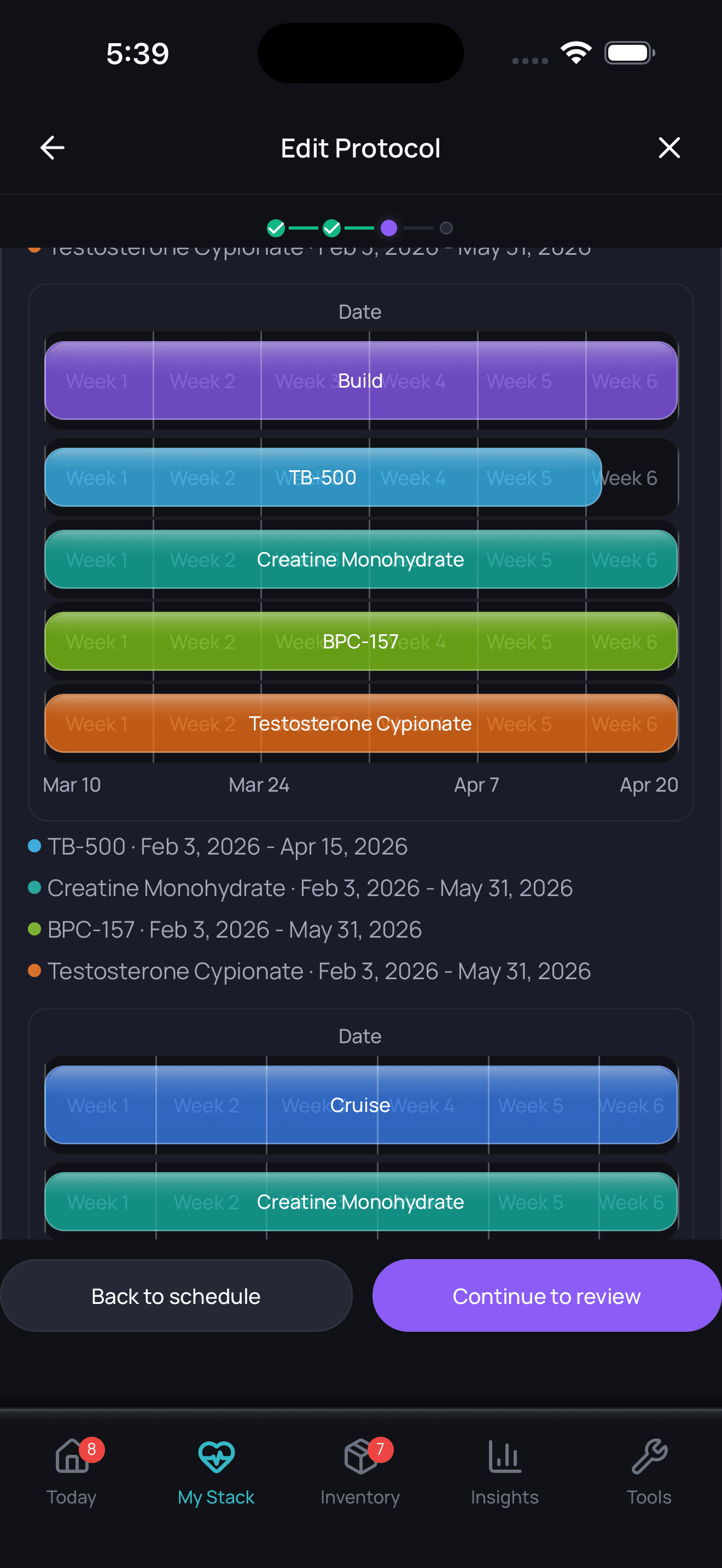
Timeline tracking helps with recall; it is not a treatment recommendation.
Timing Hypothesis & Window of Opportunity
The timing hypothesis (the concept that HRT initiated within 10 years of menopause onset or before age 60 has a more favorable risk-benefit profile) is specific to hormone therapy and does not directly apply to gabapentin. Because gabapentin has no hormonal activity, there is no cardiovascular timing window or hormone-receptor-dependent benefit profile.
However, the timing concept is relevant to the broader treatment decision. A woman in early menopause (within 10 years of onset, under age 60) with no contraindications may have more to gain from HRT than from gabapentin, because HRT within the window of opportunity provides not only superior vasomotor symptom relief but also potential cardiovascular, bone, and genitourinary benefits that gabapentin cannot offer.
For women who have passed the optimal HRT initiation window, or for whom HRT is contraindicated regardless of timing, gabapentin's value as a non-hormonal option is not affected by when menopause occurred.
Interactions & Compatibility
Drug-Drug Interactions:
Gabapentin has a remarkably clean drug interaction profile due to its lack of hepatic metabolism and CYP enzyme involvement.
- Opioids (morphine, hydrocodone, oxycodone): Increased CNS depression risk. Morphine specifically increases gabapentin plasma concentrations by approximately 44%. Use caution and monitor for sedation [1].
- Alcohol and CNS depressants (benzodiazepines, sedative antihistamines, sleep aids): Additive CNS depression. Increased drowsiness, dizziness, and impaired coordination.
- Antacids (aluminum/magnesium hydroxide): Reduce gabapentin bioavailability by approximately 20%. Take gabapentin at least 2 hours after antacids [1].
- Tamoxifen: No interaction. Gabapentin does not affect CYP2D6. This makes it a preferred non-hormonal option for breast cancer patients on tamoxifen, unlike paroxetine and fluoxetine which inhibit CYP2D6 and may reduce tamoxifen's active metabolite [16].
- SSRIs/SNRIs: Generally safe to combine. Some women take both an antidepressant and gabapentin. Monitor for additive sedation.
- Thyroid medications (levothyroxine): No known interaction.
- Blood pressure medications: No significant interactions, though additive dizziness possible with alpha-blockers.
Supplement Interactions:
- Calcium and vitamin D: No known interaction
- Magnesium supplements: Theoretical interaction (magnesium hydroxide reduces absorption, similar to antacids); space doses by 2 hours
- Melatonin: Additive sedation; use caution with combined bedtime dosing
- Black cohosh: No known interaction
- St. John's Wort: No CYP-mediated interaction expected (gabapentin is not CYP-metabolized)
Lifestyle Factors:
- Alcohol: Additive CNS depression. Limit alcohol use, especially when initiating therapy.
- Driving and machinery: Gabapentin impairs coordination and reaction time, particularly during dose titration. Avoid driving until you know how gabapentin affects you.
Cross-References:
- For more on non-hormonal options: Non-Hormonal Menopause Treatments
- For fezolinetant comparison: Fezolinetant (Veozah)
- For paroxetine comparison: Paroxetine (Brisdelle)
- For clonidine comparison: Clonidine for Menopause
Decision-Making Framework
Deciding whether gabapentin is right for managing your menopause symptoms involves weighing several factors with your healthcare provider:
Gabapentin may be a particularly good fit if you:
- Cannot take HRT due to a contraindication (active or recent breast cancer, history of VTE, active liver disease)
- Are taking tamoxifen or an aromatase inhibitor for breast cancer treatment
- Have nighttime hot flashes and night sweats as your primary symptoms
- Struggle with insomnia alongside your vasomotor symptoms
- Have comorbid conditions that gabapentin also treats (neuropathic pain, migraines, restless leg syndrome, anxiety)
- Prefer not to use hormones for personal reasons
Gabapentin may be a less ideal choice if you:
- Have kidney disease or significantly reduced kidney function
- Need optimal daytime alertness (driving, operating machinery, cognitively demanding work)
- Have a history of depression or suicidal ideation
- Have a history of substance use disorder
- Want broader systemic menopause benefits (bone protection, cardiovascular health, GSM relief) that only HRT provides
- Are within the HRT window of opportunity with no contraindications
Questions to ask your provider:
- "Am I a candidate for hormone therapy, and if not, why specifically?"
- "What dose would we start at, and how would we titrate?"
- "How will we evaluate whether gabapentin is working for me?"
- "What's the plan if I want to stop? How would we taper?"
- "Should I have kidney function tested before starting?"
- "How will gabapentin interact with my other medications?"
Finding a menopause specialist: If your provider is not familiar with gabapentin for menopause or with the current NAMS guidelines, consider seeking a NAMS-Certified Menopause Practitioner. These specialists are up to date on all treatment options, including non-hormonal approaches. The Menopause Society maintains a provider directory at menopause.org.
Administration & Practical Guide
Oral Capsules and Tablets:
- Swallow whole with water
- Can be taken with or without food (food does not significantly affect absorption of immediate-release formulations)
- If taking divided doses: space evenly throughout the day (e.g., morning, afternoon, bedtime)
- If taking a single bedtime dose: take 1-2 hours before sleep to allow onset of sedative effect
Gastroretentive Tablets (Gralise):
- MUST be taken with food (significantly affects absorption)
- Swallow whole; do not break, crush, or chew
- Take with the evening meal
Oral Solution (250 mg/5 mL):
- Useful for precise dose titration, especially when starting at doses below 100 mg
- Measure with a calibrated oral syringe or measuring device
- Store at room temperature
Missed Dose:
- If you miss a dose, take it as soon as you remember unless it is nearly time for your next dose
- Do not double up doses
- If taking gabapentin primarily at bedtime and you forget, skip the missed dose and resume the next night
Practical Tips from Community Experience:
- Keep a consistent schedule; gabapentin's short half-life means missed doses can lead to symptom breakthrough
- If drowsiness is problematic during the day, ask your provider about shifting more of the dose to bedtime
- Keep gabapentin out of extreme heat; store at room temperature (68-77 degrees F)
- If splitting a scored tablet, use the other half within a few days
Monitoring & Lab Work
Before Starting Gabapentin:
- Renal function (serum creatinine, estimated GFR/CrCl) to determine if dose adjustment is needed
- Baseline assessment of mood and any history of depression or suicidal ideation
- Review of current medications for potential interactions (especially opioids, CNS depressants)
- Baseline documentation of hot flash frequency and severity (useful for treatment evaluation)
Initial Follow-Up (4-8 Weeks):
- Symptom assessment: Are hot flashes improving? By how much?
- Side effect evaluation: Drowsiness, dizziness, cognitive effects, weight
- Mood screening: Any new depression, anxiety, or suicidal thoughts
- Dose adjustment discussion if needed
Ongoing Monitoring:
- Renal function: Annual check, more frequently for women over 65 or with known kidney disease
- Weight monitoring: Some women experience weight gain on gabapentin
- Cognitive assessment: Informal monitoring for memory or concentration changes
- Annual reassessment of continued need (menopause symptoms may have resolved)
No routine hormone monitoring needed: Unlike HRT, gabapentin does not require estradiol, FSH, or other hormone level testing for dosing purposes.
Complementary Approaches & Lifestyle
Gabapentin can be part of a broader symptom management strategy. Evidence-based complementary approaches include:
Cognitive Behavioral Therapy (CBT):
NAMS recommends CBT for vasomotor symptoms. CBT helps modify the thought patterns and behaviors around hot flashes, reducing their perceived impact. Can be used alongside gabapentin.
Exercise:
While exercise alone is not NAMS-recommended for hot flashes, regular physical activity supports cardiovascular health, bone density, mood, and sleep quality during menopause. Weight-bearing exercise is particularly important for bone health when not on HRT.
Weight Management:
NAMS recommends weight loss (if overweight) as an evidence-based strategy for hot flashes. Maintaining a healthy weight may reduce hot flash frequency.
Sleep Hygiene:
- Cool bedroom environment (65-68 degrees F)
- Moisture-wicking sleepwear and bedding
- Consistent sleep schedule
- Limit caffeine and alcohol, especially in the evening
- Gabapentin's sedative effect complements good sleep hygiene practices
Dietary Considerations:
- Avoid known hot flash triggers (spicy foods, hot beverages, alcohol, caffeine)
- Mediterranean diet pattern supports cardiovascular and metabolic health
- Adequate calcium (1200 mg/day) and vitamin D (800-1000 IU/day) for bone health
Mind-Body Practices:
Clinical hypnosis is NAMS-recommended for hot flashes. Mindfulness meditation may reduce the distress associated with hot flashes even if it does not reduce their frequency.
Supplements with limited evidence:
- Black cohosh: Mixed evidence; not NAMS-recommended
- Soy isoflavones: Not NAMS-recommended
- Vitamin E: Marginal benefit at best
Cross-references:
- For supplement information: Menopause Nutrition & Lifestyle
Stopping HRT / Discontinuation
Although gabapentin is not HRT, the principles of thoughtful discontinuation apply:
When to consider stopping:
- Menopause symptoms have resolved (vasomotor symptoms naturally improve over time for most women)
- Side effects outweigh benefits
- New contraindication develops (e.g., significant renal impairment)
- Transitioning to HRT or another treatment option
- Annual reassessment suggests the medication is no longer needed
Tapering strategy (essential):
Gabapentin should NEVER be stopped abruptly. Gradual dose reduction is required:
- Reduce by 100-300 mg every 3-7 days
- For women on higher doses (900+ mg/day), taper over 2-4 weeks or longer
- For women on low doses (100-300 mg at bedtime), a 1-2 week taper is typically sufficient
- If withdrawal symptoms occur during tapering, slow the taper further
Withdrawal symptoms to expect:
- Return of hot flashes (expected, not a withdrawal symptom per se)
- Anxiety
- Insomnia
- Nausea
- Sweating
- Irritability
- In seizure patients: potential seizure recurrence (not typically a concern for women using gabapentin for menopause only)
What to monitor during discontinuation:
- Hot flash frequency and severity (are they returning, and to what degree?)
- Sleep quality
- Mood and anxiety levels
- Pain (if gabapentin was also managing pain)
Restarting:
If menopause symptoms return after discontinuation and remain bothersome, gabapentin can be restarted. Many women find they need gabapentin for a finite period (2-5 years) corresponding to the most active phase of vasomotor symptoms.
Special Populations & Situations
Breast Cancer Survivors
Gabapentin is a first-line non-hormonal option for breast cancer survivors experiencing hot flashes from tamoxifen, aromatase inhibitors, or ovarian suppression therapy. Its lack of CYP2D6 interaction makes it safer than paroxetine or fluoxetine for women on tamoxifen. Both meta-analyses confirmed efficacy in breast cancer populations [3][4]. The North American Menopause Society and ASCO recommend gabapentin as a treatment option for this population.
Women Over 65
Age-related decline in renal function requires dose adjustment. Start at lower doses and titrate more slowly. Increased fall risk from dizziness and sedation is a significant concern in older women. The American Geriatrics Society Beers Criteria list gabapentin as potentially inappropriate in older adults due to fall risk.
Women with Kidney Disease
Gabapentin is eliminated entirely by the kidneys. Dose must be adjusted based on creatinine clearance. Close monitoring of renal function is essential. Provider guidance is particularly important for this population.
Women with History of Substance Use Disorder
Gabapentin has recognized misuse potential. Several US states classify it as Schedule V. Women with a history of opioid, alcohol, or benzodiazepine use disorder should discuss this risk with their provider. Alternative non-hormonal options (fezolinetant, SSRIs/SNRIs) may be preferable.
Women with Depression or Anxiety Disorders
The AED class warning for suicidality applies. However, some women with menopause-related anxiety report benefit from gabapentin's anxiolytic properties. Close monitoring of mood is essential, particularly in the first months of treatment.
Surgical Menopause
Women who have undergone bilateral oophorectomy often experience severe, abrupt vasomotor symptoms. If HRT is contraindicated, gabapentin can provide meaningful relief. Higher doses may be needed given the severity of symptoms in surgical menopause.
Perimenopause
Gabapentin can be used during perimenopause for vasomotor symptoms, though HRT is generally preferred if not contraindicated. The erratic hormone fluctuations of perimenopause can make symptoms unpredictable; gabapentin's short half-life means it works on a dose-by-dose basis rather than requiring hormonal stabilization.
Regulatory, Insurance & International
United States (FDA):
- FDA-approved for: postherpetic neuralgia, adjunctive therapy for partial seizures
- NOT FDA-approved for: vasomotor symptoms (off-label use)
- No FDA black box warning for menopause use specifically; class AED suicidality warning applies
- Controlled substance status: Not federally scheduled; Schedule V in Alabama, Kentucky, Michigan, North Dakota, Tennessee, Virginia, West Virginia, and several other states
- Generic availability: Widely available, inexpensive (typically $10-30/month without insurance for generic)
- Insurance: Generally covered for off-label use when prescribed; prior authorization rarely required for generic gabapentin
United Kingdom (MHRA):
- Licensed for: epilepsy, peripheral neuropathic pain
- Off-label for menopause (similar to US)
- Reclassified as Class C controlled substance (Schedule 3) in April 2019 due to misuse concerns
- Available on NHS prescription
- NICE NG23 (Menopause) acknowledges gabapentin as a non-hormonal option
Canada (Health Canada):
- Approved for: adjunctive therapy in epilepsy, neuropathic pain
- Off-label for VMS
- Generic widely available
- Provincial coverage varies
Australia (TGA):
- Approved for: adjunctive therapy in epilepsy, neuropathic pain
- Off-label for VMS
- PBS listed for approved indications; off-label menopause use may require private prescription
European Union (EMA):
- Authorized across EU member states
- Approved for epilepsy and peripheral neuropathic pain
- Off-label use for VMS recognized in clinical guidelines across member states
Frequently Asked Questions
Is gabapentin FDA-approved for menopause?
No. Gabapentin is FDA-approved for epilepsy and postherpetic neuralgia. Its use for menopausal hot flashes is off-label. However, off-label prescribing is standard medical practice, and gabapentin is recommended by The Menopause Society (formerly NAMS) as a non-hormonal option for vasomotor symptoms.
How effective is gabapentin compared to HRT for hot flashes?
Clinical evidence consistently shows HRT is more effective than gabapentin for hot flashes. Meta-analyses demonstrate gabapentin reduces hot flash frequency by roughly 20-50%, while estrogen typically provides 75-90% reduction. Gabapentin is best understood as an alternative for women who cannot or prefer not to use HRT.
What is the best dose for hot flashes?
The most commonly studied dose is 900 mg/day (300 mg three times daily). However, many women find meaningful benefit at lower doses, particularly 100-300 mg taken at bedtime. Your provider will help determine the right dose based on your symptom severity and tolerance of side effects.
Can I take gabapentin with HRT?
Yes. There are no known interactions between gabapentin and hormone therapy. Some women use gabapentin in addition to HRT for breakthrough nighttime symptoms or when HRT alone does not fully control hot flashes.
Will gabapentin make me gain weight?
Weight gain is a possible side effect, though not universal. Clinical trial data show modest weight gain in some participants. Community reports are mixed. If weight gain occurs, discuss with your provider whether dose adjustment or an alternative treatment is appropriate.
How long does it take for gabapentin to work for hot flashes?
Most clinical trials show significant improvement by 4 weeks. Some women notice benefit within the first few days, particularly for nighttime symptoms. Full therapeutic effect is typically reached by 12 weeks.
Can I stop gabapentin suddenly?
No. Gabapentin should always be tapered gradually. Abrupt discontinuation can cause withdrawal symptoms including anxiety, insomnia, nausea, and sweating. Work with your provider on a tapering plan.
Is gabapentin safe long-term?
The long-term safety profile of gabapentin for menopause specifically has not been studied in large, dedicated trials. It has been used safely for epilepsy and neuropathic pain for decades. Concerns about long-term cognitive effects have emerged in community reports, though causation has not been established in controlled studies. Regular reassessment with your provider is recommended.
Can I take gabapentin if I've had breast cancer?
Yes. Gabapentin has no hormonal activity and does not interact with tamoxifen's CYP2D6-dependent metabolism. It is one of the recommended non-hormonal options for breast cancer survivors experiencing vasomotor symptoms.
Does gabapentin help with anxiety during menopause?
Some women report anxiety reduction as a benefit, and gabapentin has some evidence for anxiety disorders. However, it is not FDA-approved for anxiety and the evidence in menopause-related anxiety specifically is limited. If anxiety is your primary symptom, discuss targeted treatments with your provider.
What's the difference between gabapentin and pregabalin (Lyrica)?
Both bind to the alpha-2-delta subunit of calcium channels. Pregabalin has higher bioavailability and does not have the saturable absorption of gabapentin. However, the 2023 NAMS Position Statement recommends gabapentin but does NOT recommend pregabalin for vasomotor symptoms, citing insufficient evidence.
Can I drink alcohol while taking gabapentin?
Alcohol increases the CNS depressant effects of gabapentin (drowsiness, dizziness, impaired coordination). Limit alcohol consumption, especially when first starting gabapentin or after dose increases.
Myth vs. Fact
Myth: Gabapentin is "just" a seizure drug and has no place in menopause treatment.
Fact: While gabapentin was originally developed for epilepsy, it has been extensively studied for vasomotor symptoms in menopause. Three independent meta-analyses and a Phase 3 randomized controlled trial support its efficacy. The Menopause Society (formerly NAMS) officially recommends it as a non-hormonal option for hot flashes in its 2023 Position Statement [6].
Myth: Gabapentin works as well as hormone therapy for hot flashes.
Fact: Clinical evidence clearly shows HRT is more effective. Meta-analyses demonstrate gabapentin reduces hot flash frequency by 20-50%, whereas estrogen typically achieves 75-90% reduction [3]. One small study suggested high-dose gabapentin (2400 mg/day) may approach estrogen's efficacy, but this has not been confirmed in larger trials [11].
Myth: Gabapentin is completely safe with no serious side effects.
Fact: Gabapentin is generally well tolerated, but it carries a class-wide FDA warning for increased risk of suicidal thoughts and behavior. It can cause significant drowsiness, dizziness, and cognitive effects. Physical dependence can develop, and withdrawal symptoms occur with abrupt discontinuation. Some states have reclassified it as a controlled substance due to abuse potential [1][15].
Myth: You can stop taking gabapentin whenever you want.
Fact: Gabapentin should always be tapered gradually under medical supervision. Abrupt discontinuation can cause withdrawal symptoms including anxiety, insomnia, nausea, pain, and sweating. For seizure patients, sudden withdrawal can trigger seizures. A gradual taper over 1-4 weeks (or longer for high doses) is standard practice [1].
Myth: Gabapentin provides the same benefits as HRT for menopause.
Fact: Gabapentin addresses vasomotor symptoms (hot flashes, night sweats) and may improve sleep, but it provides none of HRT's systemic benefits. It does not protect bone density, improve vaginal dryness, support cardiovascular health, or address the genitourinary syndrome of menopause. Women who are candidates for HRT and desire these broader benefits should discuss HRT with their provider.
Myth: All anti-seizure medications work for hot flashes.
Fact: The 2023 NAMS Position Statement specifically recommends gabapentin but does NOT recommend pregabalin (Lyrica) for vasomotor symptoms, citing insufficient evidence [6]. Different anti-seizure medications have different mechanisms and different evidence bases for hot flash treatment.
Myth: Gabapentin is addictive.
Fact: Gabapentin is not classified as a federally controlled substance, and most people using it for menopause at standard doses do not develop addiction. However, misuse has been documented, particularly in individuals with history of substance use disorders. Physical dependence (requiring tapering to stop) is different from addiction (compulsive use despite harm). Several US states have scheduled gabapentin due to misuse concerns [1].
Myth: If gabapentin doesn't work in a few days, it won't work at all.
Fact: Clinical trials show that the full effect of gabapentin on hot flashes develops over 4-12 weeks. While some women notice improvement within days, others need several weeks at an adequate dose before seeing meaningful benefit [10]. If there is no improvement after 4-8 weeks at a therapeutic dose, it may be reasonable to try an alternative.
Sources & References
Clinical Guidelines
- Gabapentin capsules prescribing information (Full Prescribing Information). DailyMed/FDA. Revised 3/2022. https://dailymed.nlm.nih.gov/dailymed/lookup.cfm?setid=9d80e67c-44f8-4236-8b8f-4bd2b8c16de7
- The 2023 Nonhormone Therapy Position Statement of The Menopause Society. Menopause. 2023;30(6):573-590. doi:10.1097/GME.0000000000002200
Systematic Reviews & Meta-Analyses
- Shan D, et al. Efficacy and safety of gabapentin and pregabalin in patients with vasomotor symptoms: a systematic review and meta-analysis. Menopause. 2020;27(11):1295-1305. PMID: 31870736.
- Liu YR, et al. Gabapentin for the treatment of hot flushes in menopause: a meta-analysis. Menopause. 2020;27(10):1166-1176. PMID: 32049930.
- Toulis KA, et al. Gabapentin for the treatment of hot flashes in women with natural or tamoxifen-induced menopause: a systematic review and meta-analysis. Clin Ther. 2009;31(2):221-235. PMID: 19302896.
Randomized Controlled Trials
- Pinkerton JV, et al. Phase 3 randomized controlled study of gastroretentive gabapentin for the treatment of moderate-to-severe hot flashes in menopause. Menopause. 2014;21(6):567-573. PMID: 24149930. ClinicalTrials.gov: NCT01080300.
- Reddy SY, et al. Gabapentin, estrogen, and placebo for treating hot flushes: a randomized controlled trial. Obstet Gynecol. 2006;108(1):41-48. PMID: 16816054.
- Guttuso T Jr, et al. Gabapentin's effects on hot flashes in postmenopausal women: a randomized controlled trial. Obstet Gynecol. 2003;101(2):337-345. PMID: 12576259.
Observational Studies & Reviews
- Guttuso T Jr. Gabapentin's effects on hot flashes and hypothermia. Neurology. 2000;54(11):2161-2163. PMID: 10851388.
- Pachman DR, Jones JM, Loprinzi CL. Management of menopause-associated vasomotor symptoms: current treatment options, challenges and future directions. Int J Womens Health. 2010;2:123-135. PMC2971731.
Government/Institutional Sources
- Taylor CP, et al. A summary of mechanistic hypotheses of gabapentin pharmacology. Epilepsy Res. 1998;29(3):233-249. PMID: 9551785.
- Rance NE, et al. Neurokinin B and the hypothalamic regulation of reproduction. Brain Res. 2010;1364:116-128. PMID: 20800582.
- Pande AC, et al. Placebo-controlled study of gabapentin treatment of panic disorder. J Clin Psychopharmacol. 2000;20(4):467-471. PMID: 10917407.
- Silberstein S, et al. Practice parameter: evidence-based guidelines for migraine headache. Neurology. 2000;55(6):754-762. PMID: 10993991.
- FDA. Statistical review and evaluation: antiepileptic drugs and suicidality. 2008. https://www.fda.gov/files/drugs/published/Statistical-Review-and-Evaluation--Antiepileptic-Drugs-and-Suicidality.pdf
- Stearns V, et al. Paroxetine is an effective treatment for hot flashes: results from a prospective randomized clinical trial. J Clin Oncol. 2005;23(28):6919-6930. PMID: 16192581.
Related Guides & Cross-Links
Same Category (Non-Hormonal Prescription)
- Fezolinetant (Veozah) — NK3 receptor antagonist; first FDA-approved non-hormonal treatment for VMS
- Elinzanetant (Lynkuet) — Dual NK1/NK3 antagonist
- Paroxetine (Brisdelle) — Only FDA-approved SSRI for hot flashes
- Clonidine for Menopause — Alpha-2 agonist; not NAMS-recommended
- Ospemifene (Osphena) — SERM for dyspareunia
- Tibolone (Livial) — Synthetic steroid with estrogenic, progestogenic, and androgenic activity
Related Treatment Options
- Non-Hormonal Menopause Treatments — Overview of all non-hormonal options
- Getting Started with HRT — For women considering whether HRT is appropriate
Related Conditions
- Menopause — Overview of menopause and treatment options
- Perimenopause — Transitional stage where VMS often begins
- Surgical Menopause — Abrupt menopause after oophorectomy
Complementary Approaches
- Menopause Nutrition & Lifestyle — Diet, exercise, and lifestyle strategies