Clonidine for Menopause: The Complete HRT Guide
On this page
Quick Reference Card
Attribute
Brand Name(s)
- Value
- Catapres (US, oral); Catapres-TTS (US, transdermal); Dixarit (UK, Australia, Canada); Nexiclon XR (US, ER tablets)
Attribute
Generic Name
- Value
- Clonidine hydrochloride
Attribute
Drug Class / Type
- Value
- Central alpha-2 adrenergic agonist (antihypertensive used off-label for VMS)
Attribute
FDA-Approved Indications
- Value
- Hypertension (NOT FDA-approved for menopausal symptoms)
Attribute
UK Licensing
- Value
- Licensed for vasomotor symptoms of menopause (Dixarit)
Attribute
Common Doses (for VMS)
- Value
- Oral: 0.05-0.1 mg/day in divided doses; Transdermal: 0.1 mg/24 hours patch weekly
Attribute
Route(s) of Administration
- Value
- Oral (immediate-release, extended-release), transdermal patch
Attribute
Dosing Schedule
- Value
- Typically twice daily (oral); weekly (transdermal patch)
Attribute
Key Monitoring Requirements
- Value
- Blood pressure, heart rate; taper on discontinuation
Attribute
Key Safety Warning
- Value
- Do NOT stop abruptly; taper gradually to avoid rebound hypertension
Attribute
NAMS 2023 Status
- Value
- Not recommended (other options more effective with fewer side effects)
Overview / What Is Clonidine for Menopause?
The Basics
Clonidine is a blood pressure medication that has been used for decades as an off-label option for reducing hot flashes in menopausal women. Originally developed and approved for treating high blood pressure in 1974, clinicians noticed that it could also dampen the frequency and intensity of hot flashes, and it gradually became one of the first non-hormonal alternatives offered to women who could not or chose not to use hormone replacement therapy.
Understanding where clonidine fits in the current menopause treatment landscape is important. It is not a first-line treatment. Hormone therapy remains the most effective option for vasomotor symptoms, and among non-hormonal alternatives, newer agents such as fezolinetant (Veozah), SSRIs, SNRIs, and gabapentin have all demonstrated greater efficacy with more manageable side effect profiles. The 2023 position statement from The Menopause Society (formerly NAMS) explicitly does not recommend clonidine for vasomotor symptoms, citing inferior efficacy and more problematic side effects compared to alternatives [1].
That said, clonidine still occupies a niche role. In the UK, it holds one of the few non-hormonal licenses for menopausal vasomotor symptoms (as Dixarit). Some women find it effective when other non-hormonal options have failed or are contraindicated. And for women who also have elevated blood pressure, the antihypertensive effect can serve double duty. The clinical reality is that menopausal symptom management is deeply individual, and a medication that works poorly on average can still be the right answer for a particular person.
The Science
Clonidine hydrochloride (2-(2,6-dichlorophenylamino)-2-imidazoline hydrochloride) is an imidazoline derivative with selective central alpha-2 adrenergic agonist activity, displaying approximately 200:1 selectivity for alpha-2 over alpha-1 receptors [2]. First approved by the FDA in 1974 for hypertension, its application to menopausal vasomotor symptoms emerged from clinical observations that the medication reduced sympathetic nervous system overactivity, a component of the hot flash cascade [3].
A 2006 systematic review and meta-analysis of nonhormonal therapies for menopausal hot flashes (Nelson et al., JAMA) identified 10 clinical trials of clonidine from 4,249 screened abstracts. Meta-analysis of 4 qualifying trials demonstrated a mean reduction of 0.95 daily hot flashes compared with placebo (95% CI: -1.44 to -0.47). For context, SSRIs/SNRIs showed a mean reduction of 1.13 (95% CI: -1.70 to -0.57) and gabapentin 2.05 (95% CI: -2.80 to -1.30) in the same meta-analysis [4].
The NAMS 2023 nonhormone therapy position statement classified clonidine as "not recommended" based on Levels I-III evidence, noting that it is "modestly more beneficial than placebo but less beneficial than SSRIs, SNRIs, and gabapentin in reducing VMS" and "used infrequently because of adverse effects" [1]. In contrast, the British Menopause Society acknowledges its UK licensing status while noting the "contradictory" evidence base and recommending cessation if no benefit is observed after four weeks [5].
Medical / Chemical Identity
Property
Generic Name
- Value
- Clonidine hydrochloride
Property
Chemical Class
- Value
- Imidazoline derivative; centrally acting alpha-2 adrenergic agonist
Property
Molecular Formula
- Value
- C9H9Cl2N3·HCl
Property
Molecular Weight
- Value
- 266.56 g/mol
Property
CAS Number
- Value
- 4205-91-8
Property
Appearance
- Value
- Odorless, bitter, white crystalline substance
Property
Solubility
- Value
- Soluble in water and alcohol
Property
Drug Class
- Value
- Antihypertensive (centrally acting)
Property
FDA Initial Approval
- Value
- 1974
Property
NDA Number
- Value
- NDA022500 (extended-release)
Property
Primary Indication
- Value
- Hypertension
Property
VMS Indication
- Value
- Off-label (US, Australia); Licensed (UK as Dixarit)
Brand Names by Country:
Country
United States
- Brand(s)
- Catapres (oral IR), Catapres-TTS (transdermal), Nexiclon XR (oral ER)
- Formulations
- 0.1, 0.2, 0.3 mg tablets; 0.1, 0.2, 0.3 mg/day patches
Country
United Kingdom
- Brand(s)
- Dixarit
- Formulations
- 25 mcg tablets
Country
Australia
- Brand(s)
- Catapres, Dixarit
- Formulations
- Oral tablets
Country
Canada
- Brand(s)
- Dixarit, Catapres
- Formulations
- Oral tablets, transdermal
Country
European Union
- Brand(s)
- Various generic names
- Formulations
- Oral, transdermal
Note: The US formulations are dosed in milligrams (0.1 mg = 100 mcg), while UK/Australian formulations (Dixarit) are typically dosed in micrograms (25 mcg, 50 mcg). This difference in nomenclature can be confusing. 25 mcg = 0.025 mg.
Mechanism of Action
The Basics
To understand how clonidine might reduce hot flashes, it helps to know what causes them. During menopause, declining estrogen levels disrupt your body's internal thermostat, which is located in a part of the brain called the hypothalamus. Normally, your body tolerates small fluctuations in core temperature without triggering a cooling response. In menopause, the tolerance zone narrows dramatically, meaning even tiny increases in core temperature can trigger a full-blown hot flash: blood vessels dilate, sweating begins, and your heart rate increases as your body attempts to dump heat it doesn't actually need to lose.
This process is driven partly by the sympathetic nervous system, the same "fight or flight" system that raises your heart rate during stress. Clonidine works by turning down the volume on that system. It stimulates alpha-2 receptors in the brain stem, which sends a signal to reduce the overall output of the sympathetic nervous system. With less sympathetic activity, the threshold for triggering a hot flash rises, and when flashes do occur, they may be less intense.
This is fundamentally different from how hormone therapy works. HRT restores estrogen, which widens the thermostat's tolerance zone back toward normal. Clonidine does not address the estrogen deficiency itself; it works downstream, dampening the nervous system's overreaction to that deficiency. This is why its effects tend to be more modest than HRT and why it does not address the many other symptoms of menopause that stem from estrogen loss, such as vaginal dryness, bone loss, or genitourinary changes.
The Science
Clonidine is an imidazoline derivative that functions as a selective central alpha-2 adrenergic agonist. In the nucleus tractus solitarii, it excites an inhibitory pathway that suppresses excitatory cardiovascular neurons. In the posterior hypothalamus and medulla, it reduces sympathetic outflow from the central nervous system, leading to decreased peripheral vascular resistance, reduced heart rate, and lower blood pressure [2][6].
The mechanism by which clonidine reduces vasomotor symptoms is thought to involve two complementary pathways. First, central alpha-2 stimulation reduces sympathetic nervous system tone, which is elevated during hot flashes. Norepinephrine and epinephrine levels decrease, blunting the peripheral vasodilation and sweating response. Second, clonidine may partially stabilize the thermoregulatory set point in the hypothalamic preoptic area, though this effect is less pronounced than what estrogen replacement achieves [3].
In menopausal women, the thermoneutral zone in the hypothalamic preoptic area narrows from approximately 0.4 degrees Celsius to nearly zero, meaning minimal core temperature fluctuations trigger inappropriate heat dissipation responses [7]. While estrogen replacement widens this zone back toward normal thresholds, clonidine's sympatholytic action modulates the downstream response without directly addressing the narrowed thermoneutral zone. This mechanistic distinction likely explains both the modest average efficacy and the observation that clonidine reduces hot flash intensity more consistently than it reduces frequency [4].
Clonidine also interacts with imidazoline receptors (I1 subtype) in the ventrolateral medulla, which may contribute to its hypotensive effects independently of alpha-2 agonism [2]. The clinical relevance of I1 receptor activation for vasomotor symptom control is not established.
Pathway & System Visualization
Pharmacokinetics / Hormone Physiology
The Basics
Clonidine is available in several forms, and how you take it matters for both effectiveness and side effects.
When swallowed as an immediate-release tablet, clonidine is absorbed quickly and starts working within 30 to 60 minutes, with peak effects occurring 2 to 4 hours later. The effects of each dose last roughly 6 to 8 hours, which is why most prescribers recommend taking it twice daily. Extended-release tablets are absorbed more slowly, peaking at 4 to 7 hours, and can be taken once daily.
The transdermal patch (Catapres-TTS) delivers clonidine through the skin at a steady rate over 7 days. It takes 2 to 3 days to reach peak levels after applying a new patch. While the patch avoids the peaks and troughs of oral dosing and tends to produce fewer side effects like drowsiness and dry mouth, it can cause skin irritation at the application site.
About half of each dose is processed by the liver, and 40-60% is eliminated through the kidneys unchanged. For women with kidney problems, clonidine stays in the body longer (the half-life can double or triple), so lower doses and slower titration are advisable. Clonidine passes through the blood-brain barrier readily because of its fat-soluble nature, which is why it can cause drowsiness and affects brain function.
The Science
Absorption: Oral immediate-release clonidine is rapidly and almost completely absorbed, with peak plasma concentrations (Tmax) at 3-5 hours. Extended-release tablets demonstrate delayed absorption with Tmax at 4-7 hours; for the 0.17 mg ER tablet, mean peak concentration is 0.49 (±0.09) ng/mL [8]. Transdermal systems achieve steady-state delivery with Tmax at 2-3 days; the 0.1, 0.2, and 0.3 mg/day systems use 4.33, 8.67, and 13 cm2 patches respectively [8].
Distribution: Volume of distribution is 2.1 (±0.4) L/kg. Clonidine is highly lipophilic, crossing the blood-brain barrier readily. Plasma protein binding is 20-40%, relatively low compared to many drugs [6].
Metabolism: Approximately 50% of the absorbed dose undergoes hepatic metabolism. CYP2D6 plays a predominant role in nonrenal clearance via 4-hydroxylation. Enterohepatic recirculation has been documented. Pregnancy-related increases in CYP2D6 activity accelerate clearance [9][10].
Elimination: 40-60% of the absorbed dose is recovered as unchanged drug in the urine within 24 hours. Half-life ranges from 6-20 hours in patients with normal renal function and extends to 17-41 hours with severe renal impairment [6][8].
Parameter
Tmax
- Oral IR
- 3-5 hours
- Oral ER
- 4-7 hours
- Transdermal
- 2-3 days
Parameter
Half-life
- Oral IR
- 6-20 hours
- Oral ER
- 13.7 (±3.0) hours
- Transdermal
- ~20 hours (after removal)
Parameter
Bioavailability
- Oral IR
- ~75-95%
- Oral ER
- Comparable to IR
- Transdermal
- ~60%
Parameter
Duration of effect
- Oral IR
- 6-8 hours
- Oral ER
- ~24 hours
- Transdermal
- 7 days
Parameter
Protein binding
- Oral IR
- 20-40%
- Oral ER
- 20-40%
- Transdermal
- 20-40%
Research & Clinical Evidence
The Basics
The research on clonidine for menopausal hot flashes goes back to the late 1970s, making it one of the longest-studied non-hormonal options. However, the cumulative evidence tells a nuanced story: clonidine works better than a placebo for hot flashes, but not by as much as several other available medications, and its side effects limit its usefulness for many women.
The largest analysis of the evidence (a meta-analysis published in JAMA in 2006) pooled data from multiple clinical trials and found that clonidine reduced daily hot flashes by about one per day compared to placebo. To put that in perspective, SSRIs and SNRIs reduced hot flashes by a bit more, and gabapentin reduced them by about two per day in the same analysis. All of these are substantially less effective than hormone therapy, which can reduce hot flashes by 75-90% [4].
One area where clonidine may have particular relevance is for women who have had breast cancer. A study of oral clonidine in breast cancer patients experiencing tamoxifen-induced hot flashes found significant reductions in hot flash frequency compared to placebo. Since some SSRIs (particularly paroxetine and fluoxetine) can interfere with tamoxifen metabolism through CYP2D6 inhibition, clonidine represents a non-interacting alternative for this specific population [11][12].
A head-to-head comparison of venlafaxine and clonidine in 60 breast cancer patients found them equally but moderately effective, with about a 50-55% reduction in hot flash scores. Importantly, more patients discontinued venlafaxine due to side effects than clonidine in that study [13].
The Science
Meta-analytic evidence: Nelson et al. (JAMA 2006) conducted a systematic review identifying 10 trials of clonidine from 4,249 screened abstracts. Meta-analysis of 4 qualifying trials demonstrated a mean difference of -0.95 daily hot flashes (95% CI: -1.44 to -0.47) versus placebo. Comparator analyses in the same review: SSRIs/SNRIs -1.13 (95% CI: -1.70 to -0.57); gabapentin -2.05 (95% CI: -2.80 to -1.30) [4].
Breast cancer population evidence: Pandya et al. (Ann Intern Med 2000) conducted a placebo-controlled study of oral clonidine 0.1 mg daily in postmenopausal breast cancer patients experiencing tamoxifen-induced hot flashes. Clonidine significantly reduced hot flash frequency and severity compared to placebo [11]. The Cochrane review by Rada et al. (2010) examined non-hormonal interventions for hot flashes in breast cancer survivors, including clonidine, confirming modest but statistically significant benefit [14].
Head-to-head comparison: Buijs et al. (2008) conducted a double-blind, randomized crossover study in 60 breast cancer patients comparing venlafaxine and clonidine for 8 weeks each. Median reduction in hot flash score: venlafaxine 49%, clonidine 55% (not statistically different). Premature discontinuation for toxicity was more common with venlafaxine (14/59 vs 5/53, p=0.038) [13].
Guideline positioning:
Guideline
NAMS Nonhormone Therapy
- Year
- 2023
- Recommendation
- Not recommended (Levels I-III)
Guideline
BMS Consensus
- Year
- 2025
- Recommendation
- Licensed in UK; contradictory evidence; stop if no benefit after 4 weeks
Guideline
ACOG
- Year
- 2014
- Recommendation
- Listed as effective nonhormonal alternative
Guideline
Endocrine Society
- Year
- 2015
- Recommendation
- Trial suggested for women not candidates for HRT
Guideline
Australasian Menopause Society
- Year
- Current
- Recommendation
- No longer recommended
Guideline
ASCO
- Year
- Current
- Recommendation
- May be offered for cancer-related VMS if HRT contraindicated
Evidence & Effectiveness Matrix
The following matrix uses the 20 HRT symptom/outcome categories to evaluate clonidine's evidence base. Because clonidine is a non-hormonal agent that does not address estrogen deficiency, most categories are not applicable. The Evidence Strength score reflects KB source quality. The Reported Effectiveness score reflects community sentiment data.
Category
Vasomotor Symptoms
- Evidence Strength
- 6/10
- Reported Effectiveness
- 7/10
- Summary
- Meta-analysis shows modest efficacy (~1 fewer hot flash/day vs placebo). Community reports are bimodal: dramatic responders and non-responders. Less effective than SSRIs/SNRIs, gabapentin, and NK3R antagonists.
Category
Sleep Quality
- Evidence Strength
- 3/10
- Reported Effectiveness
- 7/10
- Summary
- No dedicated RCTs on sleep outcomes. Sedative properties may secondarily improve sleep at low doses, though higher doses paradoxically disrupt sleep in 50%+ of users (BMS). Community reports are strongly positive for sleep benefit at bedtime dosing.
Category
Anxiety & Stress Response
- Evidence Strength
- 3/10
- Reported Effectiveness
- 6/10
- Summary
- Limited formal evidence for anxiolysis in menopause context. Central sympatholytic mechanism plausibly reduces anxiety. Community reports favorable for physical anxiety symptoms. Off-label use for anxiety is documented.
Category
Mood & Emotional Wellbeing
- Evidence Strength
- 2/10
- Reported Effectiveness
- 4/10
- Summary
- Insufficient menopause-specific evidence. Depression listed as rare adverse effect. Community reports are mixed: some improvement, some worsening.
Category
Energy & Fatigue
- Evidence Strength
- 2/10
- Reported Effectiveness
- 3/10
- Summary
- Drowsiness and sedation are among the most common adverse effects (~33%). Community consistently reports fatigue as a significant limitation.
Category
Cardiovascular Health
- Evidence Strength
- 4/10
- Reported Effectiveness
- 4/10
- Summary
- Established antihypertensive; lowers BP and heart rate. Potentially beneficial for hypertensive menopausal women. Harmful for hypotensive women. Not studied for cardiovascular outcomes in menopause specifically.
Categories Not Scored (insufficient data or not applicable):
Cognitive Function, Sexual Function & Libido, Genitourinary Health (GSM), Bone Health & Osteoporosis, Metabolic Health & Insulin Sensitivity, Body Composition & Weight, Joint & Musculoskeletal Health, Skin, Hair & Appearance, Headache & Migraine, Breast Cancer Risk, Endometrial Safety, Thrombotic Risk, Menstrual & Reproductive, Other Physical Symptoms
Note: Unlike hormonal therapies that address multiple estrogen-deficiency symptoms simultaneously, clonidine's therapeutic scope is narrow, targeting primarily vasomotor symptoms through sympathetic nervous system modulation. It does not address the underlying hormonal deficiency.
Benefits & Therapeutic Effects
The Basics
Clonidine's benefits for menopausal symptoms are focused primarily on hot flashes and night sweats. For some women, this is enough to make a meaningful difference in daily quality of life. The reality is that hot flashes are not just a minor inconvenience for many people. They can disrupt sleep, impair concentration at work, cause embarrassment in social situations, and create a persistent sense of dread about when the next one will strike.
When clonidine works, it can reduce the frequency of hot flashes meaningfully. Clinical evidence suggests an average reduction of about one fewer hot flash per day compared to placebo, though individual responses vary widely. Some women report near-complete resolution; others notice little change. Community reviews on medication platforms reflect this variability, with average ratings of 7 out of 10 and a telling bimodal distribution (many perfect scores alongside many very low ones).
Beyond hot flash reduction, clonidine offers several potential secondary benefits. Its calming effect on the sympathetic nervous system can reduce the heart-pounding, anxiety-like sensation that accompanies many hot flashes. For women who also have elevated blood pressure, clonidine addresses two issues with one medication. And its sedating properties, while often listed as a side effect, can be leveraged therapeutically by timing the dose at bedtime, helping women who struggle with sleep disruption.
It is important to be clear about what clonidine does not do. It does not restore estrogen. It does not protect bone density, improve vaginal health, support cardiovascular protection, or address the many other consequences of estrogen decline. For women whose primary and dominant complaint is severe hot flashes, and who cannot use other treatments, clonidine can be a reasonable option. For broader menopausal symptom management, its narrow therapeutic scope is a significant limitation.
The Science
The primary demonstrated benefit of clonidine in the menopausal context is reduction of vasomotor symptom frequency and severity. The Nelson et al. meta-analysis (2006) quantified this as a mean reduction of 0.95 daily hot flashes versus placebo (95% CI: -1.44 to -0.47) [4]. The absolute magnitude of benefit is modest compared to estrogen therapy (which reduces hot flash frequency by 75-90%) and to other nonhormonal alternatives: the same meta-analysis found gabapentin produced a 2.05 reduction and SSRIs/SNRIs a 1.13 reduction [4].
In breast cancer populations, Pandya et al. (2000) demonstrated significant hot flash frequency reduction with oral clonidine 0.1 mg daily in women with tamoxifen-induced vasomotor symptoms [11]. The Buijs et al. (2008) crossover study found clonidine and venlafaxine equally effective (55% vs 49% reduction in hot flash score, respectively) in breast cancer patients, with better tolerability for clonidine [13].
Secondary benefits reported in clinical practice and community data include: (a) anxiolytic effects via central sympatholysis, reducing the "sense of doom" and palpitations that accompany hot flashes; (b) sleep facilitation at low doses due to sedative properties; (c) antihypertensive effects beneficial for the estimated 30-40% of menopausal women with elevated blood pressure [2][6].
Risks, Side Effects & Safety
The Basics
Understanding clonidine's side effects is especially important because they represent the main reason it has fallen out of favor compared to newer non-hormonal alternatives. Most side effects are related to its fundamental mechanism: by calming the sympathetic nervous system, it can calm things too much, leading to drowsiness, low blood pressure, and slowed reflexes.
Common side effects that affect many users include dry mouth (roughly 40% of users), drowsiness (about 33%), dizziness (about 16%), constipation (about 10%), and sedation (about 10%). These effects are dose-related, meaning lower doses produce fewer problems. Many women find that the drowsiness improves after the first few weeks as the body adjusts, but it remains a significant barrier for some.
The single most important safety concern with clonidine is what happens when you stop taking it. Unlike most medications, you must never stop clonidine abruptly. Sudden discontinuation can cause rebound hypertension: your blood pressure can spike dramatically, accompanied by nervousness, agitation, headache, and tremor. In rare cases, this has led to hypertensive encephalopathy, stroke, and death. This is not a theoretical risk; it is well-documented. Any plan to stop clonidine must involve a gradual taper over at least 2-4 days, and longer tapers are advisable for those on higher doses or who have been using it for an extended period. If you are also taking a beta-blocker, the beta-blocker should be discontinued several days before tapering clonidine to avoid dangerous blood pressure spikes.
Blood pressure effects deserve careful consideration. Clonidine lowers blood pressure. For women with elevated blood pressure, this is beneficial. For women with normal or low blood pressure, it can cause problematic lightheadedness, especially when standing up quickly (orthostatic hypotension). Women with a baseline blood pressure below about 110/70 should discuss this risk carefully with their prescriber.
Less common but notable effects include bradycardia (slow heart rate), depression (rare but documented with chronic use), sexual dysfunction, and weight gain. Heart rhythm disturbances such as AV block have been reported, particularly when combined with other heart rate-slowing medications.
The Science
Common adverse effects (from DailyMed prescribing information, immediate-release formulation data) [8]:
- Xerostomia: ~40%
- Somnolence: ~33%
- Dizziness: ~16%
- Constipation: ~10%
- Sedation: ~10%
Serious adverse effects:
- Withdrawal syndrome/rebound hypertension: Well-documented; sudden cessation results in elevated catecholamine concentrations with symptoms including nervousness, agitation, headache, tremor, and rapid blood pressure rise. Rare instances of hypertensive encephalopathy, cerebrovascular accidents, and death have been reported [6][8]. Risk is increased with higher doses and concomitant beta-blocker therapy.
- Cardiovascular: Bradycardia, AV block (sinus node arrest, junctional bradycardia, high-degree AV block reported). Congestive heart failure and Raynaud's phenomenon reported rarely [8].
- CNS depression: Dose-dependent sedation, which may impair driving and machinery operation. Potentiated by alcohol, barbiturates, and other CNS depressants [8].
- Depression: Rare but clinically significant adverse effect with chronic use; progressive onset may make early detection difficult [6].
Sleep disturbance at higher doses: The BMS consensus statement notes that at higher doses, clonidine causes sleep disturbance in at least 50% of users [5]. This is paradoxical given the sedative properties at lower doses and highlights the importance of dose-response relationships in clinical practice.
Comparator risk context: Clonidine's adverse effect profile is qualitatively different from other non-hormonal VMS treatments. SSRIs/SNRIs carry risks of nausea, sexual dysfunction, and serotonin syndrome but do not pose withdrawal hypertensive crises. Gabapentin causes dizziness and somnolence but without cardiovascular effects. Fezolinetant has minimal side effects but requires liver function monitoring. The NAMS 2023 position statement's decision not to recommend clonidine reflects this unfavorable risk-benefit ratio compared to available alternatives [1].
Contraindications:
- Absolute: Hypersensitivity to clonidine
- Relative: Significant bradycardia, AV conduction defects, hypotension, severe coronary insufficiency, recent myocardial infarction, cerebrovascular disease
Being informed about potential risks is important. Being able to track and document any side effects you actually experience is what turns awareness into safety. Doserly lets you log side effects as they happen, with timestamps and severity ratings, so nothing falls through the cracks between appointments.
If you're experiencing breakthrough bleeding, headaches, breast tenderness, or any other change, having a documented timeline helps your provider distinguish between expected adjustment effects and signals that warrant a protocol change. The app also checks for interactions between your HRT and any other medications or supplements you're taking.
Connect protocol changes to labs and health markers.
Doserly can keep lab results, biomarkers, symptoms, and dose history close together so follow-up conversations have better context.
Insights
Labs and trends
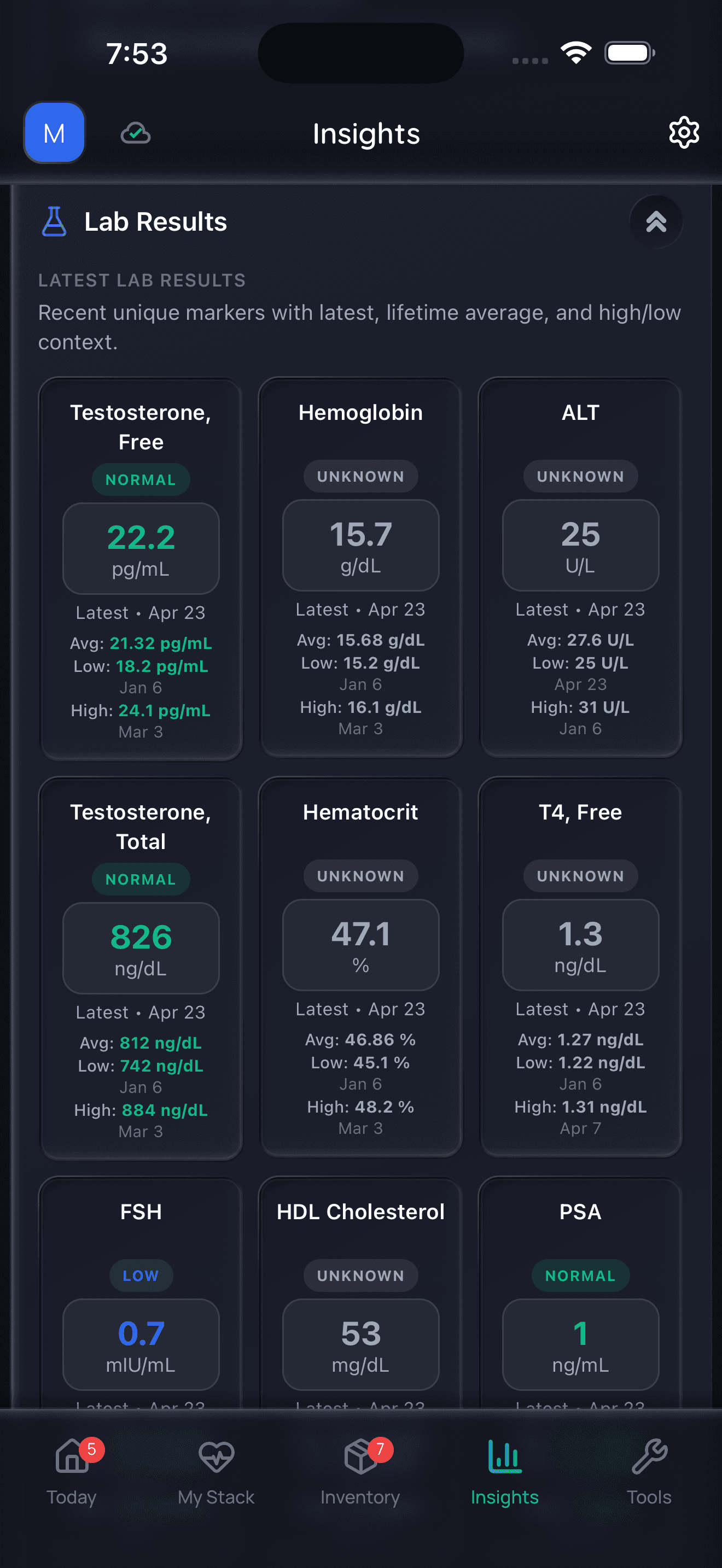
Doserly organizes data; it does not diagnose or interpret labs for you.
Dosing & Treatment Protocols
The Basics
Clonidine dosing for menopausal hot flashes is different from its dosing for high blood pressure, and the approach varies between countries. In general, the doses used for hot flashes are substantially lower than those used for blood pressure management.
In the UK, where Dixarit is licensed specifically for menopausal flushing, the typical starting dose is 25 micrograms (mcg) twice daily for two weeks, then increased to a maximum of 50 mcg three times daily if needed. That is a total daily dose of 50-150 mcg. The BMS recommends stopping if there is no benefit after four weeks [5].
In the US, where clonidine use for hot flashes is off-label, clinicians commonly prescribe 0.05 mg (50 mcg) twice daily or a total of 0.1 mg (100 mcg) daily, using immediate-release tablets. Alternatively, the 0.1 mg/day transdermal patch applied weekly is used. Some providers start lower (0.025 mg twice daily) and titrate up [15].
Key dosing principles:
- Start low. Begin at the lowest available dose to minimize side effects, especially drowsiness and blood pressure reduction.
- Titrate slowly. Increase at intervals of no less than one to two weeks, guided by symptom response and tolerability.
- Time strategically. Many prescribers recommend the larger dose (or the full dose) at bedtime, leveraging the sedative effect for sleep benefit while minimizing daytime drowsiness.
- Consider the patch. The transdermal formulation provides steadier drug levels and may cause fewer peaks-and-troughs-related side effects. It is changed weekly.
- Set a trial period. If no meaningful improvement is seen after four weeks at an adequate dose, continuing clonidine is unlikely to be worthwhile.
- Never stop abruptly. When discontinuing, taper the dose gradually over at least 2-4 days, longer for higher doses or prolonged use.
These dosing ranges represent commonly prescribed protocols in clinical practice and should not be interpreted as specific treatment recommendations. Dosing decisions should be made in consultation with a prescribing clinician who can account for individual factors.
The Science
Dosing for vasomotor symptoms (off-label in most jurisdictions):
Route
Oral IR
- Starting Dose
- 0.025-0.05 mg twice daily
- Maintenance Range
- 0.05-0.1 mg twice daily
- Maximum
- 0.15 mg twice daily
Route
Oral ER
- Starting Dose
- 0.1 mg once daily at bedtime
- Maintenance Range
- 0.1-0.2 mg once daily
- Maximum
- Per clinical judgment
Route
Transdermal
- Starting Dose
- 0.1 mg/24 hours weekly
- Maintenance Range
- 0.1 mg/24 hours weekly
- Maximum
- 0.2 mg/24 hours
For context, hypertension dosing typically ranges from 0.1-0.6 mg/day orally, with the extended-release formulation studied at 0.17-0.52 mg once daily [8]. VMS doses are generally at the lower end of this range.
Dose equivalency (IR to ER conversion): 0.1 mg IR twice daily ≈ 0.17 mg ER once daily; 0.2 mg IR twice daily ≈ 0.34 mg ER once daily [8].
Special populations:
- Renal impairment: Initiate at lower dose with slower titration. Half-life may extend to 41 hours in severe impairment. Minimal removal by hemodialysis [8].
- Geriatric patients: AGS Beers Criteria lists clonidine as potentially inappropriate for older adults due to CNS adverse effects. Lower starting doses recommended [6].
- Hepatic impairment: No specific dosage adjustment provided in prescribing information [8].
Getting the dosing right often takes time and fine-tuning with your provider. Keeping an accurate record of what you're actually taking, doses, timing, and any adjustments, makes that process smoother. Doserly tracks your HRT doses alongside everything else in your health stack, so your full protocol is always in one place.
Never wonder whether you took your morning dose or when you last changed your patch. The app logs every dose with a timestamp and sends reminders when your next one is due, helping you maintain the consistency that makes hormone therapy most effective.
Turn symptom and safety notes into a clearer timeline.
Doserly helps you log doses, symptoms, and safety observations side by side so patterns are easier to discuss with a qualified clinician.
Pattern view
Logs and observations

Pattern visibility is informational and should be reviewed with a clinician.
What to Expect (Timeline)
Starting clonidine for menopausal hot flashes involves a period of adjustment. Here is a general timeline based on clinical evidence and community experience. Individual responses vary substantially.
Days 1-3: The sedating effects are typically most pronounced in the first few days. Many women feel drowsy, lightheaded, or foggy. Dry mouth often begins immediately. Some women notice an improvement in hot flashes within the first few days, but for others it takes longer. Blood pressure may decrease, which is felt as lightheadedness on standing.
Days 4-14: Side effects often begin to diminish as the body adjusts. If starting at a low dose, your prescriber may increase the dose at the one or two week mark if hot flashes have not improved adequately. Sleep may improve during this period, especially if the dose is taken at bedtime.
Weeks 2-4: This is the key evaluation window. If clonidine is going to work for you, meaningful improvement in hot flash frequency and severity should be apparent by now. The BMS recommends stopping if there is no benefit after four weeks. Community reports suggest that women who respond well often describe significant improvement within this timeframe, while non-responders see little change.
Months 1-3: For responders, continued benefit with generally stable dosing. Side effects should have settled to their steady-state level. However, some women report a gradual decline in effectiveness over weeks to months (tolerance development), which may prompt a discussion about dose adjustment.
Months 3-6 and beyond: Ongoing monitoring of blood pressure and symptom control. Periodic reassessment of whether clonidine remains the best option as newer alternatives become available. Consider a trial of dose reduction to find the minimum effective dose.
If discontinuing: Taper gradually over at least 2-4 days. Do not stop abruptly. Hot flashes may return after stopping, sometimes with a temporary rebound intensity above pre-treatment levels due to sympathetic nervous system reactivation.
Knowing what to expect is helpful. Documenting your own journey week by week creates something even more valuable, a personal timeline that captures exactly how your treatment is unfolding. Doserly's symptom journal lets you record changes as they happen, building a detailed record from day one.
The early weeks of HRT can feel uncertain. Having a clear log of what's changing, and what hasn't shifted yet, helps you stay grounded in your actual progress rather than relying on memory. When you look back after three months, you'll see how far you've come in ways that are easy to forget without documentation.
See where a dose, cycle, or change fits in time.
Doserly gives each protocol a timeline so dose changes, pauses, restarts, and observations are easier to compare later.
Timeline
Cycle history
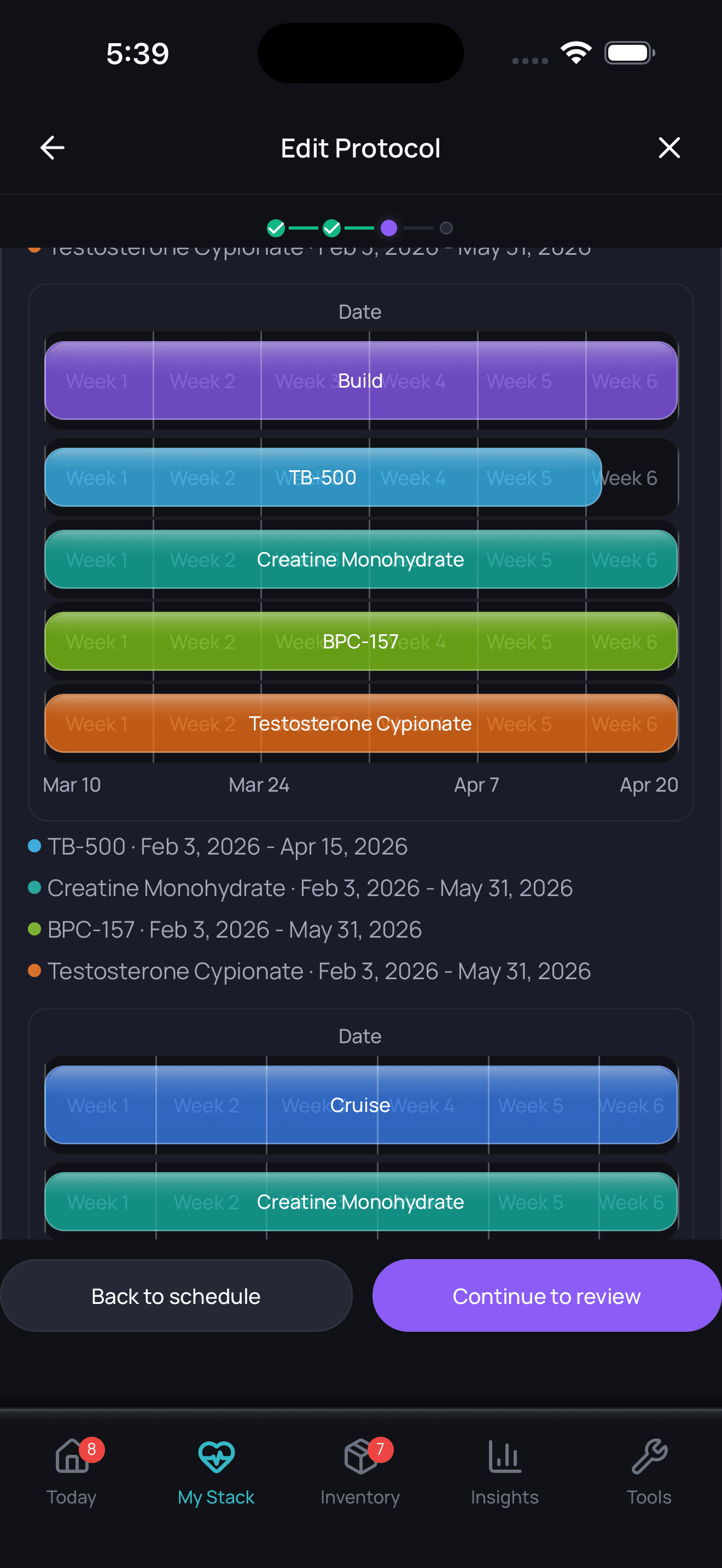
Timeline tracking helps with recall; it is not a treatment recommendation.
Timing Hypothesis & Window of Opportunity
The timing hypothesis, which suggests that HRT initiated within 10 years of menopause onset may confer cardiovascular protection while later initiation may increase risk, is a critical concept for systemic hormone therapy decision-making. However, it has limited direct relevance to clonidine.
Because clonidine is not a hormone and does not interact with estrogen receptors, it is not subject to the timing-dependent risk-benefit shifts that characterize HRT. Clonidine can be initiated at any point during or after the menopausal transition when vasomotor symptoms are problematic, without the timing considerations that influence HRT prescribing decisions.
That said, the timing hypothesis remains relevant context for women considering clonidine because it may inform the broader treatment decision. A woman within the optimal window for HRT initiation (under 60 years of age or within 10 years of menopause) who is considering clonidine should discuss with her provider whether HRT might offer superior symptom relief along with cardioprotective and bone-protective benefits. Clonidine may be more appropriate for women outside the optimal HRT window, for those with contraindications to HRT, or for those who prefer a non-hormonal approach.
Interactions & Compatibility
Clonidine has several clinically significant drug interactions that must be considered, particularly because many menopausal women are taking other medications.
Drug-Drug Interactions:
- CNS depressants (alcohol, benzodiazepines, barbiturates, opioids, sedative antihistamines): Clonidine potentiates central nervous system depression. Combined use increases sedation, respiratory depression risk, and impaired cognitive function. Women should be counseled about alcohol intake [8].
- Tricyclic antidepressants (amitriptyline, nortriptyline, imipramine): May reduce clonidine's antihypertensive effect, potentially requiring dose increases. This is a pharmacodynamic interaction at the alpha-2 receptor level [8].
- Beta-blockers (metoprolol, propranolol, atenolol): Additive effects on heart rate (bradycardia) and AV conduction. Critically, if both are used together, the beta-blocker must be discontinued first (several days before) when tapering clonidine, because unopposed alpha-adrenergic activity during clonidine withdrawal with continued beta-blockade can precipitate severe rebound hypertension [8].
- Calcium channel blockers (verapamil, diltiazem): Additive effects on heart rate and conduction. Sinus bradycardia requiring hospitalization and pacemaker insertion has been reported with concurrent clonidine and diltiazem/verapamil [8].
- Digitalis (digoxin): Additive bradycardic effects [8].
- SSRIs/SNRIs: No significant pharmacokinetic interaction. Clonidine and SSRIs/SNRIs are sometimes used together, though additive sedation may occur. Notably, clonidine does not inhibit CYP2D6 and does not interact with tamoxifen metabolism, which is a potential advantage over paroxetine and fluoxetine for breast cancer patients [12].
- Gabapentin: No known significant interaction. May be used concurrently, though additive sedation is possible.
Supplement Interactions:
- Melatonin: Additive sedation; timing at bedtime may amplify drowsiness (may be desirable or excessive depending on the individual)
- Valerian, kava, passionflower: Additive CNS depression
- St. John's Wort: May reduce clonidine levels through CYP enzyme induction
Lifestyle Factors:
- Alcohol: Significant additive sedation. Extended-release formulation may release drug faster in the presence of high alcohol concentrations [8]
- Driving and machinery operation: Clonidine may impair alertness, especially during dose initiation or increases
Cross-links to related guides:
- Gabapentin for Menopause (frequently used alternative non-hormonal agent)
- Paroxetine Low-Dose (Brisdelle) (FDA-approved non-hormonal option)
- Fezolinetant (Veozah) (recommended non-hormonal alternative)
- Non-Hormonal Menopause Treatments (overview guide)
Decision-Making Framework
Deciding whether to try clonidine for menopausal vasomotor symptoms involves weighing its modest benefits against its side effects and the availability of alternatives. This is a conversation to have with a healthcare provider who can assess your individual situation.
Clonidine may be worth considering if:
- You have tried or cannot tolerate SSRIs, SNRIs, gabapentin, and fezolinetant
- You have breast cancer and are taking tamoxifen (clonidine does not interact with tamoxifen metabolism, unlike some SSRIs)
- You also have elevated blood pressure that could benefit from treatment
- You prefer a non-hormonal option and have exhausted other recommended alternatives
- Your primary complaint is hot flashes with associated anxiety and sleep disruption
Clonidine may not be the best choice if:
- You have normal or low blood pressure (risk of hypotension and orthostatic symptoms)
- You need daytime alertness (sedation is a major limitation)
- You have bradycardia or heart conduction disorders
- You are taking beta-blockers (withdrawal risk amplified)
- You have a history of depression (rare but documented worsening)
- You want comprehensive menopausal symptom relief (clonidine only addresses vasomotor symptoms)
Questions to discuss with your provider:
- "Given that NAMS does not recommend clonidine, what is the specific reason you are suggesting it for me?"
- "Have I tried the recommended non-hormonal alternatives first?"
- "What is my blood pressure baseline, and how will we monitor for hypotension?"
- "What is the plan for tapering if I decide to stop?"
- "Is there a reason I cannot use hormone therapy, which is more effective?"
Finding a menopause specialist: If your current provider is unfamiliar with the range of non-hormonal options, consider seeking a NAMS Certified Menopause Practitioner (searchable at menopause.org) who can provide a comprehensive assessment.
Administration & Practical Guide
Oral Tablets (Immediate-Release):
- Take with or without food
- Take at consistent times each day (typically morning and bedtime, or bedtime only if using full dose at night)
- Swallow whole with water
- If a dose is missed, take it as soon as remembered unless it is close to the next dose. Never double up.
- Keep a consistent supply; running out can lead to abrupt withdrawal
Extended-Release Tablets:
- Swallow whole; do not crush, chew, or split
- Take at bedtime for optimal tolerability
- Not interchangeable milligram-for-milligram with immediate-release
Transdermal Patch (Catapres-TTS):
- Apply to a clean, dry, hairless area of the upper arm or chest
- Rotate application sites to avoid skin irritation
- Change the patch every 7 days on the same day each week
- If the patch loosens, apply adhesive overlay or replace it
- After removal, fold the patch in half with the sticky side together and dispose safely
- Leaving the old patch on for 24 hours after placing a new one may provide smoother coverage during the transition (per some clinical practice)
When converting from oral to transdermal:
- Day 1: Apply transdermal patch + full oral dose
- Day 2: Apply patch + 50% oral dose
- Day 3: Apply patch + 25% oral dose
- Day 4: Patch only (oral discontinued)
Storage: Room temperature (20-25 degrees C / 68-77 degrees F). Protect from light.
Monitoring & Lab Work
Because clonidine is used off-label for menopausal symptoms and acts primarily on blood pressure and heart rate, monitoring is focused on cardiovascular parameters rather than hormone levels.
Before starting clonidine:
- Baseline blood pressure and resting heart rate
- Review of current medications for interactions (especially beta-blockers, calcium channel blockers, CNS depressants)
- Assessment of renal function (creatinine, GFR) since renal impairment prolongs half-life
- Cardiac history review (AV block, bradycardia, heart failure)
Initial follow-up (1-4 weeks):
- Blood pressure check (seated and standing, to assess for orthostatic hypotension)
- Heart rate assessment
- Side effect evaluation (drowsiness, dry mouth, dizziness)
- Hot flash frequency assessment (symptom diary recommended)
- Decision point at 4 weeks: continue or discontinue per BMS guidance
Ongoing monitoring:
- Blood pressure at each visit
- Periodic assessment of hot flash control
- Screening for depression symptoms (rare but documented with chronic use)
- Annual review of whether clonidine remains the appropriate treatment
- Renal function monitoring if baseline impairment exists
No routine hormone level monitoring is required for clonidine use, as it does not affect estrogen, progesterone, FSH, or other reproductive hormones.
Complementary Approaches & Lifestyle
Clonidine's narrow therapeutic scope (primarily vasomotor symptoms) means that complementary strategies are especially important for addressing the broader constellation of menopausal symptoms.
Evidence-based complementary strategies:
- Cognitive-behavioral therapy (CBT): Recommended by NAMS (Level I evidence) for vasomotor symptoms. Can be combined with clonidine for additive benefit on hot flash perception and coping [1].
- Clinical hypnosis: Also recommended by NAMS (Level I evidence). Studies show reduction in hot flash frequency and improvement in sleep.
- Exercise: Regular physical activity (both aerobic and resistance training) supports cardiovascular health, bone density, mood, and sleep quality. While exercise alone may not significantly reduce hot flash frequency, it supports overall menopausal wellbeing.
- Weight management: Weight loss is recommended by NAMS (Levels II-III evidence) for VMS reduction. Higher BMI is associated with more severe vasomotor symptoms.
- Temperature management: Layered clothing, cooling fans, cool drinks, and cooler bedroom temperatures can reduce hot flash triggers.
- Stress management: Mind-body practices including meditation, yoga (though not NAMS-recommended specifically for VMS), and deep breathing may reduce the perceived impact of hot flashes.
Supplements with limited evidence:
- Black cohosh: Some studies show modest benefit for hot flash reduction, though evidence is inconsistent. Not recommended for breast cancer patients due to possible estrogenic activity.
- Phytoestrogens (soy isoflavones): Mixed evidence; not recommended by NAMS [1].
Important note: If you are taking clonidine, avoid supplements that may additively lower blood pressure or cause sedation, including high-dose magnesium, valerian, and kava.
Cross-links: Menopause Nutrition & Lifestyle
Stopping HRT / Discontinuation
Discontinuing clonidine requires more care than stopping most medications. The withdrawal risk is the single most important safety consideration in the entire clonidine treatment course.
Why tapering is essential:
Clonidine suppresses sympathetic nervous system output. When it is removed abruptly, the sympathetic system rebounds with a surge of catecholamine release. This produces rapid blood pressure elevation, often above pre-treatment levels, along with nervousness, agitation, headache, tremor, and potentially life-threatening hypertensive crises. Rare but documented consequences include hypertensive encephalopathy, stroke, and death [6][8].
Recommended tapering approach:
- Oral formulations: Reduce dose gradually over 2-4 days minimum. For those on higher doses or longer treatment courses, taper over 1-2 weeks.
- Transdermal patches: Remove the current patch and monitor blood pressure closely for several days. Consider transitioning to a low-dose oral regimen and tapering from there if blood pressure rises.
- If also taking a beta-blocker: Discontinue the beta-blocker several days BEFORE beginning clonidine taper. This sequence is critical to avoid severe rebound hypertension.
After stopping:
- Hot flashes may return, potentially with temporarily increased intensity (rebound effect vs natural symptom recurrence)
- Monitor blood pressure for several days after the final dose
- Discuss alternative treatment options with your provider if VMS remain problematic
When to consider stopping:
- No meaningful benefit after 4 weeks at adequate dose (BMS guidance)
- Side effects outweigh benefits
- Alternative treatments have become available or appropriate
- Hot flashes have naturally diminished
Special Populations & Situations
Breast Cancer Survivors
Clonidine holds one of its strongest niches in this population. Women with breast cancer history often cannot use systemic HRT and may need to avoid SSRIs that inhibit CYP2D6 (paroxetine, fluoxetine) if taking tamoxifen. Clonidine does not interact with tamoxifen metabolism and has some evidence of efficacy in this specific population (Pandya et al., 2000). The ASCO guidelines include clonidine among options for cancer-related VMS when HRT is contraindicated [11][16].
Women with Hypertension
Clonidine may offer dual benefit in this population, addressing both elevated blood pressure and hot flashes. However, current hypertension guidelines (ACC/AHA 2017) classify clonidine as a last-line antihypertensive due to its CNS adverse effects. If blood pressure is the primary concern, more effective antihypertensives should be used, with the VMS benefit considered a secondary advantage if clonidine is already being prescribed [17].
Women with Normal or Low Blood Pressure
This population faces particular risk. Orthostatic hypotension, lightheadedness, and syncope are more likely. If clonidine is attempted, starting at the lowest possible dose with careful blood pressure monitoring is essential. Community reports consistently flag low blood pressure as a significant barrier.
Geriatric Patients
The AGS Beers Criteria lists clonidine as potentially inappropriate for older adults due to high risk of bradycardia, hypotension, and CNS effects including sedation. Falls risk is increased. Lower starting doses and cautious titration are essential [6].
Women with Depression History
Depression is a documented rare adverse effect of chronic clonidine use. Women with pre-existing depression or those in the perimenopausal depression window should be monitored carefully and should consider alternative non-hormonal options that may have antidepressant benefit (SSRIs/SNRIs) rather than a medication that could worsen mood [6].
Premature Ovarian Insufficiency (POI)
Women with POI who cannot use HRT may consider clonidine for vasomotor symptoms. However, the strong recommendation for HRT in POI (to replace missing hormones for cardiovascular and bone protection until the typical age of menopause) means clonidine should only be considered when HRT is truly contraindicated.
Regulatory, Insurance & International
United States (FDA):
- Approval status: FDA-approved for hypertension only. Use for menopausal VMS is off-label.
- Insurance coverage: Generally covered as a generic antihypertensive. Off-label use for VMS may require documentation.
- Generic availability: Widely available and inexpensive as a generic medication.
- Cost: Among the least expensive non-hormonal options. Generic clonidine IR tablets cost approximately $4-15 per month. Transdermal patches cost more ($30-80/month without insurance).
United Kingdom (MHRA):
- Approval status: Dixarit (clonidine 25 mcg) is licensed for menopausal flushing and migraine prevention.
- NHS availability: Available on NHS prescription.
- Cost: Very low cost. Available as a standard NHS prescription with standard prescription charge.
Australia (TGA):
- Approval status: Available as Catapres and Dixarit. The AMS no longer recommends clonidine for VMS.
- PBS status: Listed on PBS for hypertension. Off-label prescribing for VMS is at prescriber discretion.
Canada (Health Canada):
- Available as Dixarit and Catapres.
European Union:
- Available in various formulations across EU member states.
Frequently Asked Questions
Q: Is clonidine approved by the FDA for menopausal hot flashes?
A: No. In the United States, clonidine is FDA-approved only for hypertension. Its use for menopausal hot flashes is off-label, meaning prescribers may recommend it based on clinical evidence, but it has not gone through the FDA approval process specifically for this indication. In the UK, however, Dixarit (clonidine 25 mcg) does carry a license for menopausal flushing.
Q: How effective is clonidine compared to hormone therapy for hot flashes?
A: Substantially less effective. Hormone therapy reduces hot flash frequency by approximately 75-90%. Clinical trials show clonidine reduces hot flashes by roughly one per day more than placebo. Other non-hormonal options (gabapentin, SSRIs/SNRIs, fezolinetant) are also more effective than clonidine on average.
Q: Can I take clonidine if I have normal blood pressure?
A: It is possible, but requires careful monitoring. Clonidine lowers blood pressure regardless of whether you have hypertension. Women with normal or low blood pressure are at increased risk of lightheadedness, dizziness, and fainting, especially when standing up. Discuss this risk with your prescriber.
Q: Why did NAMS stop recommending clonidine?
A: The 2023 NAMS position statement classified clonidine as "not recommended" because other non-hormonal options (SSRIs, SNRIs, gabapentin, fezolinetant) are more effective at reducing hot flashes and have fewer adverse effects. The guideline change reflects the availability of better alternatives, not new safety concerns.
Q: Can I take clonidine if I am on tamoxifen?
A: Yes. Unlike some SSRIs (paroxetine, fluoxetine) that can interfere with tamoxifen metabolism through CYP2D6 inhibition, clonidine does not interact with tamoxifen. This makes it one of the non-hormonal options specifically suitable for breast cancer patients on tamoxifen.
Q: What happens if I stop clonidine suddenly?
A: Abrupt discontinuation can cause a dangerous rebound in blood pressure, potentially leading to hypertensive crisis. Symptoms include nervousness, agitation, headache, tremor, and rapidly rising blood pressure. In rare cases, stroke or death has occurred. Always taper clonidine gradually under medical supervision.
Q: Does clonidine help with menopausal symptoms other than hot flashes?
A: Clonidine's primary benefit is for hot flashes and night sweats. It does not address vaginal dryness, bone loss, mood changes, or other estrogen-deficiency symptoms. Some women report secondary benefits for anxiety and sleep, likely related to its sedative and anxiolytic properties.
Q: How long does it take for clonidine to work for hot flashes?
A: Some women report improvement within the first few days. The recommended evaluation period is four weeks; if there is no meaningful improvement by then, continuing is unlikely to be beneficial.
Q: Can I drink alcohol while taking clonidine?
A: Alcohol significantly increases clonidine's sedating effects and can worsen hypotension. If you drink alcohol while taking clonidine, you may experience pronounced drowsiness, dizziness, and impaired coordination. Moderation or avoidance is advisable.
Q: Is the clonidine patch better than the tablets for hot flashes?
A: The transdermal patch provides steadier drug levels and may produce fewer side effects related to peak drug concentrations (drowsiness, dry mouth). Some community users report better tolerability with the patch. However, skin irritation at the application site is a unique patch side effect.
Myth vs. Fact
Myth: Clonidine is a recommended first-line non-hormonal treatment for menopausal hot flashes.
Fact: As of the 2023 NAMS position statement, clonidine is explicitly "not recommended" for menopausal vasomotor symptoms. While it was historically considered among the non-hormonal alternatives, the availability of more effective options with better tolerability profiles (SSRIs/SNRIs, gabapentin, fezolinetant) has moved clonidine to a last-resort position [1].
Myth: Because clonidine is licensed in the UK for menopausal flushing, it must be an effective treatment.
Fact: The UK licensing of Dixarit reflects a historical regulatory decision. The evidence base is described by the BMS as "contradictory." Licensing status does not equate to current best-practice recommendations, and the Australasian Menopause Society, which had a similar regulatory context, now explicitly no longer recommends clonidine for VMS [5].
Myth: Clonidine is safer than hormone therapy because it is not a hormone.
Fact: "Non-hormonal" does not automatically mean "safer." Clonidine carries unique risks including rebound hypertensive crisis on abrupt discontinuation (potentially life-threatening), hypotension, bradycardia, sedation, and depression. HRT, when used within the appropriate timing window and with individualized risk assessment, may actually have a more favorable risk-benefit profile for many women [1].
Myth: You can stop clonidine anytime without any problems.
Fact: This is one of the most dangerous misconceptions about clonidine. Abrupt discontinuation can trigger a hypertensive crisis with symptoms including severe headache, agitation, tremor, and dangerously elevated blood pressure. Rare cases of stroke and death have been documented. Clonidine must always be tapered gradually [6][8].
Myth: If clonidine doesn't work in the first few days, it won't work at all.
Fact: While some women experience rapid improvement, the recommended evaluation period is four weeks. Side effects like drowsiness often improve during the first two weeks as the body adjusts. A medication should not be abandoned prematurely, though it should also not be continued indefinitely if it is not helping.
Myth: Clonidine is addictive.
Fact: Clonidine is not classified as a controlled substance and does not produce the euphoric effects associated with addictive medications. However, physical dependence does develop, meaning the body adapts to its presence and withdrawal symptoms (primarily rebound hypertension) occur if it is stopped suddenly. Dependence and addiction are different phenomena [6].
Myth: The clonidine patch is just as effective as oral tablets.
Fact: Limited head-to-head comparison data exists between oral and transdermal clonidine specifically for VMS. The transdermal route provides steadier plasma levels and avoids first-pass metabolism. Community reports suggest comparable or potentially better tolerability with the patch, though this has not been rigorously studied in VMS populations.
Myth: Clonidine helps with all menopausal symptoms.
Fact: Clonidine's evidence applies almost exclusively to vasomotor symptoms (hot flashes and night sweats). It does not address vaginal atrophy, bone loss, cardiovascular protection, mood disorders, cognitive changes, or any of the other widespread effects of estrogen deficiency. Women with multiple menopausal symptoms may need additional treatments alongside or instead of clonidine.
Sources & References
Clinical Guidelines
- Shufelt CL, Brown V, Carpenter JS, et al. The 2023 nonhormone therapy position statement of The North American Menopause Society. Menopause. 2023;30(6):573-590. doi:10.1097/GME.0000000000002200
- British Menopause Society. Consensus Statement: Non-hormonal-based treatments for menopausal symptoms. Reviewed November 2025. Available at: thebms.org.uk
- Runowicz CD, Leach CR, Henry NL, et al. American Cancer Society/American Society of Clinical Oncology Breast Cancer Survivorship Care Guideline. J Clin Oncol. 2016;34(6):611-635.
- Whelton PK, Carey RM, Aronow WS, et al. 2017 ACC/AHA Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults. Hypertension. 2018;71(6):e13-e115.
Systematic Reviews & Meta-Analyses
- Nelson HD, Vesco KK, Haney E, et al. Nonhormonal therapies for menopausal hot flashes: systematic review and meta-analysis. JAMA. 2006;295(17):2057-2071. doi:10.1001/jama.295.17.2057
- Rada G, Capurro D, Pantoja T, et al. Non-hormonal interventions for hot flushes in women with a history of breast cancer. Cochrane Database Syst Rev. 2010;(9):CD004923. doi:10.1002/14651858.CD004923.pub2
Clinical Trials
- Pandya KJ, Raubertas RF, Flynn PJ, et al. Oral clonidine in postmenopausal patients with breast cancer experiencing tamoxifen-induced hot flushes: a University of Rochester Cancer Center Community Clinical Oncology Program study. Ann Intern Med. 2000;132:788-793.
- Buijs C, de Bock GH, Mourits MJ, et al. Venlafaxine versus clonidine for the treatment of hot flashes in breast cancer patients: a double-blind, randomized cross-over study. Breast Cancer Res Treat. 2009;115(3):573-580. doi:10.1007/s10549-008-0138-7
Pharmacological References
- Patel P, Saadabadi A. Clonidine. StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2026 Jan-. Updated December 13, 2025. PMID: 29083638.
- Nonhormonal Treatment of Vasomotor Symptoms of Menopause. Curr Cardiol Rep. 2025. PMID: 40047411.
- Patel P, Saadabadi A. Clonidine. StatPearls. 2025.
Government/Institutional Sources
- Freedman RR. Menopausal hot flashes: mechanisms, endocrinology, treatment. J Steroid Biochem Mol Biol. 2014;142:115-120.
- DailyMed. Clonidine Extended-Release Tablets (NDA022500). National Library of Medicine. Revised January 2024.
- Claessens AJ, Risler LJ, Eyal S, et al. CYP2D6 mediates 4-hydroxylation of clonidine in vitro. Drug Metab Dispos. 2010;38(9):1393-1396.
- Mehta HR, Patel IK, Patel NH, et al. Implication of enterohepatic re-circulation on single dose bioequivalence evaluation of two brands of clonidine hydrochloride tablets. Indian J Pharm Sci. 2009;71(5):515-520.
- Jin Y, Desta Z, et al. CYP2D6 Genotype, Antidepressant Use, and Tamoxifen Metabolism During Adjuvant Breast Cancer Treatment. J Natl Cancer Inst. 2005;97:30-39.
- Drugs.com. Clonidine Monograph for Professionals (ASHP). Reviewed March 10, 2026.
Related Guides & Cross-Links
Same Category (Non-Hormonal Prescription Medications)
- Fezolinetant (Veozah) — NK3 receptor antagonist, NAMS-recommended
- Elinzanetant (Lynkuet) — Dual NK1/NK3 receptor antagonist
- Paroxetine Low-Dose (Brisdelle) — Only FDA-approved non-hormonal treatment for VMS
- Gabapentin for Menopause — NAMS-recommended antiseizure agent for VMS
- Ospemifene (Osphena) — SERM for GSM symptoms
- Tibolone (Livial) — Synthetic steroid with estrogenic, progestogenic, and androgenic activity
Treatment Overview Guides
- Non-Hormonal Menopause Treatments — Comprehensive overview of all non-hormonal options
- Getting Started with HRT — For women considering whether HRT may be a better option
Condition Guides
- Menopause — Overview of the menopausal transition
- Surgical Menopause — Relevant for abrupt-onset VMS
Complementary Approaches
- Menopause Nutrition & Lifestyle — Lifestyle strategies for symptom management