Melanotan II: Complete Research Guide
On this page
Quick Reference Card
Attribute
Also Known As
- Detail
- MT-II, MT-2, MTII, Melanotan-II, Ac-Nle-c[Asp-His-D-Phe-Arg-Trp-Lys]-NH2
Attribute
Administration
- Detail
- Injectable (subcutaneous); nasal spray (unregulated, variable bioavailability)
Attribute
Research Status
- Detail
- Research Compound. Not FDA-approved for any indication. FDA Category 2 (banned from compounding, 2023). Related compound PT-141 (Bremelanotide) is FDA-approved for HSDD.
Attribute
Typical Dose Range
- Detail
- 250-1000 mcg per day during loading; 500-1000 mcg 1-2x per week for maintenance
Attribute
Half-Life
- Detail
- Approximately 1-2 hours (subcutaneous)
Attribute
Cycle Length
- Detail
- 6-8 weeks loading phase, then maintenance dosing; year-round use not advised
Attribute
Storage
- Detail
- Lyophilized: -20°C or below; Reconstituted: 2-8°C, use within 1-2 weeks
Overview / What Is Melanotan II?
The Basics
Melanotan II is a synthetic peptide designed to mimic a natural hormone your body already produces called alpha-melanocyte-stimulating hormone (alpha-MSH). This natural hormone plays a key role in controlling your skin's pigmentation, essentially telling your skin cells to produce more melanin, the pigment that makes your skin darker when you spend time in the sun.
What makes MT-II different from other tanning approaches is that it works from the inside out. Instead of damaging your skin with UV radiation to force a tan, MT-II signals your melanocytes (the cells that produce pigment) to ramp up melanin production directly. The result is a tan that can develop with minimal sun exposure.
However, MT-II does considerably more than just darken skin. Because it activates multiple receptor types throughout the body, including receptors in the brain, it also affects appetite, sexual arousal, and erectile function. These additional effects were actually discovered by accident during early clinical studies at the University of Arizona in the 1990s, when researchers noticed unexpected sexual arousal responses in their subjects [1]. That discovery eventually led to the development of PT-141 (Bremelanotide), an FDA-approved drug for sexual dysfunction that was derived directly from MT-II research.
It is important to understand that Melanotan II has never been approved by any regulatory agency for any purpose. It is illegal to sell in the United States, United Kingdom, and Australia. The limited clinical data that exists comes from small Phase I studies, and no Phase III trial has ever been conducted [1][2].
The Science
Melanotan II (Ac-Nle-c[Asp-His-D-Phe-Arg-Trp-Lys]-NH2) is a synthetic cyclic heptapeptide analog of alpha-melanocyte-stimulating hormone (alpha-MSH), developed at the University of Arizona by Al-Obeidi, Hadley, and Hruby in 1989 [3]. The compound was created by truncating alpha-MSH to its minimal active core (the His-Phe-Arg-Trp tetrapeptide at positions 6-9) and cyclizing the sequence via a lactam bridge between the side chains of aspartic acid and lysine [3].
Two key structural modifications distinguish MT-II from native alpha-MSH: replacement of methionine at position 4 with norleucine (Nle4, preventing oxidative degradation) and substitution of L-phenylalanine at position 7 with the D-isomer (D-Phe7), which increased receptor binding affinity approximately 1,000-fold and conferred protease resistance [4][5]. The cyclization confers sufficient lipophilicity for blood-brain barrier penetration, a critical pharmacological distinction from the linear Melanotan I analog (afamelanotide), which remains peripherally confined [6].
MT-II functions as a non-selective melanocortin receptor agonist, activating MC1R, MC3R, MC4R, and MC5R with sub-nanomolar to low-nanomolar affinity, while sparing MC2R (the ACTH-specific adrenal receptor), meaning it does not trigger cortisol synthesis [3][7]. This non-selectivity is the source of both its broad effects and its clinical limitations.
Molecular Identity
Attribute
Amino Acid Sequence
- Detail
- Ac-Nle-c[Asp-His-D-Phe-Arg-Trp-Lys]-NH2
Attribute
Molecular Formula
- Detail
- C50H69N15O9
Attribute
Molecular Weight
- Detail
- 1024.18 g/mol
Attribute
CAS Number
- Detail
- 121062-08-6
Attribute
PubChem CID
- Detail
- 92432
Attribute
Structure Type
- Detail
- Cyclic heptapeptide with lactam bridge, N-terminal acetylation, C-terminal amidation
Attribute
Key Modification
- Detail
- Lactam bridge between Asp gamma-carboxyl and Lys epsilon-amino groups
Attribute
D-Amino Acid
- Detail
- D-Phe at position 4 of cyclic core
Attribute
Origin
- Detail
- Synthetic; truncated cyclic analog of alpha-MSH
Mechanism of Action
The Basics
Your skin contains specialized cells called melanocytes that produce melanin, the pigment that gives skin its color. When you sit in the sun, your body sends a signal (via alpha-MSH) telling these cells to make more melanin as a form of protection against UV damage. MT-II essentially amplifies this same signal, but much more powerfully and without needing as much (or any) UV exposure as a trigger.
Think of melanocortin receptors as different locks on different doors throughout your body. Your natural alpha-MSH hormone is like a key that fits one lock particularly well (the pigmentation lock on your skin cells, called MC1R). MT-II is more like a master key that fits several locks at once. Beyond the skin pigmentation lock, it also opens the appetite lock (MC4R in the brain, reducing hunger), the sexual arousal lock (MC3R and MC4R, increasing libido and erectile response), and a few others with less understood effects.
This master-key quality is why MT-II produces its constellation of effects: tanning, appetite reduction, and sexual arousal all happen simultaneously because the peptide is activating multiple receptor systems at once. It is also why MT-II has proven difficult to develop as a targeted medication. You cannot unlock just the tanning door without also opening the others.
The Science
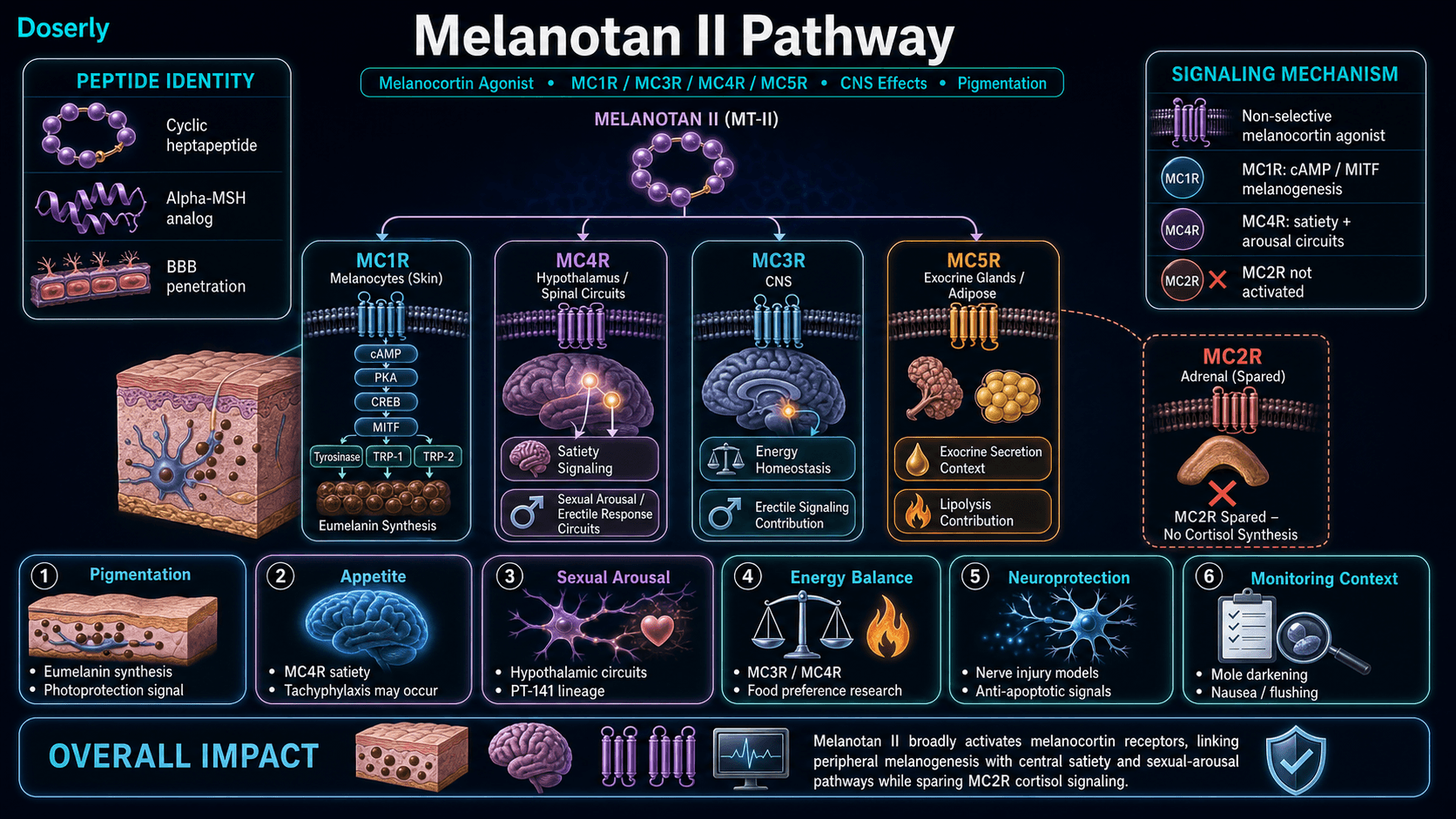
MT-II exerts its effects through agonism at four of the five melanocortin receptor subtypes:
MC1R (Melanogenesis and Photoprotection): Binding to MC1R on melanocytes activates adenylate cyclase, increasing intracellular cAMP, which activates PKA and the CREB transcription factor. This upregulates MITF (microphthalmia-associated transcription factor), the master regulator of melanocyte gene expression, driving production of tyrosinase, TRP-1, and TRP-2, the enzymes responsible for eumelanin synthesis [4][5]. MC1R activation also enhances nucleotide excision repair of UV-induced DNA damage independently of pigmentation [5]. Loss-of-function MC1R variants (R151C, R160W, D294H), prevalent in fair-skinned populations, are established melanoma risk factors precisely because they impair both eumelanin production and DNA repair capacity [5].
MC3R and MC4R (Central Nervous System Effects): MC4R activation in the hypothalamus mediates appetite suppression through the melanocortin satiety pathway and pro-erectile signaling through hypothalamic and spinal cord circuits [8][9]. MC3R modulates energy homeostasis and contributes to erectile signaling [8]. These central effects are pharmacologically significant for MT-II because the cyclic structure crosses the blood-brain barrier; the linear Melanotan I analog does not achieve meaningful CNS penetration [6].
MC5R (Exocrine Effects): MC5R, expressed in exocrine glands including sebaceous and sweat glands, modulates secretion and may contribute to lipolysis. Clinical significance remains uncertain [7].
MC2R (Spared): MT-II does not activate MC2R (Ki > 1 microM), the ACTH-specific receptor responsible for adrenal steroidogenesis. Neither melanocortin analog triggers cortisol release, an important safety boundary [3][7].
Pathway Visualization
Pharmacokinetics
The Basics
MT-II moves through your body relatively quickly. After a subcutaneous injection, it reaches its peak concentration in about 1-2 hours and is largely cleared within a few hours after that. This short active window is one reason why daily dosing is typically discussed during loading phases.
However, the effects of MT-II outlast its presence in the bloodstream. The tanning effect, for example, builds progressively over days and weeks because melanin production is a cumulative process. Once melanocytes have been stimulated to produce melanin, that pigment remains in the skin even after the peptide itself has been cleared. This is why maintenance dosing can be reduced to once or twice per week after the initial loading period.
The nasal spray route, which has been popularized on social media, delivers substantially less peptide to the bloodstream compared to injection, with much more variable absorption. No clinical study has ever quantified the bioavailability of nasally administered MT-II [2].
The Science
MT-II exhibits rapid absorption following subcutaneous injection with an absorption half-life of 0.07-0.79 hours and peak plasma concentration (Tmax) reached within approximately 1-2 hours [1]. The elimination half-life is 0.8-1.7 hours, consistent with peptidase-mediated degradation [1][6].
Parameter
Route
- Value
- Subcutaneous injection
Parameter
Tmax
- Value
- ~1-2 hours
Parameter
Elimination half-life
- Value
- 0.8-1.7 hours
Parameter
BBB penetration
- Value
- Yes (cyclic structure confers lipophilicity)
Parameter
SC bioavailability
- Value
- Assumed high (not formally quantified)
Parameter
Oral bioavailability
- Value
- Negligible
Parameter
Nasal bioavailability
- Value
- Low, variable, unquantified
Despite the short pharmacokinetic half-life, the pharmacodynamic effects on melanogenesis persist for days to weeks because melanin turnover in the epidermis operates on a separate timescale from peptide elimination. Eumelanin deposited in keratinocytes through melanosome transfer persists until those cells are naturally shed through epidermal turnover, typically over 28-30 days [5][6].
Research & Clinical Evidence
Skin Pigmentation
The Basics
The tanning effect is the most extensively studied application of MT-II, though "extensively" is relative. In the original human study, researchers found that just five low doses given over two weeks produced measurable tanning in light-skinned volunteers [1]. The effect works by stimulating your melanocytes to produce eumelanin (the brown-black pigment that provides genuine photoprotection), rather than pheomelanin (the reddish pigment associated with sun damage in fair-skinned individuals).
Community reports consistently describe noticeable pigmentation changes within the first 1-2 weeks of use, with many users achieving tans they describe as deeper and more even than anything achievable through sun exposure alone.
The Science
Dorr and colleagues conducted the only formal Phase I clinical study of MT-II in 1996: a single-blind, alternating-day, placebo-controlled trial in three male volunteers receiving subcutaneous injections at 0.01-0.025 mg/kg (approximately 0.7-1.75 mg for a 70 kg person) [1]. Dose-dependent increases in skin melanin density were observed, with measurable tanning after just five administrations over two weeks. The minimal erythema dose (MED) also increased, suggesting functional photoprotection [1].
It is worth noting that current community dosing protocols (250-500 mcg) are 2-3x lower than the Dorr trial's effective doses (0.7-1.75 mg), reflecting a deliberate trade-off favoring reduced nausea over faster tanning onset [2].
Sexual Function and Erectile Response
The Basics
The sexual arousal effects of MT-II were discovered accidentally during the original tanning studies. Researchers found that the peptide triggered spontaneous erections and heightened sexual desire in male subjects, leading to a whole new line of research. This eventually produced bremelanotide (PT-141, marketed as Vyleesi), which received FDA approval in 2019 for hypoactive sexual desire disorder in premenopausal women [10].
Importantly, MT-II appears to work through a different pathway than medications like sildenafil (Viagra). While Viagra improves blood flow, MT-II acts on receptors in the brain that control sexual desire and arousal. This distinction means that in studies, MT-II was effective for men with psychogenic (stress or anxiety-related) erectile dysfunction even when Viagra had failed [11][12].
The Science
Wessells and colleagues conducted small crossover studies (n=10-20) demonstrating that 8 of 10 men with psychogenic erectile dysfunction developed clinically apparent erections after MT-II administration, with mean tip rigidity exceeding 80% for 38 minutes versus 3 minutes on placebo (P=0.0045) [11]. Increased sexual desire was reported after 68% of MT-II doses versus 19% of placebo doses [12]. A subsequent study in men with organic (vascular) erectile dysfunction showed reduced efficacy, suggesting the MC4R-mediated mechanism is most effective in the absence of vascular pathology [13].
In women, a proof-of-concept study (Diamond et al., 2006) demonstrated increased genital arousal response and enhanced subjective sexual desire following MT-II administration, providing the mechanistic basis for bremelanotide development [14].
Appetite Suppression and Metabolic Effects
The Basics
Many people who use MT-II report reduced appetite as a secondary effect. Research in animal models suggests this occurs because MT-II activates the same brain receptors (MC4R) involved in satiety signaling. Some community users note this as a welcome bonus, particularly those using MT-II alongside fitness or body composition goals.
However, this appetite-reducing effect appears to diminish with continued use. The body adapts to the signal over time, which limits MT-II's potential as a sustained weight management tool.
The Science
MT-II reduces food intake through central MC3R/MC4R activation, operating through both leptin-dependent and leptin-independent satiety pathways in the paraventricular nucleus of the hypothalamus [15][16]. Unlike leptin, MT-II crosses the blood-brain barrier in concentrations sufficient to influence hypothalamic TRH expression, giving it a theoretical pharmacokinetic advantage as an exogenous anorectic agent [16].
Animal studies demonstrate that MT-II significantly reduces food consumption and alters macronutrient preference, with treated mice preferentially avoiding fatty foods through MC4R-dependent mechanisms [15]. However, tachyphylaxis (diminishing response with repeated dosing) of the anorectic effect occurs with chronic administration, limiting sustained utility for weight management [17].
Neuroprotection and Nerve Regeneration
The Basics
Emerging animal research suggests MT-II may have neuroprotective properties, meaning it could help protect nerve cells from damage and potentially support nerve regeneration. In rat studies, MT-II appeared to help damaged nerves recover faster and offered some protection against the nerve damage caused by chemotherapy drugs [18]. This research is very early-stage and has not been tested in humans.
The Science
In a rat model of sciatic nerve crush injury, MT-II administration at 20 mcg/kg promoted functional recovery and nerve regeneration [18]. Additionally, MT-II partially blocked cisplatin-induced neurotoxicity, suggesting a protective mechanism against chemotherapy-related peripheral neuropathy [18]. Melanocortin receptor activation has also been investigated in models of ischemic stroke, traumatic brain injury, and Alzheimer's disease, with demonstrated anti-inflammatory and anti-apoptotic effects [19][20].
Alcohol and Impulse Control
The Basics
An interesting line of animal research has found that MT-II may reduce alcohol consumption. In rats that preferred alcohol, MT-II reduced their intake and increased water consumption instead. When combined with naltrexone (a medication already used to treat alcohol dependence), the effect was dramatically amplified, with efficacy boosted more than seven-fold [21]. This research is entirely preclinical and no human studies have been conducted.
The Science
York and colleagues demonstrated that MT-II reduces ethanol intake through melanocortin activity in the amygdala [22]. Navarro and colleagues showed that MT-II works synergistically with naltrexone to blunt binge-like ethanol intake in mice (C57BL/6J), with the combined treatment achieving greater-than-additive effects [21]. The mechanism likely involves MT-II's stimulation of oxytocin release and modulation of reward circuitry through MC4R activation [23].
Biomarker Evidence Matrix
Category
Skin Health
- Evidence Strength
- 7/10
- Reported Effectiveness
- 8/10
- Summary
- Strong Phase I human data showing dose-dependent melanogenesis. Overwhelmingly positive community reports of rapid, deep tanning.
Category
Libido
- Evidence Strength
- 6/10
- Reported Effectiveness
- 7/10
- Summary
- Small but well-designed crossover human studies demonstrating MC4R-mediated sexual desire. Consistent and prominent community reporting.
Category
Sexual Function
- Evidence Strength
- 6/10
- Reported Effectiveness
- 7/10
- Summary
- Human crossover studies (n=10-20) with significant erectile response in psychogenic ED (P=0.0045). Community reports spontaneous erections.
Category
Appetite & Satiety
- Evidence Strength
- 5/10
- Reported Effectiveness
- 6/10
- Summary
- Animal studies demonstrate MC4R-mediated appetite reduction. Community reports confirm but note tachyphylaxis with chronic use.
Category
Nausea & GI Tolerance
- Evidence Strength
- 6/10
- Reported Effectiveness
- 3/10
- Summary
- Dose-dependent nausea established in Phase I studies (13% severe at erectile doses). Near-universal negative community reporting of initial nausea.
Category
Side Effect Burden
- Evidence Strength
- 5/10
- Reported Effectiveness
- 4/10
- Summary
- Known side effect profile from Phase I data and case reports. Community mixed on tolerability; many power through, some discontinue.
Category
Temperature Regulation
- Evidence Strength
- 4/10
- Reported Effectiveness
- 3/10
- Summary
- Facial flushing documented in Phase I studies. Community consistently reports flush as unpleasant but transient.
Category
Fat Loss
- Evidence Strength
- 3/10
- Reported Effectiveness
- 5/10
- Summary
- Animal data supports MC4R-mediated effects on energy balance. Limited and heavily confounded community reporting.
Category
Weight Management
- Evidence Strength
- 3/10
- Reported Effectiveness
- 5/10
- Summary
- Linked to appetite suppression mechanism. Community reporting is indirect and confounded.
Category
Mood & Wellbeing
- Evidence Strength
- 2/10
- Reported Effectiveness
- 6/10
- Summary
- No direct evidence for mood effects; community positivity likely driven by appearance satisfaction (psychosocial, not pharmacological).
Category
Body Image
- Evidence Strength
- 2/10
- Reported Effectiveness
- 7/10
- Summary
- No clinical evidence. Strong community signal driven by satisfaction with cosmetic tanning outcomes.
Category
Cravings & Impulse Control
- Evidence Strength
- 4/10
- Reported Effectiveness
- 5/10
- Summary
- Preclinical evidence for alcohol craving reduction via MC4R/oxytocin. No community discussion of this application.
Category
Longevity & Neuroprotection
- Evidence Strength
- 3/10
- Reported Effectiveness
- N/A
- Summary
- Preclinical neuroprotection data (nerve regeneration, Alzheimer's model). No community data.
Category
Energy Levels
- Evidence Strength
- 2/10
- Reported Effectiveness
- 4/10
- Summary
- Mild fatigue reported as side effect. No evidence of energy enhancement. Community mixed.
Benefits & Potential Effects
The Basics
The primary reason people are interested in MT-II is for tanning. The peptide produces a noticeable, even tan that can develop with much less sun exposure than would normally be required. For fair-skinned individuals, this can mean achieving a level of pigmentation that natural tanning could never provide. Many users report that the tan looks more natural than spray tans or self-tanners.
Beyond tanning, the most commonly discussed secondary effects are increased libido and appetite suppression. The libido effect is particularly well-documented and was significant enough to spawn an entirely separate FDA-approved drug (bremelanotide/PT-141). The appetite suppression effect is real but tends to fade over time as the body adapts.
It is essential to weigh these effects against the significant side effect profile and regulatory status of MT-II. This is not an approved medication, and the risk-benefit calculation is a personal decision that should be made with full awareness of the limitations of current safety data.
The Science
The documented and reported effects of MT-II can be categorized by their mechanistic basis:
MC1R-mediated effects (peripheral): Increased eumelanin synthesis and melanocyte dendricity, producing progressive skin darkening and enhanced photoprotection. Increased minimal erythema dose (MED) indicating functional UV protection [1][5].
MC4R-mediated effects (central): Appetite suppression through hypothalamic satiety pathway activation [15][16]. Pro-erectile and pro-arousal effects through hypothalamic and spinal cord MC4R circuits [8][9]. The erectile response represents one of the most dramatic effect sizes reported in the sexual medicine literature, with tip rigidity sustained above 80% for 38 minutes in psychogenic ED patients [11].
MC3R-mediated effects (central): Contribution to energy homeostasis modulation and erectile signaling, though less well-characterized than MC4R-mediated effects [8].
MC5R-mediated effects (peripheral): Potential modulation of sebaceous secretion and lipolysis, though clinical significance remains uncertain [7].
Side Effects & Safety Considerations
The Basics
MT-II is not considered a side-effect-free peptide. Most users experience at least some adverse effects, particularly during the initial dosing period.
Nausea is the most commonly reported side effect and is directly dose-dependent. Starting at lower doses and titrating up gradually is the most widely recommended mitigation strategy. Many users find that nausea diminishes significantly after the first week. Evening dosing and having a light snack beforehand are commonly cited community strategies.
Facial flushing (warmth, redness, and a "wave" of heat) is nearly universal in the first few injections and typically peaks 30-90 minutes post-injection. It is uncomfortable but transient and generally diminishes with continued use.
Mole and freckle darkening is a significant safety concern. MT-II stimulates melanocytes throughout the body, including those in existing moles and freckles. Users widely report darkening of existing pigmented lesions and, in some cases, the appearance of new ones. Anyone with a personal or family history of melanoma or atypical mole syndrome should not use MT-II. Regular dermatological monitoring with ABCDE screening (Asymmetry, Border, Color, Diameter, Evolution) is strongly recommended for anyone considering this compound.
Spontaneous erections and increased libido are commonly reported, particularly in males. While some users view this as a benefit, others find it inconvenient. This effect is dose-dependent and more pronounced at higher doses.
Other reported effects include mild fatigue, reduced appetite, yawning/stretching episodes, darkening of the lips or gums, headache, and elevated blood pressure.
The Science
Common adverse effects documented in clinical studies and community reporting include: nausea (dose-dependent; 13% severe at preferred erectile dose) [1], facial flushing (vasodilatory, transient) [1], fatigue and yawning, spontaneous erections (MC4R-mediated) [11], appetite suppression [15], and injection site reactions [1].
Dermatologic signals: Darkening of existing nevi, eruption of new nevi (including those with dysplastic histology), and melanonychia have been documented across multiple independent case series [24][25][26]. These changes are consistent with non-selective melanocyte stimulation and represent the most clinically relevant monitoring concern.
Melanoma risk: The weight of evidence indicates that MC1R activation is photoprotective rather than oncogenic. The Addison's disease cohort (3,299 patients with chronic MC1R activation over 40 years) shows a standardized incidence ratio for melanoma of 0.7 [5]. All five melanoma cases reported in MT-II users involved confounding UV exposure or pre-existing risk factors [5][24][25][26]. However, no formal animal carcinogenicity studies have been conducted for either melanotan analog [5][6].
Serious adverse events from case reports:
- Rhabdomyolysis: A 39-year-old male injected 6 mg (far exceeding typical protocols) and presented with creatine phosphokinase peaking at 17,773 IU/L, requiring three days of intensive care [27].
- Renal infarction: A 45-year-old with approximately 27 mg cumulative exposure over 6 months developed right-sided renal infarction affecting approximately 50% of the kidney [28].
- Priapism: Reported with overdose, consistent with MC4R-mediated erectile mechanism [1].
Contraindications: Personal or family history of melanoma or dysplastic nevus syndrome, uncontrolled hypertension or cardiovascular disease, pregnancy/lactation (no safety data), concurrent priapism risk factors [6].
The side effects and contraindications above give you a map of what to watch for. Doserly turns that map into a daily practice. Log the specific biomarkers and symptoms associated with this compound's known risk profile, and the app builds a timeline of how your body is responding across your cycle.
Trending in the wrong direction on a key marker? Noticing a pattern that started two weeks into your protocol? Doserly connects the dots between your protocol timeline and your logged data, making it easier to spot emerging issues early and have informed, data-backed conversations with your healthcare provider about what's working and what needs attention.
Capture changes while they are still fresh.
Log symptoms, energy, sleep, mood, and other observations alongside protocol events so patterns do not live only in memory.
Trend view
Symptom timeline

Symptom tracking is informational and should be interpreted with a qualified clinician.
Dosing Protocols
The Basics
MT-II dosing follows a two-phase approach that most sources agree on: a loading phase to build up melanin production, followed by a maintenance phase to sustain results with less frequent dosing.
During the loading phase, sources suggest starting at a low dose (typically 100-250 mcg per day) and gradually increasing over several weeks. This slow titration approach is widely recommended because it significantly reduces nausea, the most common barrier to continued use. Most sources indicate that daily dosing continues for 6-8 weeks.
After achieving the desired level of pigmentation, most protocols transition to maintenance dosing at 1-2 injections per week. The maintenance dose is typically in the same range as the loading dose but administered less frequently.
Skin type plays a role in protocol duration. Fair-skinned individuals (Fitzpatrick types I-II) generally require longer loading phases and may need higher cumulative doses to achieve noticeable results compared to those with naturally darker skin.
The Science
The only human pharmacokinetic dosing data derives from Dorr et al. (1996), which used 0.01-0.025 mg/kg subcutaneously (approximately 0.7-1.75 mg for a 70 kg individual) [1]. Current community protocols use 2-3x lower doses than the Dorr trial's effective range, reflecting empirical nausea-minimization strategies rather than formal dose-optimization studies [2].
Commonly reported loading protocol:
Phase
Tolerance test
- Dose
- 250 mcg
- Frequency
- Single dose
- Duration
- Day 1
Phase
Loading (week 1)
- Dose
- 250 mcg
- Frequency
- Daily
- Duration
- 7 days
Phase
Loading (week 2)
- Dose
- 500 mcg
- Frequency
- Daily
- Duration
- 7 days
Phase
Loading (week 3)
- Dose
- 750 mcg
- Frequency
- Daily
- Duration
- 7 days
Phase
Loading (weeks 4-8)
- Dose
- 1000 mcg
- Frequency
- Daily
- Duration
- 4-5 weeks
Phase
Maintenance
- Dose
- 500-1000 mcg
- Frequency
- 1-2x weekly
- Duration
- Ongoing
Reconstitution: 3.0 mL bacteriostatic water per 10 mg vial yields a concentration of 3.33 mg/mL. At this concentration, 1 unit on a U-100 insulin syringe equals approximately 33.3 mcg [2].
Timing notes: Evening dosing is commonly recommended in community protocols to allow nausea to resolve during sleep. For sexual function effects, administration 4-6 hours before anticipated activity has been reported [2].
Consistency is the difference between a protocol that delivers results and one that wastes time and money. Doserly was built for exactly this: keeping you on track with the precision your protocol demands.
The built-in calculators handle the math you shouldn't be doing in your head. The reconstitution calculator tells you exactly how much bacteriostatic water to add for your target concentration. The dose calculator converts between units, milligrams, and syringe markings so you draw the right amount every time. The injection site heat map tracks where you've administered and when, helping you rotate sites systematically to reduce tissue damage, scarring, and absorption inconsistencies from overusing the same area. Pair that with smart reminders tuned to your protocol's timing requirements, and you build the kind of daily consistency that separates optimized protocols from haphazard ones.
Turn symptom and safety notes into a clearer timeline.
Doserly helps you log doses, symptoms, and safety observations side by side so patterns are easier to discuss with a qualified clinician.
Pattern view
Logs and observations

Pattern visibility is informational and should be reviewed with a clinician.
What to Expect
Week 1 (Days 1-7): Most users start at a low dose (100-250 mcg). Side effects are most pronounced during this period. Expect nausea, facial flushing, and possibly a slight "wave" of warmth 30-90 minutes after injection. Some people report yawning and mild fatigue. Pigmentation changes are generally not yet visible, though some may notice a very subtle undertone shift by the end of the first week. Libido changes may begin to emerge.
Week 2 (Days 8-14): As the dose titrates upward and the body adjusts, nausea typically diminishes significantly. Flushing may persist but becomes less intense. Many users begin to notice the first visible signs of pigmentation, particularly on areas exposed to even incidental sunlight. Forearms, face, and neck often show changes first. Libido and erectile effects, if present, become more noticeable.
Weeks 3-4: The tan becomes clearly visible to others. Pigmentation deepens noticeably, especially with even modest UV exposure. Appetite suppression effects typically peak during this period. Side effects continue to diminish for most users. Mole and freckle darkening may become apparent and should be monitored.
Weeks 5-8: Full loading phase. Users at the higher end of the dosing range report achieving a deep, even tan that others describe as looking like a week-long beach vacation. This is typically when the transition to maintenance dosing occurs. Some users achieve their desired result earlier and begin reducing frequency sooner.
Maintenance (Week 8+): With 1-2 injections per week, most users report sustaining their tan with minimal additional UV exposure. The appetite-suppressive effect may diminish (tachyphylaxis). Libido effects generally persist with continued dosing. The tan fades gradually over weeks to months if dosing is discontinued, as pigmented keratinocytes are shed through normal skin turnover.
The week-by-week expectations above are drawn from research and community reports, but your experience will be uniquely yours. Doserly's biomarker tracking transforms those general timelines into personal data points you can actually see and measure.
Log the specific markers relevant to this compound, whether that's pain levels, energy, sleep quality, body composition, recovery time, or mood, and watch your own trend lines emerge over weeks and months. Did your key markers start shifting in week three, like the research suggests? Is your experience tracking with what the community reports, or diverging? Over time, this creates something more valuable than any guide: an evidence-based picture of how your body responds to this specific compound, at your specific dose, within your specific health context.
Build reminders around the routine, not just the compound.
Doserly can keep timing, skipped doses, and schedule changes organized so the plan you read about becomes easier to follow and review.
Today view
Upcoming reminders
Reminder tracking supports consistency; it does not select a protocol for you.
Interaction Compatibility
Commonly Combined With
- PT-141 (Bremelanotide) — Related melanocortin agonist. Some users combine MT-II (for tanning) with on-demand PT-141 (for sexual function). Both act on melanocortin receptors; concurrent use increases the risk of receptor overstimulation, nausea, and cardiovascular effects.
- GHK-Cu — Copper peptide for skin rejuvenation. Community sources list this as a complementary skin combination.
- BPC-157 — Listed in community protocols as a skin-complementary compound.
- KPV — Anti-inflammatory peptide. Listed as a skin-stack companion in community protocols.
- Glutathione — Antioxidant. Community sources suggest pairing for overall skin health support.
- Retatrutide, Cagrilintide — GLP-1/GIP agonists. Listed in community fat loss stacking protocols alongside MT-II.
- MOTS-C, SS-31, 5-Amino-1MQ — Metabolic peptides listed as complementary in fat loss stacking contexts.
- Tesofensine — Appetite suppressant. Listed in community protocols for further appetite reduction alongside MT-II.
Cautions and Contraindications
- Other melanocortin agonists: Concurrent use of MT-II with PT-141 or other MCR agonists requires careful monitoring due to overlapping receptor targets.
- Antihypertensive medications: MT-II may transiently increase blood pressure. Individuals on blood pressure medications should exercise caution and monitor closely.
- Phosphodiesterase inhibitors (sildenafil, tadalafil): Combining with MT-II may increase priapism risk given MT-II's pro-erectile MC4R effects.
- UV exposure: While not a drug interaction, excessive UV exposure combined with MT-II use represents the most significant practical risk, as it compounds potential skin damage risks beyond what MT-II alone may present.
Administration Guide
MT-II is most commonly administered via subcutaneous injection. The peptide is supplied as a lyophilized (freeze-dried) powder that requires reconstitution before use.
Materials typically used: U-100 insulin syringes (29-31 gauge, 1/2 inch needle), bacteriostatic water for reconstitution, alcohol swabs for vial and injection site preparation, and a sharps container for needle disposal. For doses under 10 units, 30-unit or 50-unit insulin syringes provide improved measurement accuracy.
Reconstitution: The most commonly cited reconstitution method uses 3.0 mL of bacteriostatic water per 10 mg vial, yielding a concentration of 3.33 mg/mL. Water should be injected slowly along the inside wall of the vial to avoid foaming. The vial is then gently rolled or swirled (never shaken vigorously) until fully dissolved.
Timing considerations: Evening administration is widely recommended in community protocols because nausea, the most common side effect, peaks 30-90 minutes post-injection and can be slept through. For those seeking the sexual function effects, administration 4-6 hours before anticipated activity has been reported. Some community protocols suggest splitting the daily dose between morning and evening for more consistent appetite suppression.
Post-administration observations: Expect facial flushing and warmth within 30-90 minutes. Nausea, if it occurs, typically peaks within the same window and resolves within 1-2 hours. If persistent nausea occurs, a light snack before injection and ginger tea have been widely cited as mitigation strategies. Any injection site redness or stinging should be mild and resolve within hours.
Supplies & Planning
The following materials are generally associated with MT-II protocols:
- Peptide vials: MT-II is commonly available in 10 mg lyophilized vials
- Bacteriostatic water: Used for reconstitution (3.0 mL per 10 mg vial is the most frequently cited ratio)
- Insulin syringes: U-100 (1 mL, 29-31 gauge) for injection. Consider 30 or 50-unit syringes for small-volume doses
- Alcohol swabs: For cleaning vial stoppers and injection sites before each use
- Sharps container: For safe disposal of used syringes and needles
The total supplies needed will depend on the specific protocol, dose, and duration determined in consultation with a healthcare provider. Use a reconstitution calculator for precise preparation math.
Storage & Handling
Lyophilized (powder) form:
- Optimal long-term storage: -20°C (-4°F) or below, protected from light and moisture
- Short-term storage: Refrigeration at 2-8°C (35.6-46.4°F) is acceptable for weeks to months
- Room temperature: Acceptable for short periods (days) if dry and protected from light, but not recommended for extended storage
- Keep in sealed packaging with desiccant to minimize moisture exposure
- Allow vials to reach room temperature before opening to prevent condensation
Reconstituted (liquid) form:
- Refrigerate immediately at 2-8°C (35.6-46.4°F)
- Use within 1-2 weeks when reconstituted with bacteriostatic water
- Do NOT freeze reconstituted solution; freezing denatures peptides
- Avoid freeze-thaw cycles; if longer storage is needed, aliquot into sterile single-use vials before freezing
- Inspect for clarity before each use; discard if cloudy, discolored, or if particles are visible
- Label vials with the reconstitution date
Lifestyle Factors
UV exposure and sun protection: This is the most critical lifestyle consideration for MT-II users. While MT-II stimulates melanin production that provides some UV protection, it does not eliminate the need for sun protection. UV radiation causes DNA damage independently of whether you have a tan. Responsible sun practices (appropriate sunscreen, limiting exposure duration, avoiding tanning beds) remain essential. Many community sources emphasize this point explicitly. The photoprotection from MT-II-stimulated eumelanin is a bonus, not a replacement for sun safety.
Hydration: Adequate fluid intake is particularly important given the common nausea and appetite suppression effects. Dehydration can worsen nausea and impair overall wellbeing.
Dermatological monitoring: Regular self-examination of moles and skin using the ABCDE criteria (Asymmetry, Border irregularity, Color variation, Diameter > 6mm, Evolution over time) is strongly recommended. Baseline and follow-up full-body dermatological exams every 3-6 months are advised during and after use. Discontinue immediately if new pigmented lesions arise or existing lesions change rapidly.
Bloodwork and monitoring: Community protocols suggest tracking CMP/liver function (ALT, AST, ALP, bilirubin, creatinine/eGFR), CBC, blood pressure, and heart rate. For those using MT-II for appetite effects, fasting glucose and HbA1c monitoring has been recommended. Vitamin D supplementation may be advisable for users limiting sun exposure.
Sleep: Ensuring 7-9 hours of quality sleep supports hormonal balance and overall recovery. Evening dosing aligns with natural sleep timing and allows side effects to resolve overnight.
Regulatory Status & Research Classification
United States (FDA): Not approved for any indication. The FDA classified MT-II as Category 2 in 2023, effectively banning it from compounding pharmacy preparation [2][6]. It is not a DEA-scheduled controlled substance, so possession is not criminalized, but sale and distribution as a therapeutic product is prohibited. MT-II is expected to remain restricted even following the February 2026 HHS partial reversal of Category 2 peptide bans [6]. The related compound bremelanotide (PT-141/Vyleesi) received FDA approval in 2019 for hypoactive sexual desire disorder in premenopausal women [10].
United Kingdom (MHRA): Illegal to sell as a medicinal product. Nasal tanning sprays containing MT-II fall outside both medicinal products and cosmetics regulation, creating an enforcement gap that regulators are actively working to close [6]. The UK Chartered Trading Standards Institute has issued warnings about youth targeting through flavored nasal tanning products [6].
Australia (TGA): Illegal to sell. The TGA requested removal of 4,800+ unlawful therapeutic goods advertisements from digital platforms in 2023-2024, many related to melanotan products [6].
European Union (EMA): Not approved. Note that Melanotan I (afamelanotide, marketed as Scenesse) IS EMA/FDA-approved for erythropoietic protoporphyria, but this is a different compound with a different selectivity profile.
WADA status: Melanotan II is listed on the WADA Prohibited List under S2 (Peptide Hormones, Growth Factors, Related Substances, and Mimetics).
Active clinical trials: No active clinical trials for MT-II are registered as of 2026. The only formal human trial was the Dorr et al. Phase I study (1996) [1]. Clinical development efforts shifted to bremelanotide (PT-141) for sexual dysfunction indications.
Product quality concern: Analysis of commercially available MT-II products has revealed significant quality issues. When Imperial College London researchers analyzed 10 tanning kits, some contained more than 100 unidentified ingredients. LegitScript data indicates 41% of tested products showed laboratory-confirmed contamination or mislabeling [6].
Regulatory status changes frequently. Always verify the current legal status of any compound in your specific country or jurisdiction before making any decisions.
FAQ
What is Melanotan II used for?
MT-II is a research peptide that has been studied primarily for its ability to stimulate skin pigmentation (tanning) through melanocortin receptor activation. It has also been investigated for effects on sexual function and appetite. It is not approved for any therapeutic use by any regulatory agency worldwide.
What is the difference between Melanotan I and Melanotan II?
Melanotan I (afamelanotide) is a linear 13-amino-acid peptide that selectively activates MC1R (the skin pigmentation receptor) and does not cross the blood-brain barrier. It is FDA/EMA-approved as Scenesse for erythropoietic protoporphyria. Melanotan II is a cyclic 7-amino-acid peptide that non-selectively activates four melanocortin receptors, including brain receptors that produce appetite suppression and sexual arousal. MT-II has never completed clinical development and remains unapproved.
Does Melanotan II cause melanoma?
The available evidence indicates that MC1R activation is photoprotective rather than oncogenic. A 40-year follow-up of 3,299 Addison's disease patients (who have chronic MC1R activation) found melanoma incidence numerically below expected rates [5]. All five melanoma cases reported in MT-II users involved confounding factors such as concurrent tanning bed use or familial melanoma risk [5][24][25]. However, MT-II does stimulate melanocyte activity and can darken moles, and no long-term safety studies have been conducted.
Is Melanotan II legal?
MT-II is illegal to sell in the United States, United Kingdom, and Australia. The FDA classified it as Category 2 in 2023. It is not a DEA-scheduled controlled substance, meaning possession is not criminalized, but commercial sale and distribution is prohibited [6].
What are the most common side effects?
Based on available research and community reports, nausea (dose-dependent) is the most common adverse effect, followed by facial flushing, appetite reduction, and increased libido/spontaneous erections. Darkening of existing moles and freckles is widely reported. Serious adverse events including rhabdomyolysis and renal infarction have been documented at supratherapeutic doses [1][27][28].
How long does it take to see results?
Community reports describe noticeable pigmentation changes within the first 1-2 weeks of daily dosing, with significant visible tanning typically achieved by weeks 3-4. Results vary significantly based on skin type, dose, and UV exposure.
Are nasal tanning sprays effective?
No published clinical trial has evaluated the intranasal route for MT-II. Nasal bioavailability is substantially lower and more variable than subcutaneous injection. Nasal tanning sprays are unregulated products of unknown composition and dose [2][6].
What about PT-141? How is it different?
PT-141 (Bremelanotide) is a direct derivative of MT-II research. It was developed specifically to isolate the sexual arousal mechanism (MC4R agonism) and is FDA-approved for hypoactive sexual desire disorder in premenopausal women [10]. PT-141 produces minimal tanning compared to MT-II.
Sources & References
Clinical Trials and Human Studies
[1] Dorr RT, Lines R, Levine N, et al. Evaluation of melanotan-II, a superpotent cyclic melanotropic peptide in a pilot phase-I clinical study. Life Sci. 1996;58(20):1777-1784. PMID: 8637402
[2] Dorr RT, Ertl G, et al. Melanotan II: an investigational peptide for tanning and photoprotection. J Am Acad Dermatol. 2000. PMID: 10822066
[10] FDA. Bremelanotide (Vyleesi) Prescribing Information. Approved June 2019.
[11] Wessells H, Fuciarelli K, Hansen J, et al. Synthetic melanotropic peptide initiates erections in men with psychogenic erectile dysfunction: double-blind, placebo-controlled crossover study. J Urol. 1998;160(2):389-393. PMID: 9679884
[12] Wessells H, Levine N, Hadley ME, et al. Melanocortin receptor agonists, penile erection, and sexual motivation. Int J Impot Res. 2000;12(Suppl 4):S74-S79. PMID: 11035391
[13] Wessells H, et al. Effect of an alpha-MSH analog on penile erection and sexual desire in men with organic erectile dysfunction. Urology. 2000;56(4):641-646. PMID: 11018622
[14] Diamond LE, Earle DC, Heiman JR, et al. An effect on the subjective sexual response in premenopausal women with sexual arousal disorder by bremelanotide (PT-141), a melanocortin receptor agonist. J Sex Med. 2006;3(4):628-638. DOI: 10.1111/j.1743-6109.2006.00215.x
Foundational Pharmacology
[3] Al-Obeidi F, Castrucci AM, Hadley ME, Hruby VJ. Potent and prolonged acting cyclic lactam analogues of alpha-melanotropin: design based on molecular dynamics. J Med Chem. 1989;32(12):2555-2561. PMID: 2555512
[4] Sawyer TK, Sanfilippo PJ, Hruby VJ, et al. [Nle4, D-Phe7]-alpha-MSH: a highly potent alpha-melanotropin with ultralong biological activity. PNAS. 1980;77(10):5754-5758. PMID: 6777774
[5] Bohm M, et al. An overview of benefits and risks of chronic MC1R activation. JEADV. 2025;39:39-51. PMID: 39082868
[6] Minder EI, et al. Pharmacokinetics and Pharmacodynamics of Afamelanotide and Related Compounds. Clin Pharmacokinet. 2017;56(8):815-823.
[7] Hruby VJ, et al. Approaches to the rational design of selective melanocortin receptor antagonists. Expert Opin Drug Discov. 2015;10(10):1057-1069. PMC4608743
Mechanism and Receptor Pharmacology
[8] King SH, et al. Melanocortin receptors, melanotropic peptides and penile erection. Curr Top Med Chem. 2007;7(11):1098-1106. PMID: 17584130
[9] Mun Y, Kim W, Shin D. MC1R: Pharmacological and Therapeutic Aspects. Int J Mol Sci. 2023;24(15):12152. PMID: 37569558
Animal and Preclinical Studies
[15] Van der Klaauw A, et al. Role of melanocortin signaling in the preference for dietary macronutrients in human beings. Lancet. 2015;385(Suppl 1):S12.
[16] Shimizu H, Inoue K, Mori M. The leptin-dependent and -independent melanocortin signaling system: regulation of feeding and energy expenditure. J Endocrinol. 2007;193(1):1-9.
[17] Intermittent MTII Application Evokes Repeated Anorexia and Robust Fat and Weight Loss. PMC2860181
[18] Strand FL, et al. The Potent Melanocortin Receptor Agonist melanotan-II promotes peripheral nerve regeneration and has neuroprotective properties in the rat. PMID: 12591111
[19] Lau JKY, et al. Melanocortin receptor activation alleviates amyloid pathology and glial reactivity in an Alzheimer's disease transgenic mouse model. Sci Rep. 2021;11(1):4359. DOI: 10.1038/s41598-021-83932-4
[20] Giuliani D, et al. Multiple beneficial effects of MC4R agonists in experimental neurodegenerative disorders. PMID: 27916623
[21] Navarro M, et al. Evidence that Melanocortin Receptor Agonist Melanotan-II Synergistically Augments the Ability of Naltrexone to Blunt Binge-Like Ethanol Intake in Male C57BL/6J Mice. Alcohol Clin Exp Res. 2015;39(8):1425-1433.
[22] York DA, Boghossian S, Park-York M. Melanocortin activity in the amygdala influences alcohol intake. Pharmacol Biochem Behav. 2011;98(1):112-119.
[23] Minakova E, et al. Melanotan-II reverses autistic features in a maternal immune activation mouse model of autism. PLoS ONE. 2019;14(1). PMID: 30629642
Safety and Adverse Events
[24] Hjuler KF, Lorentzen HF. Melanoma associated with the use of melanotan-II. Dermatology. 2014;228:34-36. PMID: 24355990
[25] Mahieu et al. Changes of melanocytic lesions induced by Melanotan injections and sun bed use in a teenage patient with FAMMM syndrome. Dermatol Pract Concept. 2013;3(2):51-54. PMID: 23785612
[26] Habbema L, et al. Risks of unregulated use of alpha-MSH analogues: a review. Int J Dermatol. 2017;56(10):975-980. PMID: 28266027
[27] Nelson ME, et al. Melanotan II injection resulting in systemic toxicity and rhabdomyolysis. Clin Toxicol. 2012;50(10):1169-1173. PMID: 23121206
[28] Peters B, et al. Melanotan II: a possible cause of renal infarction. CEN Case Rep. 2020;9(2):159-161. PMID: 31953620
Related Peptide Guides
- Melanotan I — Linear, MC1R-selective analog. FDA/EMA-approved (Scenesse) for EPP. Same pharmacophore, different selectivity profile.
- PT-141 (Bremelanotide) — MC4R agonist derived directly from MT-II research. FDA-approved for HSDD. Focuses on sexual function without significant tanning.
- GHK-Cu — Copper peptide for skin rejuvenation. Listed in community stacking protocols with MT-II.
- KPV — Anti-inflammatory peptide. Skin health stack companion.
- BPC-157 — Regenerative peptide. Listed in community skin health combinations.
- Glutathione — Antioxidant. Complementary in skin health protocols.
- Oxytocin — Related through MT-II's oxytocin-releasing mechanism (autism/social behavior research).
- Semaglutide, Retatrutide, Cagrilintide — GLP-1 agonists. Alternative approaches for appetite/weight management.
- Tesofensine — Appetite suppressant listed in community stacking protocols.
Need the reconstitution math for Melanotan II: Complete Research Guide?
Open the calculator with Melanotan II: Complete Research Guide prefilled to estimate concentration, draw volume, and related measurement math from the reconstitution details you already have.