ARA-290 (Cibinetide): Complete Peptide Guide
On this page
Quick Reference Card
Attribute
Also Known As
- Detail
- Cibinetide, PH-BSP
Attribute
Administration
- Detail
- Injectable (subcutaneous)
Attribute
Research Status
- Detail
- Research Compound. FDA Orphan Drug and Fast Track designation for sarcoidosis-associated small fiber neuropathy. Not FDA-approved. Phase 3 trials not conducted due to funding constraints.
Attribute
Typical Dose Range
- Detail
- 2-4 mg daily (subcutaneous); 4 mg is the most commonly studied clinical dose
Attribute
Half-Life
- Detail
- Plasma half-life approximately 2-20 minutes; biological effects persist for hours due to sustained intracellular signaling
Attribute
Cycle Length
- Detail
- 4-8 weeks (28-84 days); typically used as a single defined course rather than continuous cycling
Attribute
Storage
- Detail
- Lyophilized: 2-8°C (up to 2 years) or -20°C (up to 3 years). Reconstituted: 2-8°C, use within 28 days. Protect from light.
Overview / What Is ARA-290?
The Basics
ARA-290 is a synthetic peptide with a very specific job: activating your body's built-in tissue repair system without the baggage that comes with the hormone it was derived from.
Your body already produces a hormone called erythropoietin (EPO) that does two things. The well-known function is making red blood cells. The lesser-known function is protecting and repairing damaged tissue, especially nerve tissue. The problem is, you can't use EPO for tissue repair without also getting the red blood cell effects, which can thicken your blood and increase clotting risks.
ARA-290 was engineered to solve this problem. Researchers mapped EPO's three-dimensional shape and identified the exact surface region responsible for tissue repair. They then built a small 11-amino-acid peptide that mimics only that repair surface. The result is a molecule that triggers the same protective and regenerative pathways as EPO, but without any effect on red blood cell production.
What makes ARA-290 particularly notable in the peptide landscape is its clinical data. Unlike many research peptides with only animal studies, ARA-290 has been tested in multiple Phase 2 human clinical trials. In patients with sarcoidosis-related small fiber neuropathy, it demonstrated something remarkable: measurable nerve fiber regrowth, confirmed by microscopy. This is not symptom suppression or pain masking. It is biological reversal of nerve damage.
The compound earned FDA Fast Track and Orphan Drug designations for sarcoidosis, but development stalled after 2020 when its developer, Araim Pharmaceuticals, ran out of funding before reaching Phase 3 trials. The science was successful; the business model was not.
The Science
ARA-290 (cibinetide) is a synthetic 11-amino acid peptide (sequence: pGlu-Glu-Leu-Glu-Arg-Ala-Leu-Asn-Ser-Ser) derived from the helix B surface domain of human erythropoietin [1]. The peptide was rationally designed based on the three-dimensional structure of EPO, specifically the surface that contacts the innate repair receptor (IRR) rather than the classical erythropoietin receptor responsible for erythropoiesis [2].
Unlike EPO, which binds to EPOR homodimers on erythroid progenitor cells in bone marrow to stimulate red blood cell production, ARA-290 selectively engages the EPOR-CD131 (beta-common receptor) heterodimer, a distinct receptor complex known as the innate repair receptor [2]. This receptor complex is not constitutively expressed on healthy tissues but is rapidly upregulated in response to injury, inflammation, hypoxia, or metabolic stress [3].
The peptide has progressed through multiple Phase 2 clinical trials for sarcoidosis-associated small fiber neuropathy (NCT02039687), Type 2 diabetic neuropathy, and diabetic macular edema [4][5]. It received US and EU Orphan Drug Designation and US FDA Fast Track Designation for sarcoidosis. The molecular formula is C51H84N16O21 with a molecular weight of 1257.3 g/mol (CAS No: 1208243-50-8; PubChem CID: 91810664) [6].
Molecular Identity
Attribute
Amino Acid Sequence
- Value
- pGlu-Glu-Leu-Glu-Arg-Ala-Leu-Asn-Ser-Ser (ZEQLERALNSS)
Attribute
Number of Amino Acids
- Value
- 11
Attribute
Molecular Formula
- Value
- C51H84N16O21
Attribute
Molecular Weight
- Value
- 1257.3 g/mol
Attribute
CAS Number
- Value
- 1208243-50-8
Attribute
PubChem CID
- Value
- 91810664
Attribute
Synonyms
- Value
- Cibinetide, PH-BSP
Attribute
Origin
- Value
- Derived from the helix B surface domain of erythropoietin
Attribute
Classification
- Value
- Non-erythropoietic EPO-derived tissue-protective peptide
Mechanism of Action
The Basics
To understand how ARA-290 works, think of your body as having a damage detection system. When tissue gets injured, whether from inflammation, low oxygen, nerve damage, or metabolic stress, cells in the affected area put up a distress signal by expressing a special receptor on their surface. This receptor only appears where there is actual damage.
ARA-290 is specifically shaped to activate this distress receptor. When it does, three important things happen. First, it tells damaged cells to survive rather than self-destruct. Second, it dials down the inflammatory response that can become self-perpetuating and cause additional damage. Third, it signals for repair resources, including stem cells and improved blood flow, to be directed toward the injured area.
The key advantage of this approach is precision. Because the receptor only appears where damage exists, ARA-290's effects are concentrated where they are needed most. Healthy tissue without the receptor is essentially invisible to the peptide.
This explains why ARA-290 does not increase red blood cell production. The receptor configuration in bone marrow that drives red blood cell production is completely different from the damage-sensing receptor that ARA-290 targets. The peptide simply cannot interact with the blood-making machinery.
The Science
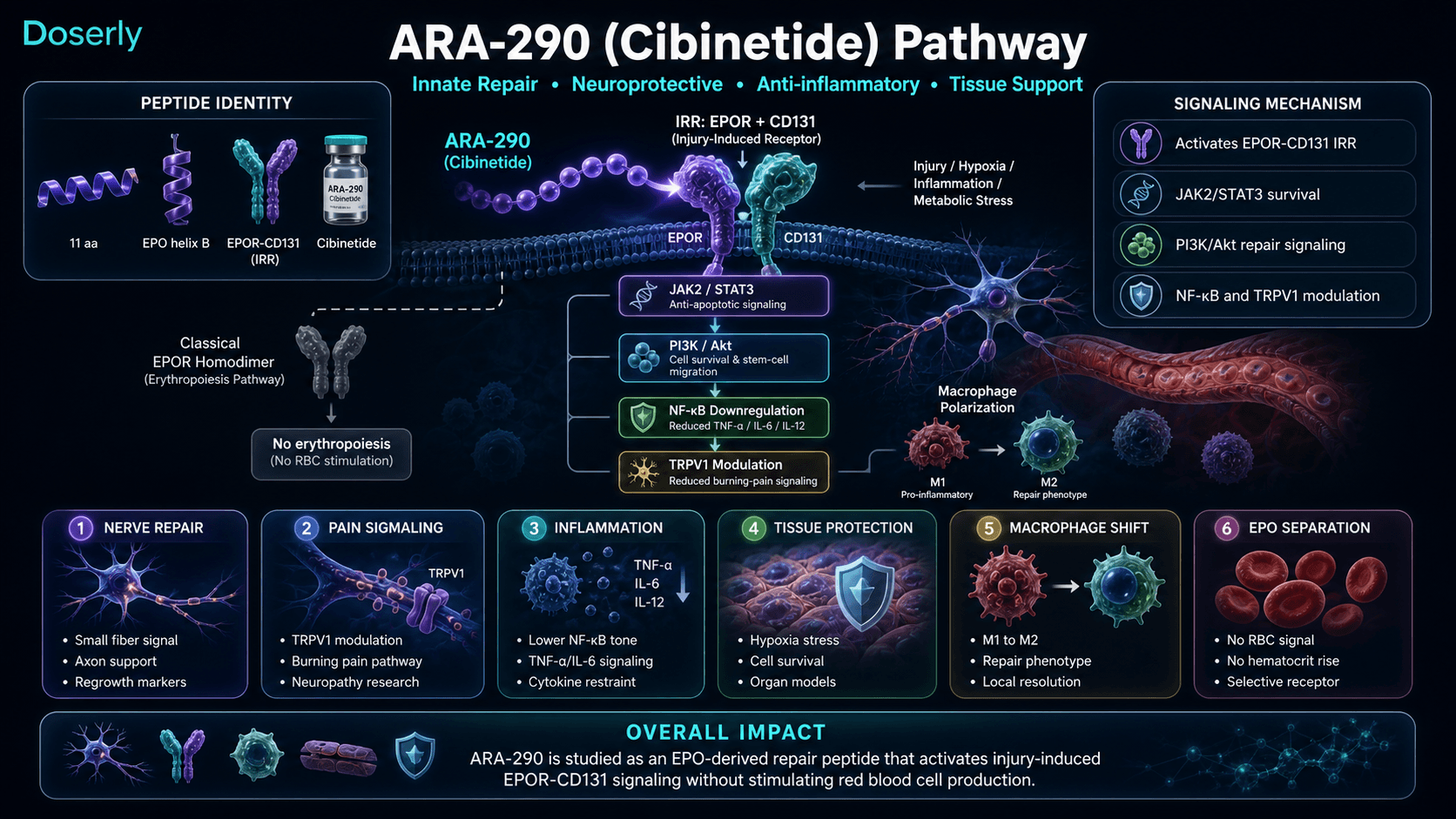
ARA-290 activates the innate repair receptor (IRR), a heterodimer composed of the erythropoietin receptor (EPOR) and CD131 (beta-common receptor, also known as the beta-c or IL-3/IL-5/GM-CSF receptor common beta chain) [2][3]. This receptor complex is distinct from the EPOR homodimer expressed on erythroid progenitor cells that mediates erythropoiesis.
The IRR is not constitutively expressed on healthy tissues. It is rapidly induced in response to tissue injury signals including inflammation, hypoxia, and metabolic stress, functioning as an endogenous damage sensor [3]. CD131 knockout studies confirm this receptor specificity: animals lacking the beta-common receptor subunit lose all tissue-protective effects from ARA-290 while erythropoiesis continues normally [2].
Upon binding the IRR, ARA-290 initiates several downstream signaling cascades:
- JAK2/STAT3 signaling: Activates anti-apoptotic gene expression, rescuing damaged cells from programmed cell death [1][2]
- PI3K/Akt pathway: Modulates cell survival, promotes stem cell migration toward injury sites, and enhances regional blood flow [2]
- NF-kB downregulation: Reduces production of pro-inflammatory cytokines, particularly TNF-alpha, IL-6, and IL-12 [7][8]
- TRPV1 channel inhibition: Directly inhibits the capsaicin receptor responsible for heat and burning pain perception, providing analgesic effects independent of anti-inflammatory action [9]
- M1-to-M2 macrophage polarization: Shifts local macrophage phenotype from pro-inflammatory to pro-reparative, promoting tissue healing rather than continued inflammatory damage [10]
These combined effects confer anti-inflammatory, neuroprotective, and tissue-reparative properties without stimulating erythropoiesis. The absence of erythropoietic activity has been confirmed in all clinical trials by the lack of changes in hemoglobin, hematocrit, or red blood cell counts [4][5].
Pathway Visualization Image
Pharmacokinetics
The Basics
ARA-290 has an unusually short time in the bloodstream. After injection, it clears from your blood within minutes. At first glance, this might seem like a problem, but the biology tells a different story.
Think of ARA-290 like a key that turns on a lock and then walks away. The lock stays engaged long after the key is gone. When ARA-290 activates its target receptor, it triggers internal cell signaling cascades that continue working for hours or even days after the peptide itself has been cleared. The receptor essentially acts as a molecular switch that stays in the "on" position.
This is why a single daily injection is effective despite the very short plasma half-life. The peptide only needs to be present long enough to activate the receptor. After that, the repair signaling sustains itself.
After a 4 mg subcutaneous injection, peak blood levels reach about 3 nanograms per milliliter. This comfortably exceeds the minimum concentration needed to activate the receptor, which is approximately 1 nanomolar.
The Science
ARA-290 exhibits a paradoxically short plasma half-life of approximately 2-20 minutes following subcutaneous administration [3][11]. Despite this rapid clearance, biological effects persist for hours to days because receptor activation triggers sustained intracellular signaling cascades. The IRR functions as a molecular switch: ligand binding initiates downstream JAK2/STAT3 and PI3K/Akt signaling that persists independently of continued receptor occupancy [3].
Following a 4 mg subcutaneous dose, peak plasma concentration (Cmax) reaches approximately 3 ng/mL (2.4 nmol/L), which exceeds the minimum effective concentration of approximately 1 nmol/L required for IRR activation [11]. The time to peak concentration (Tmax) occurs within minutes of injection.
The disconnect between pharmacokinetic half-life and pharmacodynamic duration is well-characterized. In clinical trials, daily dosing at 4 mg produced sustained therapeutic effects, and some clinical endpoints (corneal nerve fiber density, Small Fiber Neuropathy Screening List scores) continued to improve even after dosing cessation [4][5]. This suggests that ARA-290 initiates repair processes that are self-sustaining once triggered.
Pharmacokinetics informed clinical trial dose selection: 1 mg, 4 mg, and 8 mg daily doses were tested, with 4 mg producing the optimal efficacy signal and 8 mg offering no additional benefit [5].
Consistency is the difference between a protocol that delivers results and one that wastes time and money. Doserly was built for exactly this: keeping you on track with the precision your protocol demands.
The built-in calculators handle the math you shouldn't be doing in your head. The reconstitution calculator tells you exactly how much bacteriostatic water to add for your target concentration. The dose calculator converts between units, milligrams, and syringe markings so you draw the right amount every time. The injection site heat map tracks where you've administered and when, helping you rotate sites systematically to reduce tissue damage, scarring, and absorption inconsistencies from overusing the same area. Pair that with smart reminders tuned to your protocol's timing requirements, and you build the kind of daily consistency that separates optimized protocols from haphazard ones.
Build reminders around the routine, not just the compound.
Doserly can keep timing, skipped doses, and schedule changes organized so the plan you read about becomes easier to follow and review.
Today view
Upcoming reminders

Reminder tracking supports consistency; it does not select a protocol for you.
Research & Clinical Evidence
ARA-290 and Small Fiber Neuropathy (Sarcoidosis)
The Basics
The strongest human evidence for ARA-290 comes from patients with sarcoidosis, an inflammatory condition that can destroy small sensory nerves in the skin. These tiny nerves are responsible for temperature sensation, pain perception, and autonomic functions like sweating. When they die back, patients experience burning pain, numbness, tingling, and dysfunction that conventional pain medications can only mask, not reverse.
In clinical trials, ARA-290 did something that no other treatment has demonstrated: it measurably regrew these damaged nerve fibers. Using microscopy to count nerve fibers in the cornea and skin, researchers documented actual increases in nerve fiber density, not just symptom improvement but biological repair.
The Science
DOSARA Trial (Phase 2b, n=64): Patients received subcutaneous cibinetide at 1 mg, 4 mg, or 8 mg daily for 28 days versus placebo. The 4 mg dose group showed a 23% increase in corneal nerve fiber area versus baseline, confirmed by corneal confocal microscopy. Skin punch biopsies revealed increases in GAP-43 positive nerve fibers, a marker of active nerve regeneration rather than mere nerve survival [4][5].
Pilot Study (n=22): The earlier proof-of-concept trial demonstrated that ARA-290 patients achieved an 11.5-point improvement in Small Fiber Neuropathy Screening List (SFNSL) scores versus 2.9 points for placebo. 42% of ARA-290 patients achieved clinically meaningful 15+ point improvements versus 0% in the placebo group [12].
Notably, clinical improvements persisted after dosing cessation. SFNSL improvements were maintained at 16 weeks (12 weeks post-dosing), and corneal nerve fiber density continued to improve after treatment completion, suggesting that ARA-290 triggers a self-sustaining repair process [4].
ARA-290 and Type 2 Diabetes
The Basics
Beyond neuropathy, ARA-290 has shown promise in improving metabolic markers in people with Type 2 diabetes. In a clinical trial, participants receiving ARA-290 showed improvements in HbA1c levels (a measure of long-term blood sugar control), lipid profiles, and neuropathic symptoms. This dual benefit, addressing both metabolic dysfunction and nerve damage, is particularly relevant because diabetic neuropathy is one of the most common complications of diabetes.
The Science
In a Phase 2 trial involving approximately 40 Type 2 diabetes patients, ARA-290 (4 mg daily for 28 days) improved HbA1c levels, lipid profiles, and corneal nerve fiber density in patients with baseline deficits [13]. These results suggest that IRR activation may influence metabolic pathways beyond pure neuroprotection, possibly through anti-inflammatory modulation of insulin signaling and pancreatic beta cell protection.
ARA-290 and Tissue Protection (Preclinical)
The Basics
Animal studies have shown that ARA-290 can protect multiple organ systems during injury. In kidney transplant models, it reduced the damage caused by temporary blood flow interruption. In heart attack models, it reduced the size of the damaged area. It has also shown neuroprotective effects in stroke and traumatic brain injury models, and it appears to cross the blood-brain barrier, meaning it can potentially protect brain tissue directly.
The Science
Preclinical evidence spans multiple organ systems:
- Renal protection: ARA-290 attenuates ischemia-reperfusion injury in kidney transplant models by targeting the NF-kB pathway, reducing inflammatory infiltration and fibrosis [14]
- Cardiac protection: A 2023 mouse study demonstrated that ARA-290 reduced cardiac aging hallmarks and preserved ejection fraction [3]
- Cerebral protection: A 2024 study confirmed brain tissue protection through the beta-common receptor in ischemic stroke models [15]
- Endothelial protection: ARA-290 enhances endothelial colony-forming cell proliferation, migration, and homing ability, suggesting potential applications in vascular repair and retinal ischemia [16][17]
- Islet transplantation: ARA-290 inhibits macrophage activation and prolongs transplanted islet cell survival by suppressing inflammatory cytokines (IL-6, IL-12, TNF-alpha) [10]
- Autoimmune disease: In lupus models, ARA-290 suppressed autoantibody levels (ANA, anti-dsDNA) and reduced kidney damage [18]
- Inflammatory bowel disease: Cibinetide dampened innate immune cell functions and ameliorated experimental colitis [19]
Biomarker Evidence Matrix
Category
Pain Management
- Evidence Strength
- 8/10
- Reported Effectiveness
- 7/10
- Summary
- Multiple Phase 2 human trials demonstrate significant neuropathic pain reduction. Community reports consistent with clinical data, particularly for burning and tingling symptoms.
Category
Inflammation
- Evidence Strength
- 7/10
- Reported Effectiveness
- 6/10
- Summary
- Strong preclinical evidence across multiple inflammatory models. NF-kB downregulation and cytokine suppression well-documented. Community reports limited but positive.
Category
Longevity & Neuroprotection
- Evidence Strength
- 8/10
- Reported Effectiveness
- 7/10
- Summary
- Corneal nerve fiber regrowth confirmed by confocal microscopy in human trials, representing a first-in-class demonstration. Community members specifically cite nerve regeneration as primary motivation.
Category
Recovery & Healing
- Evidence Strength
- 6/10
- Reported Effectiveness
- 6/10
- Summary
- Preclinical evidence across multiple tissue types (kidney, cardiac, vascular). Community reports suggest improved recovery when paired with structural repair compounds.
Category
Side Effect Burden
- Evidence Strength
- 9/10
- Reported Effectiveness
- 8/10
- Summary
- Clinical trials consistently show adverse events comparable to placebo. No hematological changes, no antibody formation. Community confirms excellent tolerability.
Category
Immune Function
- Evidence Strength
- 6/10
- Reported Effectiveness
- N/A
- Summary
- Preclinical evidence for immune modulation (macrophage polarization, dendritic cell modulation, T-cell regulation). No community data on immune-specific outcomes.
Category
Daily Functioning
- Evidence Strength
- 5/10
- Reported Effectiveness
- 6/10
- Summary
- No direct clinical endpoints for daily functioning, but trial outcomes (pain reduction, nerve regrowth) imply functional improvements. Community reports meaningful quality-of-life gains.
Category
Heart Health
- Evidence Strength
- 5/10
- Reported Effectiveness
- N/A
- Summary
- Preclinical cardiac protection data (reduced infarct size, preserved ejection fraction in aging mice). No human cardiovascular outcome data or community reports.
Category
Treatment Adherence
- Evidence Strength
- N/A
- Reported Effectiveness
- 4/10
- Summary
- Not a clinical endpoint. Community reports highlight cost ($600-700/month) as the primary barrier to sustained use, not tolerability or protocol complexity.
Categories with insufficient data for scoring: Fat Loss, Muscle Growth, Weight Management, Appetite & Satiety, Food Noise, Energy Levels, Sleep Quality, Focus & Mental Clarity, Memory & Cognition, Mood & Wellbeing, Anxiety, Stress Tolerance, Motivation & Drive, Emotional Aliveness, Emotional Regulation, Libido, Sexual Function, Joint Health, Physical Performance, Gut Health, Digestive Comfort, Nausea & GI Tolerance, Skin Health, Hair Health, Blood Pressure, Heart Rate & Palpitations, Hormonal Symptoms, Temperature Regulation, Fluid Retention, Body Image, Bone Health, Cravings & Impulse Control, Social Connection, Withdrawal Symptoms.
Benefits & Potential Effects
The Basics
ARA-290's primary benefits center on three connected areas: nerve repair, pain reduction, and tissue protection during inflammatory conditions.
For neuropathic pain, ARA-290 appears to address the root cause rather than just masking symptoms. Where drugs like gabapentin and pregabalin modulate pain signals without addressing underlying nerve damage, ARA-290's clinical data suggests it can promote actual nerve fiber regrowth. This is a fundamentally different approach, and it is why the compound generates interest among people whose neuropathy has not responded to conventional treatments.
The anti-inflammatory effects are broad-based. By calming down overactive inflammatory signaling (particularly the NF-kB pathway), ARA-290 may help create the conditions for healing across multiple tissue types. This is why preclinical research has explored it for conditions as diverse as kidney transplant protection, heart attack recovery, and inflammatory bowel disease.
One additional benefit worth noting: ARA-290 carries none of the risks associated with EPO. There is no blood thickening, no increased clotting risk, no need for hemoglobin monitoring. This safety advantage is a direct result of its selective receptor targeting.
The Science
Published benefits from clinical and preclinical research include:
- Neuropathic pain reduction: Statistically significant improvements in PainDetect scores and SFNSL scores in sarcoidosis patients receiving 4 mg daily [4][5][12]
- Small fiber nerve regeneration: 23% increase in corneal nerve fiber area confirmed by confocal microscopy; increased GAP-43 positive nerve fibers in skin biopsies [4]
- Metabolic improvement: Improved HbA1c and lipid profiles in Type 2 diabetes patients [13]
- Endothelial protection: Enhanced endothelial colony-forming cell survival, proliferation, and homing in ischemic retina models [16][17]
- Immune modulation: Macrophage polarization from M1 (pro-inflammatory) to M2 (pro-reparative), reduced inflammatory cytokine secretion, modulated dendritic cell antigen presentation [7][10]
- Organ protection: Reduced ischemia-reperfusion injury in renal transplant models [14], cardiac protection in aging mouse models [3], neuroprotection in stroke models [15]
- Absence of erythropoietic effects: No changes in hemoglobin, hematocrit, or red blood cell counts across all clinical trials [4][5][13]
Side Effects & Safety Considerations
The Basics
ARA-290 has one of the cleaner safety profiles among research peptides, backed by actual human clinical trial data rather than just preclinical studies.
In multiple Phase 2 trials, the rate of adverse events in patients receiving ARA-290 was comparable to the rate in patients receiving placebo. The most commonly reported side effects were mild injection site reactions (redness, brief discomfort at the injection site) and occasional transient headaches. These are minor and consistent with what is seen with any subcutaneous injection.
The critical safety advantage over its parent molecule EPO deserves emphasis: ARA-290 does not increase red blood cell production. This means no risk of polycythemia (dangerously thick blood), no increased thrombosis risk, no hypertension from blood volume overload, and no need for regular hemoglobin monitoring. Blood labs in clinical trial participants confirmed zero hematological changes.
No participants in clinical trials developed antibodies against ARA-290, which is relevant because anti-drug antibodies can reduce effectiveness over time and potentially cause safety issues.
One caution worth noting from community reports: a user with Sjogren's disease (an autoimmune condition) experienced painful nerve flares at doses of 2 mg and above. While this is a single report, it suggests that individuals with active autoimmune processes may respond unpredictably, and starting at lower doses with careful monitoring may be prudent.
The Science
Safety data from multiple Phase 2 clinical trials:
- Adverse event frequency was comparable between ARA-290 and placebo groups across all trials [4][5][12]
- No clinically significant hematological changes were observed, confirming absence of erythropoietic activity (no changes in hemoglobin, hematocrit, RBC counts, or reticulocyte counts) [4][5]
- No anti-cibinetide antibodies were detected in any trial participants [4]
- Injection site reactions (mild pain, transient redness) occurred at rates similar to placebo [4][5]
- No dose-limiting toxicity was observed at doses up to 8 mg daily [5]
Safety Concern
Thrombosis
- EPO
- Increased risk
- ARA-290
- Not observed
Safety Concern
Polycythemia
- EPO
- Can occur
- ARA-290
- Not observed
Safety Concern
Hypertension
- EPO
- Can occur
- ARA-290
- Not observed
Safety Concern
Pure red cell aplasia
- EPO
- Risk with antibody formation
- ARA-290
- Not applicable (no antibodies detected)
Safety Concern
Hemoglobin monitoring
- EPO
- Required
- ARA-290
- Not required
Limitations: Clinical trial durations were 4-12 weeks. No long-term safety data beyond clinical trial follow-up periods exists. The total number of human subjects exposed to ARA-290 across all trials is relatively small (fewer than 200). Post-marketing surveillance data does not exist since the compound never reached market approval.
The side effects and contraindications above give you a map of what to watch for. Doserly turns that map into a daily practice. Log the specific biomarkers and symptoms associated with this compound's known risk profile, and the app builds a timeline of how your body is responding across your cycle.
Trending in the wrong direction on a key marker? Noticing a pattern that started two weeks into your protocol? Doserly connects the dots between your protocol timeline and your logged data, making it easier to spot emerging issues early and have informed, data-backed conversations with your healthcare provider about what's working and what needs attention.
Capture changes while they are still fresh.
Log symptoms, energy, sleep, mood, and other observations alongside protocol events so patterns do not live only in memory.
Trend view
Symptom timeline

Symptom tracking is informational and should be interpreted with a qualified clinician.
Dosing Protocols
The Basics
ARA-290 dosing is relatively straightforward compared to many peptides. The most commonly studied protocol in clinical trials was 4 mg injected subcutaneously once per day for 28 days. This is the dose that showed the strongest efficacy signal across multiple trials, and doses up to 8 mg did not provide additional benefit.
Some community members and practitioners suggest starting at 2 mg daily during the first week to assess tolerance before moving up to the full 4 mg dose. This is a reasonable precaution, though clinical trials did not observe dose-dependent side effects.
Cycle length in clinical trials was typically 4 weeks, though some protocols extended to 8 weeks. ARA-290 is generally used as a defined course rather than continuous indefinite therapy. Benefits have been documented to persist for months after a course ends, which suggests that repeat courses may only be needed if symptoms return, typically after 3-6 months.
Commonly reported dosing ranges from sources:
Protocol
Clinical trial standard
- Dose
- 4 mg
- Frequency
- Once daily, subcutaneous
- Duration
- 28 days
- Notes
- Most commonly studied; strongest efficacy signal
Protocol
Titration approach
- Dose
- 2 mg (week 1), then 4 mg
- Frequency
- Once daily, subcutaneous
- Duration
- 4-8 weeks
- Notes
- Allows tolerance assessment
Protocol
Extended protocol
- Dose
- 4 mg
- Frequency
- Once daily, subcutaneous
- Duration
- 8-16 weeks
- Notes
- Based on clinical response; not formally studied beyond 12 weeks
Protocol
Maximum studied
- Dose
- 8 mg
- Frequency
- Once daily, subcutaneous
- Duration
- Up to 4 weeks
- Notes
- No additional benefit over 4 mg in clinical data
The Science
Clinical dose-ranging data from the DOSARA trial (NCT02039687) tested 1 mg, 4 mg, and 8 mg daily subcutaneous doses against placebo over 28 days [5]. The 4 mg dose produced the clearest efficacy signal across endpoints including corneal nerve fiber area, PainDetect scores, and SFNSL scores. The 1 mg dose showed smaller signals, and the 8 mg dose offered no advantage over 4 mg [5].
The paradox of effective daily dosing despite a 2-20 minute plasma half-life is explained by the receptor-mediated "molecular switch" mechanism: a single daily pulse of sufficient concentration to activate the IRR triggers intracellular signaling cascades that persist independently of continued ligand presence [3][11].
No dose-limiting toxicities were observed at any tested dose [5]. The most commonly cited range in published literature is 2-4 mg daily, with 4 mg as the established target therapeutic dose [4][5][13].
What to Expect
The following timeline is derived from clinical trial data and community reports. Individual responses will vary based on the type and severity of the underlying condition, overall health status, and concurrent treatments.
Weeks 1-2
The innate repair receptor begins activating at injury sites. Anti-apoptotic signaling cascades engage, and the local inflammatory environment starts shifting from pro-inflammatory toward pro-reparative. Some individuals report sensory symptoms beginning to quiet, with less burning and tingling. Clinical trials showed the earliest symptom improvements beginning around day 12 in some patients. This is a period of internal reorganization rather than dramatic external change.
Weeks 2-4
Small fiber protection becomes established. M1-to-M2 macrophage polarization takes effect locally. Most individuals who will respond report noticeable reductions in neuropathic symptoms during this window. Tingling may decrease, movement may feel less guarded, and pain-related avoidance behaviors may begin to relax. Clinical trial data shows statistically significant improvements in pain scores by week 4.
Weeks 4-8
For those continuing beyond the standard 28-day protocol, nerve regeneration support continues. Proprioception improvements may become noticeable, with better balance, coordination, and confidence during physical activities. Corneal nerve fiber density continues to increase during this period in clinical data.
After Stopping
One of ARA-290's most distinctive features is that benefits persist well after the last dose. In clinical trials, PainDetect improvements were maintained at 8 weeks (4 weeks after dosing ended). SFNSL improvements were maintained at 16 weeks (12 weeks post-dosing). Corneal nerve fiber density continued to improve even after dosing stopped. This pattern strongly suggests that ARA-290 triggers a repair process that becomes self-sustaining once initiated.
If symptoms eventually return, most sources suggest that repeat courses may be considered after 3-6 months, though long-term cycling protocols have not been formally studied.
The week-by-week expectations above are drawn from research and community reports, but your experience will be uniquely yours. Doserly's biomarker tracking transforms those general timelines into personal data points you can actually see and measure.
Log the specific markers relevant to this compound, whether that's pain levels, energy, sleep quality, body composition, recovery time, or mood, and watch your own trend lines emerge over weeks and months. Did your key markers start shifting in week three, like the research suggests? Is your experience tracking with what the community reports, or diverging? Over time, this creates something more valuable than any guide: an evidence-based picture of how your body responds to this specific compound, at your specific dose, within your specific health context.
See where a dose, cycle, or change fits in time.
Doserly gives each protocol a timeline so dose changes, pauses, restarts, and observations are easier to compare later.
Timeline
Cycle history

Timeline tracking helps with recall; it is not a treatment recommendation.
Interaction Compatibility
Good With (Synergistic Compounds)
- BPC-157: Complementary mechanisms. BPC-157 promotes vascular access and tissue repair at the structural level, while ARA-290 targets nerve repair and anti-inflammatory signaling. Recommended when nerve pain coexists with structural tissue damage.
- TB-500: Enhances cellular mobility and the overall healing environment. Combined with ARA-290, it addresses the structural and neural components of recovery simultaneously.
- GHK-Cu: Connective tissue and repair signaling support. One community member reported success using intranasal ARA-290 combined with GHK-Cu for nerve pain from spinal stenosis.
- KPV: Anti-inflammatory gut-immune support. Complementary anti-inflammatory pathway (alpha-MSH derived) that does not overlap with IRR activation.
- MOTS-C: Mitochondrial resilience support. Addresses cellular energy metabolism that can support nerve repair processes.
- SS-31: Mitochondrial membrane stabilization. Useful if healing has stalled after 4+ weeks, as mitochondrial oxidative damage can become a bottleneck during prolonged repair.
- NAD+: Metabolic support during nerve repair. NAD+ levels decline with age and are critical for cellular repair processes.
- Tesamorelin: Compatible (different pathways). Tesamorelin supports GH-axis function at night; ARA-290 targets nerve repair in the morning. No interference between the two.
- Sermorelin: Compatible as part of a broader recovery or anti-aging stack.
Not Good With (Caution)
- Erythropoietin (EPO): While ARA-290 does not stimulate erythropoiesis, combining it with EPO could theoretically create complex receptor competition at the EPOR-CD131 heterodimer. No data exists on this combination.
- Immunosuppressive medications: ARA-290 modulates immune function. Combining with strong immunosuppressants (cyclosporine, tacrolimus) may produce unpredictable interactions with immune cell signaling. No clinical data on these combinations exists.
- Active autoimmune flares: Community reports suggest that individuals with active autoimmune conditions (particularly Sjogren's disease) may experience symptom flares when starting ARA-290, possibly due to immune modulation in an already dysregulated immune system.
Administration Guide
Materials typically used:
- U-100 insulin syringes (29-31 gauge, 1/2" needle)
- Alcohol swabs (for vial stopper and injection site)
- Sharps container for needle disposal
Reconstitution solution:
Sources differ on the ideal reconstitution solution. The compound's published patent and clinical trial protocols specify Phosphate Buffered Saline (PBS). Some practitioners recommend bacteriostatic water with sodium chloride (isotonic) as an alternative that may reduce injection site sting. Community members have reported occasional solubility challenges with standard bacteriostatic water alone. Readers should discuss reconstitution options with their healthcare provider or pharmacist.
Timing considerations:
- Most sources suggest morning administration on an empty stomach for optimal absorption
- Consistent daily timing is recommended for protocol consistency
- Time of day is described as flexible by some sources, though morning dosing is most commonly cited
Post-administration care:
- Mild injection site redness or discomfort may occur and typically resolves within minutes to hours
- No specific post-injection monitoring is required for routine use
- Baseline and follow-up labs recommended by some practitioners: CBC with hematocrit (to confirm absence of erythropoietic effect), CMP, and inflammatory markers (CRP, ESR) where applicable
Supplies & Planning
Typical vial sizes available:
- 10 mg vials
- 16 mg vials (commonly referenced in dosing protocols)
General supplies associated with ARA-290 protocols:
- Peptide vials (quantity depends on dose and duration; consult with healthcare provider)
- Bacteriostatic water or Phosphate Buffered Saline for reconstitution
- U-100 insulin syringes (one per daily injection)
- Alcohol swabs (two per injection: one for vial stopper, one for injection site)
- Sharps container for needle disposal
Cost considerations:
Community members consistently note that ARA-290 is one of the more expensive research peptides. Reports cite costs of $600-700 per month at 4 mg daily from domestic suppliers. Availability may also be inconsistent, as the compound is less widely stocked than more mainstream peptides.
For exact reconstitution volumes and injection calculations based on specific vial sizes, readers can use the reconstitution calculator available through the Doserly app.
Storage & Handling
Lyophilized (powder) form:
- Refrigerate at 2-8°C (35.6-46.4°F) for up to 2 years
- Freeze at -20°C (-4°F) for extended storage up to 3 years
- Keep in original sealed packaging with desiccant to minimize moisture exposure
- Protect from light
Reconstituted (liquid) form:
- Refrigerate at 2-8°C (35.6-46.4°F)
- Use within 28 days of reconstitution
- Do not freeze reconstituted solution (freezing denatures peptides)
- Allow vials to reach room temperature before opening to minimize condensation
- Discard if any discoloration, cloudiness, or particulate matter is observed
General handling:
- Label vials with reconstitution date immediately after preparation
- Use a new sterile syringe for each injection
- Follow standard aseptic technique when accessing vials
Lifestyle Factors
Lifestyle factors that may complement an ARA-290 protocol, based on available research and community discussion:
Glycemic management: For individuals addressing diabetic neuropathy, optimizing blood sugar control through diet and medication adherence is consistently cited as essential. Community members and clinical literature both note that running ARA-290 while blood sugar remains uncontrolled limits results significantly.
Physical activity: Regular physical activity appropriate to individual capacity supports nerve health and peripheral circulation. Walking, light resistance training, and balance exercises may complement nerve regeneration effects. The goal is to maintain blood flow and neural signaling to the extremities without overloading damaged nerves.
Sleep and recovery: Adequate sleep supports tissue repair processes. Sleep is when many regenerative pathways are most active, making it a relevant consideration during a nerve repair protocol.
Substance avoidance: Alcohol and smoking are both directly neurotoxic and can worsen neuropathic conditions. Limiting or eliminating these during an ARA-290 protocol may improve outcomes.
Stress management: Chronic stress elevates inflammatory markers that can counteract ARA-290's anti-inflammatory effects. Stress reduction practices may support the repair environment that ARA-290 is designed to promote.
Addressing root causes: Multiple sources emphasize that ARA-290 works best when the underlying cause of nerve damage is addressed simultaneously. Continuing toxic exposures, maintaining uncontrolled inflammation, or ignoring metabolic dysfunction while using ARA-290 limits the compound's potential.
Regulatory Status & Research Classification
United States (FDA):
- Not FDA-approved for any indication
- FDA Orphan Drug Designation for sarcoidosis-associated small fiber neuropathy (granted 2016)
- FDA Fast Track Designation for sarcoidosis-associated small fiber neuropathy
- Successful End-of-Phase 2 FDA meeting completed (2017)
- Multiple Phase 2 clinical trials completed (ClinicalTrials.gov: NCT02039687 and others)
- No Phase 3 trials registered or announced
- Currently available only as a research chemical
European Union (EMA):
- EU Orphan Drug Designation for sarcoidosis
- EU Orphan Designation for pancreatic islet transplantation
- Not approved for marketing
Development status:
- Araim Pharmaceuticals (the developer and patent holder) shows no public activity since approximately July 2020
- Total funding of approximately $8.1 million (insufficient for Phase 3 trials, which typically require $50-100 million or more)
- The company had 1-10 employees as of last public update
- No pharmaceutical partner or licensee has been announced
WADA status: ARA-290 is not explicitly listed on the WADA prohibited list. However, athletes should verify current status independently as regulatory classifications change.
Active academic research: Despite commercial development stalling, academic research on ARA-290 and the IRR mechanism continues. A 2023 study demonstrated cardiac protection effects in aging mice. A 2024 study confirmed brain tissue protection through the beta-common receptor in stroke models.
Regulatory status changes frequently. Always verify the current legal status of any compound in your specific country or jurisdiction before making any decisions.
FAQ
What is ARA-290 and how does it differ from EPO?
ARA-290 (cibinetide) is an 11-amino acid synthetic peptide derived from the tissue-protective region of erythropoietin (EPO). Unlike EPO, which stimulates red blood cell production and carries risks of blood thickening and thrombosis, ARA-290 selectively activates the innate repair receptor (IRR) for tissue protection and nerve repair without any effect on red blood cell counts. It was specifically engineered to deliver EPO's protective benefits while eliminating its hematological side effects.
What conditions has ARA-290 been studied for?
ARA-290 has been tested in Phase 2 human clinical trials for sarcoidosis-associated small fiber neuropathy, Type 2 diabetic neuropathy, and diabetic macular edema. Preclinical (animal) research has explored kidney protection during transplantation, cardiac protection, stroke neuroprotection, inflammatory bowel disease, and systemic lupus erythematosus.
What dosing protocols are commonly reported in available research?
Based on published clinical trial data, the most commonly studied protocol involves 4 mg administered subcutaneously once daily for 28 days. Some sources describe starting at 2 mg during the first week for tolerance assessment before increasing to 4 mg. Doses up to 8 mg daily were tested in clinical trials without dose-limiting toxicity, though no additional benefit over 4 mg was observed. Readers should consult with a qualified healthcare professional for guidance specific to their situation.
How long do the effects of ARA-290 last after stopping?
Clinical trial data suggests that benefits can persist for months after a course ends. In the sarcoidosis trials, pain score improvements were maintained at 8 weeks (4 weeks after dosing stopped), and nerve fiber density continued to improve even after treatment completion. This pattern suggests ARA-290 triggers a self-sustaining repair process rather than providing only transient symptom relief.
Why isn't ARA-290 FDA-approved despite positive trial results?
The developer, Araim Pharmaceuticals, appears to have run out of funding before conducting the Phase 3 trials required for FDA approval. The company had total funding of approximately $8.1 million, which is insufficient for Phase 3 trials (typically $50-100 million or more). The scientific evidence was promising; the commercial development stalled for financial, not scientific, reasons.
Can ARA-290 be combined with other peptides?
Based on available information, ARA-290 is commonly discussed in combination with BPC-157 and TB-500, which address structural tissue repair while ARA-290 targets nerve repair. NAD+ is sometimes mentioned for metabolic support during nerve repair. These compounds work through different pathways and are generally considered non-overlapping. However, no formal studies have evaluated these combinations, and readers should discuss any combination protocols with their healthcare provider.
What reconstitution solution should be used?
Sources differ on this point. The compound's published patent and clinical trials used Phosphate Buffered Saline (PBS). Some community members report that standard bacteriostatic water may cause solubility issues, while isotonic solutions (bacteriostatic water with sodium chloride) appear to work better. This is a practical consideration worth discussing with a healthcare provider or pharmacist.
Sources & References
Clinical Trials and Human Studies
[1] Brines M. "Discovery of a Master Regulator of Injury and Healing: Tapping the Innate Repair Receptor." Molecular Medicine. 2014. PMC4374522
[2] Brines M, Cerami A. "The Receptor That Tames the Innate Immune Response." Molecular Medicine. 2012. (Discovery and development of the innate repair receptor and its non-erythropoietic ligands)
[3] Dahan A, et al. "Targeting the innate repair receptor to treat neuropathy." Pain Reports. 2017. PMC5741312
[4] Culver DA, et al. "Cibinetide Improves Corneal Nerve Fiber Abundance in Patients With Sarcoidosis-Associated Small Nerve Fiber Loss and Neuropathic Pain." Investigative Ophthalmology & Visual Science. 2017;58(6):BIO52-BIO60. doi: 10.1167/iovs.16-21291
[5] ClinicalTrials.gov. NCT02039687. "Phase 2 study of ARA 290 on corneal nerve fiber density in sarcoidosis (1 mg vs 4 mg vs 8 mg daily SC for 28 days)."
[6] IUPHAR/BPS Guide to Pharmacology. Cibinetide (ARA-290) ligand profile: structure, receptor binding, and pharmacology.
Preclinical Studies
[7] Nairz M, et al. "Cibinetide dampens innate immune cell functions thus ameliorating the course of experimental colitis." Scientific Reports. 2017;7:13012. doi: 10.1038/s41598-017-13046-3
[8] Peng B, Kong G, Yang C, Ming Y. "Erythropoietin and its derivatives: from tissue protection to immune regulation." Cell Death & Disease. 2020;11(2):79. doi: 10.1038/s41419-020-2276-8
[9] Zhang W, Yu G, Zhang M. "ARA 290 relieves pathophysiological pain by targeting TRPV1 channel: Integration between immune system and nociception." Peptides. 2016.
[10] Watanabe M, et al. "A Nonhematopoietic Erythropoietin Analogue, ARA 290, Inhibits Macrophage Activation and Prevents Damage to Transplanted Islets." Transplantation. 2016;100(3):554-562. doi: 10.1097/TP.0000000000001026
[11] Brines M, et al. "ARA 290, a Nonerythropoietic Peptide Engineered from Erythropoietin, Improves Metabolic Control and Neuropathic Symptoms in Patients with Type 2 Diabetes." Molecular Medicine. 2015. PMC4365069
[12] Heij L, et al. "Safety and efficacy of ARA 290 in sarcoidosis patients with symptoms of small fiber neuropathy: a randomized, double-blind pilot study." Molecular Medicine. 2012. PMC3563705
[13] Brines M, et al. "ARA 290 improves metabolic control and neuropathic symptoms in patients with type 2 diabetes." Molecular Medicine. 2015. PMC4365069
[14] Yan L, et al. "EPO Derivative ARA290 Attenuates Early Renal Allograft Injury in Rats by Targeting NF-κB Pathway." Transplantation Proceedings. 2018;50(5):1575-1582. doi: 10.1016/j.transproceed.2018.03.015
[15] CNS Neuroscience & Therapeutics. "ARA290 brain tissue protection in cerebral ischemic stroke." 2024.
[16] Hache G, et al. "ARA290, a Specific Agonist of Erythropoietin/CD131 Heteroreceptor, Improves Circulating Endothelial Progenitors' Angiogenic Potential and Homing Ability." Shock. 2016;46(4):390-397. doi: 10.1097/SHK.0000000000000606
[17] O'Leary OE, et al. "The vasoreparative potential of endothelial colony-forming cells in the ischemic retina is enhanced by cibinetide, a non-hematopoietic erythropoietin mimetic." Experimental Eye Research. 2019;182:144-155. doi: 10.1016/j.exer.2019.03.001
[18] Huang B, et al. "Non-erythropoietic erythropoietin-derived peptide protects mice from systemic lupus erythematosus." Journal of Cellular and Molecular Medicine. 2018;22(7):3330-3339. doi: 10.1111/jcmm.13608
Additional References
[19] Bitto A, et al. "Activation of the EPOR-β common receptor complex by cibinetide ameliorates impaired wound healing in mice with genetic diabetes." Biochimica et Biophysica Acta. 2018;1864(2):632-639. doi: 10.1016/j.bbadis.2017.12.006
[20] Al-Onaizi MA, et al. "Early monocyte modulation by the non-erythropoietic peptide ARA 290 decelerates AD-like pathology progression." 2022.
[21] Mohtavinejad N, et al. "Synthesis and evaluation of (99m)Tc-DOTA-ARA-290 as potential SPECT tracer for targeting cardiac ischemic region." 2021.
[22] PMC3567997. "ARA290 attenuates renal ischemia/reperfusion injury." 2013.
[23] Hosseini-Zare MS, et al. "Peripheral neuropathy response to erythropoietin in type 2 diabetic patients with mild to moderate renal failure." Clinical Neurology and Neurosurgery. 2012;114(6):663-667. doi: 10.1016/j.clineuro.2012.01.007
Related Peptide Guides
- BPC-157 — Core tissue repair peptide; addresses structural healing where ARA-290 addresses neural repair
- TB-500 — Cellular mobility and systemic healing support; complementary to ARA-290 for comprehensive recovery
- GHK-Cu — Connective tissue and collagen quality; reported by some community members in combination with ARA-290 for nerve pain
- KPV — Anti-inflammatory tripeptide for gut and immune modulation; complementary anti-inflammatory pathway
- SS-31 — Mitochondrial membrane stabilization; useful when healing stalls due to mitochondrial dysfunction
- MOTS-C — Mitochondrial-derived peptide for metabolic health; supports cellular energy during nerve repair
- NAD+ — Cellular energy and repair cofactor; supports metabolic foundation for nerve regeneration
- Tesamorelin — GH-axis support; compatible with ARA-290 and often layered for recovery protocols
- Sermorelin — Growth hormone releasing hormone analog; compatible for broader anti-aging stacks
- VIP — Vasoactive intestinal peptide; relevant for disc/spinal degeneration where ARA-290 addresses nerve pain component
- Semaglutide — GLP-1 agonist; relevant given ARA-290's metabolic benefits in diabetes and reports of GLP-1-induced neuropathy requiring ARA-290
Need the reconstitution math for ARA-290 (Cibinetide): Complete Peptide Guide?
Open the calculator with ARA-290 (Cibinetide): Complete Peptide Guide prefilled to estimate concentration, draw volume, and related measurement math from the reconstitution details you already have.