Bronchogen: Complete Research Guide
On this page
Quick Reference Card
Attribute
Also Known As
- Detail
- AEDL, Ala-Glu-Asp-Leu peptide, Khavinson tetrapeptide, Respiratory bioregulator
Attribute
Administration
- Detail
- Injectable (subcutaneous), Oral (capsule form available in some markets)
Attribute
Research Status
- Detail
- Research Compound — No FDA Approval. Preclinical data only (rat models, cell cultures).
Attribute
Typical Dose Range
- Detail
- 0.5–5 mg/day subcutaneous; 1–2 mg/day most commonly cited
Attribute
Half-Life
- Detail
- Not established (no formal pharmacokinetic studies published)
Attribute
Cycle Length
- Detail
- 10–40 days, repeated every 3–6 months
Attribute
Storage
- Detail
- Lyophilized: -20°C (up to 36 months); Reconstituted: 2–8°C (use within 28 days)
Overview / What Is Bronchogen?
The Basics
Bronchogen is a lung-specific peptide bioregulator made up of just four amino acids. It belongs to a class of short peptides developed through decades of Russian bioregulation research, specifically designed to support and restore the cells lining your airways.
Think of your bronchial tubes as highways where air travels in and out of your lungs. The lining of these tubes takes constant punishment from everything you breathe, including pollution, allergens, smoke, and pathogens. Over time, or after illness, this lining can become damaged and inflamed. Bronchogen was designed to help those cells repair and regenerate.
Unlike bronchodilators or inhalers that provide immediate symptom relief by opening airways, Bronchogen works at the cellular level over a period of weeks. It targets the root of respiratory decline rather than masking symptoms. People who explore Bronchogen are typically dealing with the aftermath of smoking, chronic respiratory conditions, environmental pollution exposure, or age-related decline in lung function.
The peptide was developed by Vladimir Khavinson and colleagues at the Saint Petersburg Institute of Bioregulation and Gerontology, as part of a broader research program that produced organ-specific bioregulators for different tissues throughout the body.
The Science
Bronchogen (Ala-Glu-Asp-Leu, or AEDL) is a synthetic tetrapeptide classified as a bioregulatory peptide with tissue-specific effects in bronchial and pulmonary tissue. It was originally derived from murine bronchial mucosa and synthesized as part of Khavinson's peptide bioregulator research program at the Institute of Bioregulation and Gerontology, Saint Petersburg, Russia [1][2].
The peptide acts through multiple molecular mechanisms, including direct DNA binding and stabilization, chromatin remodeling via histone interactions, and tissue-specific gene expression modulation. Research demonstrates preferential accumulation and biological activity in lung tissue, with relatively few off-target effects in other organ systems [2][3].
In preclinical models, Bronchogen has shown the ability to restore bronchial epithelial structure in rats with nitrogen dioxide-induced chronic obstructive pulmonary disease (COPD), reduce pro-inflammatory cytokine levels, increase surfactant production, and normalize mucociliary function [4][5]. All published evidence comes from animal models and in vitro studies. No human clinical trials have been conducted or registered as of early 2026.
Molecular Identity
Attribute
Common Names
- Detail
- Bronchogen, AEDL, Ala-Glu-Asp-Leu peptide
Attribute
Amino Acid Sequence
- Detail
- Ala-Glu-Asp-Leu (AEDL)
Attribute
Full Condensed Form
- Detail
- H-Ala-Glu-Asp-Leu-OH
Attribute
Molecular Formula
- Detail
- C₁₈H₃₀N₄O₉
Attribute
Molecular Weight
- Detail
- 446.45 g/mol
Attribute
CAS Number
- Detail
- Not assigned
Attribute
Structural Type
- Detail
- Linear tetrapeptide
Attribute
Source
- Detail
- Fully synthetic (solid-phase peptide synthesis)
Attribute
Net Charge at Physiological pH
- Detail
- -2 (two acidic residues: Glu, Asp)
Attribute
Appearance
- Detail
- White crystalline lyophilized powder
Attribute
DNA Interaction
- Detail
- Binds DNA at guanine-N7 within the major groove; non-intercalating
Attribute
Functional Class
- Detail
- Bioregulator peptide; DNA-binding regulatory peptide; geroprotective agent
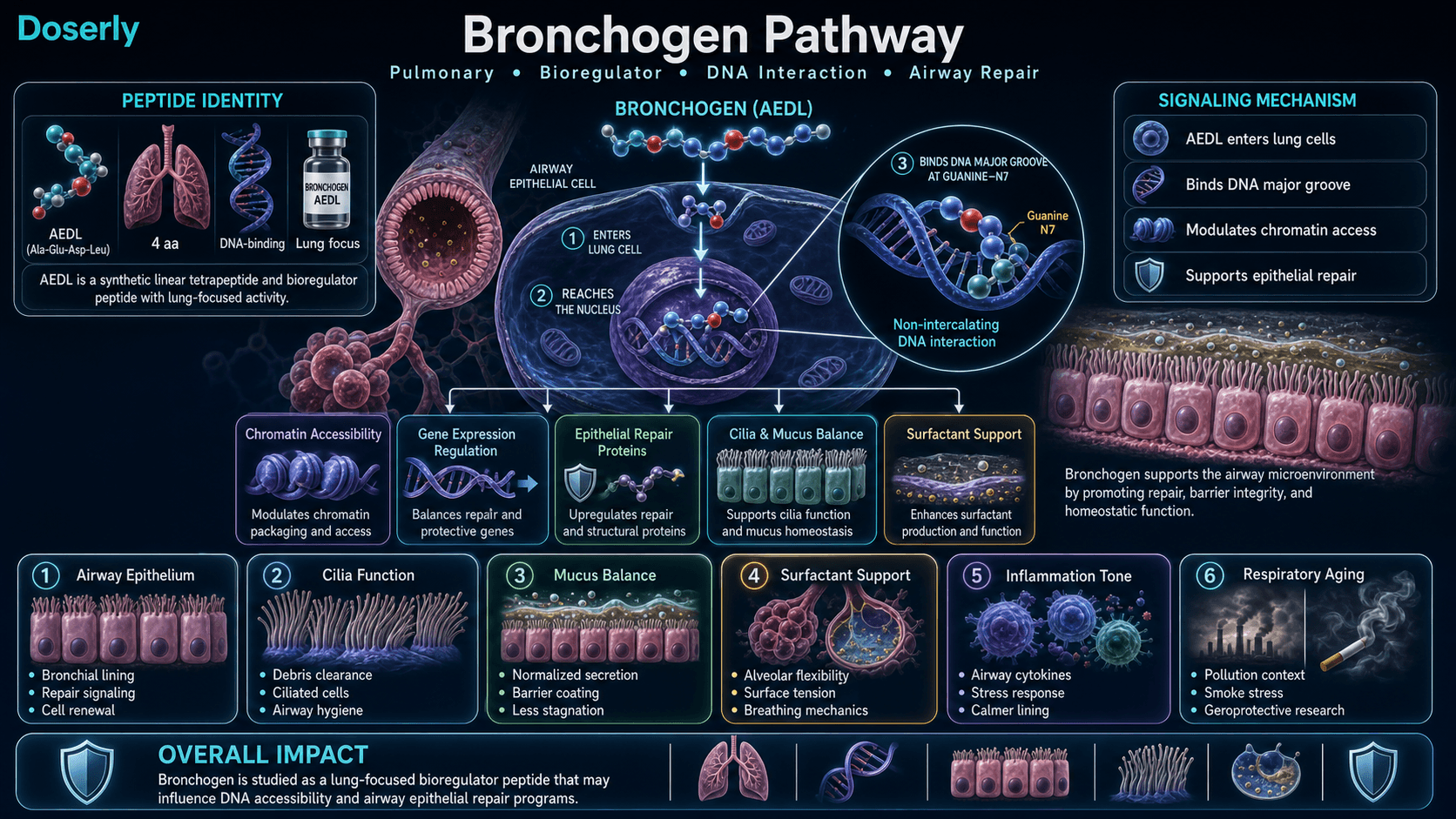
Mechanism of Action
The Basics
Bronchogen works by entering your lung cells and interacting directly with their genetic machinery. It is small enough (only four amino acids) to pass through cell membranes and reach the nucleus, where your DNA is stored.
Once inside, Bronchogen acts like a stabilizer for your DNA. Imagine your DNA as a set of instructions that your cells need to read in order to build and repair themselves. Over time, especially with exposure to pollution, smoke, or simply aging, those instructions can become damaged or harder to read. Bronchogen helps keep those instructions stable and accessible, making it easier for your lung cells to carry out their repair work.
Beyond DNA stabilization, Bronchogen also influences how tightly your genetic material is packed. In older or damaged cells, the DNA tends to become more tightly wound, making certain repair instructions inaccessible. Bronchogen loosens this packaging, allowing your cells to access genes they need for repair and regeneration. This effect appears to be more pronounced in older cells, which is consistent with the peptide's geroprotective profile.
The overall result is a cascade of beneficial effects: your airway lining rebuilds itself more effectively, inflammation settles down, and your lungs produce more of the protective surfactant coating that keeps air sacs flexible.
The Science
Bronchogen operates through three interconnected molecular mechanisms:
1. DNA Stabilization
Differential scanning microcalorimetry studies demonstrate that Bronchogen increases DNA melting temperature (Tm) by approximately 3.1°C within a specific concentration range (r = 0.01–0.055, molar ratio of peptide to DNA base pairs) [6]. The peptide binds within the major groove at guanine-N7 positions, with preferential affinity for CTG motifs. This stabilization reduces DNA damage accumulation, decreases cell turnover rates, and consequently reduces telomerase activation, which is associated with both cancer risk and accelerated aging [2][7].
2. Chromatin Remodeling
Fluorescence experiments demonstrate Bronchogen binding to linker histone H1 and core histone H3 at specific lysine residues [8]. These interactions shift condensed heterochromatin toward euchromatin states, increasing transcriptional accessibility. Plant cell studies showed heterochromatin reduction from 45% to 25% following treatment [8]. This epigenetic modification enables re-expression of silenced genes in aged cells without altering the underlying DNA sequence.
3. Tissue-Specific Gene Expression
In bronchial epithelial cell cultures, Bronchogen upregulates several key lung-specific genes [9][10]:
- NKX2-1: Master regulator of lung epithelial cell fate
- FOXA1 and FOXA2: Maintain cellular identity in respiratory epithelium (1.5–15x baseline, with stronger effects in older cells)
- MUC4 and MUC5AC: Gel-forming mucins essential for airway barrier function
- SFTPA1: Surfactant protein A, involved in alveolar surface tension reduction and innate immune defense
- Ki67 and Mcl-1: Cell proliferation and anti-apoptotic markers
Comparative research confirms tissue specificity: Bronchogen activates lung cell genes exclusively, while related peptides with different sequences activate pancreatic or other organ-specific differentiation markers [10].
Pathway Visualization Image
Pharmacokinetics
The Basics
Formal pharmacokinetic data for Bronchogen is not available in the published literature. There are no studies measuring how quickly the peptide is absorbed, how long it stays in your system, or how it is eliminated from your body.
What is known is that Bronchogen is a very small molecule (446 daltons), which allows it to pass through cell membranes and reach the nucleus. Its small size likely means rapid absorption and clearance, similar to other ultra-short peptides in the bioregulator class.
The peptide is most commonly administered subcutaneously, though oral bioregulator capsules are available in some markets (particularly from Russian manufacturers). The absorption and bioavailability differences between these routes have not been formally compared in published research.
The Science
No formal pharmacokinetic parameters (Cmax, Tmax, AUC, clearance, volume of distribution, bioavailability) have been published for Bronchogen. This represents a significant gap in the available evidence base.
Based on properties of analogous ultra-short peptides in the bioregulator family, the following can be inferred but not confirmed:
- Molecular weight (446.45 Da): Well below the threshold for passive membrane permeation, suggesting efficient cellular uptake [8]
- Peptide transporter uptake: Ultra-short peptides are taken up via peptide transporters (e.g., PEPT1/2, LAT family) and can reach intracellular compartments including the nucleus [11]
- Oral stability signal: Related tetrapeptides (e.g., Livagen/KEDA) show resistance to intestinal peptidase hydrolysis in rat models, suggesting potential oral bioavailability for this peptide class [11]
- Tissue distribution: Khavinson's research indicates tissue-specific accumulation in bronchial and lung tissue, consistent with the peptide's observed organ selectivity [2]
The absence of formal PK data means that dosing protocols are based on empirical clinical observation from Russian practitioners rather than pharmacokinetically optimized regimens.
Research & Clinical Evidence
Bronchogen and Chronic Obstructive Pulmonary Disease (COPD)
The Basics
The strongest evidence for Bronchogen comes from rat studies modeling COPD. Researchers exposed rats to nitrogen dioxide gas for 60 days to create lung damage similar to chronic obstructive conditions, then treated them with Bronchogen for one month.
The results showed that Bronchogen reversed many of the hallmarks of COPD. The damaged airway lining healed, with ciliated cells (the tiny hair-like structures that sweep debris out of your airways) being restored. Abnormal cell changes, including goblet cell overgrowth (too many mucus-producing cells) and squamous metaplasia (cells changing to the wrong type), were corrected. Inflammation markers in the airways decreased, and the lungs began producing more of the protective substances they need, including secretory IgA (for fighting infections) and surfactant protein B (for keeping air sacs from collapsing).
Importantly, these improvements persisted after treatment stopped, suggesting genuine tissue repair rather than temporary symptom suppression.
The Science
Two key animal studies form the core evidence base:
Kuzubova et al. (2015) demonstrated that one-month Bronchogen administration in rats with NO₂-induced COPD eliminated bronchial epithelial remodeling symptoms: goblet cell hyperplasia, squamous metaplasia, lymphocytic infiltration, and emphysema were all reversed [4]. Ciliated cell populations were restored, and functional markers normalized. Bronchoalveolar lavage analysis showed increased secretory IgA production and normalization of the inflammatory cytokine profile [4].
Titova et al. (2017) expanded these findings, demonstrating decreased neutrophilic inflammation, normalization of cellular composition and pro-inflammatory cytokine/enzyme profiles in bronchoalveolar fluid, restoration of bronchial epithelial structure, and increased levels of both secretory IgA (local immunity marker) and surfactant protein B (lung compliance marker) [5].
Both studies used the same COPD model (60-day intermittent NO₂ exposure in Wistar rats) and confirmed consistent results across the Bronchogen intervention.
Bronchogen and DNA Stabilization
The Basics
Laboratory studies show that Bronchogen physically stabilizes DNA, making it more resistant to heat damage. While this might sound like a niche laboratory finding, it has broader implications. More stable DNA means less damage accumulates over time, which translates to healthier cells that maintain their function longer as they age. For lung cells that are constantly exposed to environmental stressors, this stabilizing effect could help maintain their repair capacity over decades.
The Science
Monaselidze et al. (2011) used differential scanning microcalorimetry to demonstrate that Bronchogen increases DNA melting temperature by 3.1°C from calf thymus and mouse liver DNA within a narrow concentration range (r = 0.01–0.055) [6]. This stabilization effect plateaued beyond this range, suggesting a saturable binding mechanism consistent with specific DNA interaction rather than nonspecific coating.
Bronchogen and Gene Expression in Aging Cells
The Basics
One of the most interesting findings is that Bronchogen appears to have a stronger effect on older cells than younger ones. In laboratory cell cultures, the peptide's ability to activate repair genes became more pronounced as the cells aged. This age-dependent effect aligns with the concept that the peptide works by reopening genetic instructions that have become locked away as cells get older.
The Science
Khavinson et al. (2014) demonstrated that Bronchogen regulates gene expression and protein synthesis in bronchial epithelium, with expression increases ranging from 1.5 to 15 times baseline depending on the gene and cell passage number [9]. FOXA genes showed particularly strong activation in later-passage cultures, indicating enhanced responsiveness in senescent cellular environments. This age-dependent effect is consistent with the chromatin remodeling mechanism, where aged cells have more condensed heterochromatin available for peptide-mediated de-condensation [8].
Biomarker Evidence Matrix
The following matrix summarizes the available evidence and community-reported effectiveness for Bronchogen across relevant health categories.
Category
Recovery & Healing
- Evidence Strength
- 5/10
- Reported Effectiveness
- 6/10
- Summary
- Animal studies demonstrate epithelial restoration in COPD models. Community reports describe improved breathing and airway clearing, though sample size is very small.
Category
Inflammation
- Evidence Strength
- 5/10
- Reported Effectiveness
- 6/10
- Summary
- Rat models show reduced pro-inflammatory cytokines (TNF-alpha, IL-6) and normalized immune cell composition. Community users report reduced airway inflammation.
Category
Immune Function
- Evidence Strength
- 4/10
- Reported Effectiveness
- N/A
- Summary
- Animal studies show increased secretory IgA production, suggesting enhanced mucosal immunity. No community data available.
Category
Longevity & Neuroprotection
- Evidence Strength
- 3/10
- Reported Effectiveness
- 4/10
- Summary
- DNA stabilization and geroprotective properties observed in vitro. Community interest is theoretical rather than experiential.
Category
Side Effect Burden
- Evidence Strength
- 4/10
- Reported Effectiveness
- 8/10
- Summary
- No adverse effects documented in preclinical research. Community reports consistently describe high tolerability with minimal side effects.
Category
Treatment Adherence
- Evidence Strength
- N/A
- Reported Effectiveness
- 7/10
- Summary
- No research data. Community reports indicate straightforward protocols with good adherence.
Category
Physical Performance
- Evidence Strength
- 2/10
- Reported Effectiveness
- 5/10
- Summary
- Indirect evidence only: improved respiratory function could enhance exercise capacity. Limited community reports of improved cardio tolerance.
Category
Energy Levels
- Evidence Strength
- 2/10
- Reported Effectiveness
- 4/10
- Summary
- No direct research. Theoretical improvement through better oxygenation. Insufficient community data.
Categories not scored (insufficient data): Fat Loss, Muscle Growth, Weight Management, Appetite & Satiety, Food Noise, Sleep Quality, Focus & Mental Clarity, Memory & Cognition, Mood & Wellbeing, Anxiety, Stress Tolerance, Motivation & Drive, Emotional Aliveness, Emotional Regulation, Libido, Sexual Function, Joint Health, Pain Management, Gut Health, Digestive Comfort, Nausea & GI Tolerance, Skin Health, Hair Health, Heart Health, Blood Pressure, Heart Rate & Palpitations, Hormonal Symptoms, Temperature Regulation, Fluid Retention, Body Image, Bone Health, Cravings & Impulse Control, Social Connection, Withdrawal Symptoms, Daily Functioning
Benefits & Potential Effects
The Basics
Bronchogen's benefits center squarely on respiratory health. It is not a broad-spectrum peptide that promises improvements across dozens of body systems. Instead, it targets the lungs specifically, which is both its strength and its limitation.
The primary potential benefit is restoration of damaged airway tissue. For people whose bronchial lining has been compromised by years of smoking, pollution exposure, chronic bronchitis, or simply aging, Bronchogen may help those cells rebuild themselves from the ground up. This includes restoring the ciliated cells that sweep debris out of your airways, normalizing mucus production (not too much, not too little), and increasing surfactant production to keep your air sacs flexible.
The anti-inflammatory effect is the second major benefit. Chronic low-grade inflammation in the airways is both a cause and consequence of respiratory decline. By reducing inflammatory signaling molecules, Bronchogen may help break the cycle of inflammation and tissue damage.
A third potential benefit is DNA stabilization and geroprotective effects. By keeping lung cell DNA healthy for longer, Bronchogen may slow the age-related decline in respiratory capacity that affects everyone, becoming more relevant as you enter your 50s and beyond.
The Science
Based on preclinical evidence, the following benefits have been documented:
- Bronchial Epithelial Restoration: Structural normalization of airway epithelium in COPD models, including restoration of ciliated cells, prevention of goblet cell hyperplasia, and reversal of squamous metaplasia [4][5]
- Anti-inflammatory Effects: Reduced neutrophilic inflammation with normalization of pro-inflammatory cytokine profiles (TNF-alpha, IL-6, IL-8) in bronchoalveolar lavage fluid [4][5]
- Enhanced Mucosal Immunity: Increased secretory IgA production, strengthening local immune defense against inhaled pathogens [4][5]
- Surfactant Restoration: Increased surfactant protein B levels, improving alveolar compliance and gas exchange efficiency [5]
- DNA Stabilization: Enhanced DNA thermostability suggesting reduced DNA damage accumulation and decreased need for telomerase activation [6]
- Gene Expression Normalization: Upregulation of lung-specific differentiation markers (NKX2-1, FOXA1/2) and mucin/surfactant genes, with enhanced effects in aged cellular environments [9][10]
All documented benefits derive from animal and in vitro models. Human clinical validation remains absent.
Reading about potential benefits is the starting point. Knowing whether you're actually experiencing them is where real value begins. Doserly lets you track the specific health markers that matter for your protocol, from body composition and energy levels to sleep quality, mood, and recovery time, building a personal dataset that goes beyond subjective impressions.
The app's proactive monitoring doesn't wait for you to notice a problem. It surfaces patterns in your logged data that might suggest suboptimal timing, flags potential interactions with other items in your health stack, and helps you identify which benefits are tracking with what the research suggests and which aren't materializing. Think of it as a second set of eyes on your protocol, always watching the trends.
Capture changes while they are still fresh.
Log symptoms, energy, sleep, mood, and other observations alongside protocol events so patterns do not live only in memory.
Trend view
Symptom timeline

Symptom tracking is informational and should be interpreted with a qualified clinician.
Side Effects & Safety Considerations
The Basics
Bronchogen has a favorable safety profile based on what is available in the published literature. In animal studies, no significant adverse effects have been reported. Community users consistently describe high tolerability, with the most commonly noted reaction being brief, mild flushing and a temporary increase in heart rate lasting a few minutes after injection.
One user reported transient flushing and elevated heart rate (approximately 106 bpm) lasting about three minutes before returning to baseline. No other adverse effects were reported across multiple community accounts spanning different dosing protocols and durations.
It is important to note, however, that the safety data is limited. No formal toxicology studies, no dose-escalation studies, and no human clinical trials have been published. The absence of reported side effects is not the same as evidence of safety, particularly at higher doses or with longer-term use. Anyone considering Bronchogen should consult with a healthcare professional, especially those with existing respiratory conditions, autoimmune disorders, or who are taking immunomodulatory medications.
The Science
Published preclinical studies report no significant adverse effects associated with Bronchogen administration in rat models [4][5]. The peptide's tissue specificity (preferential accumulation in bronchial/lung tissue with minimal off-target effects) is posited as a contributing factor to its tolerability profile [2].
One community report noted transient autonomic responses (flushing, heart rate increase to 106 bpm for approximately 3 minutes post-injection) at 500 mcg subcutaneous dosing, resolving spontaneously. This pattern is consistent with vasoactive peptide responses and has not been associated with adverse outcomes.
Theoretical safety considerations include:
- Immunomodulatory effects: Increased secretory IgA and altered cytokine profiles could theoretically interact with immunosuppressive medications or autoimmune conditions
- Cell proliferation: Upregulation of Ki67 (proliferation marker) warrants theoretical caution in individuals with active or history of malignancy, particularly lung cancer
- Limited long-term data: No studies examine repeated cycling over periods longer than one month
Dosing Protocols
The Basics
Bronchogen dosing protocols are not standardized and have not been established through formal clinical trials. What follows is a summary of the ranges most commonly discussed in research literature and community reports.
Most sources describe a daily subcutaneous injection, with doses typically falling between 0.5 mg and 5 mg per day. The range of 1 to 2 mg daily appears most frequently across both research-oriented and community sources. Some protocols include a loading phase at the lower end (0.5 mg/day for the first week) before moving to a maintenance dose of 2 mg/day.
Cycle length varies more significantly. Some protocols call for short courses of 10 to 20 days, while others extend to 30 or 40 days. The 10 to 20 day range is more common in the published literature, while 30 to 40 day cycles appear more frequently in community protocols. Most sources agree that cycles should be repeated every 3 to 6 months, reflecting the bioregulator philosophy that these short peptides "reset" cellular function and the effects persist between courses.
Administration is typically once daily, subcutaneously. One community source recommends a 6 days on, 1 day off schedule. Timing relative to meals varies: one source suggests at least 2 hours after the last meal (administered at bedtime), while others recommend morning administration during peak respiratory activity.
As with all research compounds, anyone considering Bronchogen should discuss dosing with a qualified healthcare professional who can account for individual health factors.
The Science
No formal dose-response studies have been published for Bronchogen. Preclinical animal studies used the peptide at concentrations consistent with Khavinson's broader bioregulator dosing framework, but specific mg/kg dosing in animal models has not been standardized in the available English-language literature [4][5].
The dosing protocols in circulation are derived from clinical observation within the Russian bioregulator tradition rather than pharmacokinetically optimized regimens. The absence of human PK data (Cmax, AUC, bioavailability) means that optimal dosing remains empirically determined.
Consistency is the difference between a protocol that delivers results and one that wastes time and money. Doserly was built for exactly this: keeping you on track with the precision your protocol demands.
The built-in calculators handle the math you shouldn't be doing in your head. The reconstitution calculator tells you exactly how much bacteriostatic water to add for your target concentration. The dose calculator converts between units, milligrams, and syringe markings so you draw the right amount every time. The injection site heat map tracks where you've administered and when, helping you rotate sites systematically to reduce tissue damage, scarring, and absorption inconsistencies from overusing the same area. Pair that with smart reminders tuned to your protocol's timing requirements, and you build the kind of daily consistency that separates optimized protocols from haphazard ones.
Track injection timing, draw notes, and site rotation.
Doserly helps keep syringe-related notes, injection site history, reminders, and reconstitution context together for easier review.
Injection log
Site rotation
Injection logs support record-keeping; follow clinician instructions for administration.
What to Expect
Bronchogen is a bioregulator peptide, and bioregulators work differently from most other peptides. Rather than producing immediate, noticeable effects, they work gradually at the cellular level, and their benefits tend to accumulate over weeks and persist for months after a course ends.
Days 1–7:
Most users report no noticeable changes during the first week. Some may experience brief flushing or a mild increase in heart rate immediately after injection, lasting only a few minutes. One user described this as an immediate airway clearing sensation, though this is not universally reported. This is typically the loading phase if a titrated protocol is being followed.
Days 8–20:
Subtle improvements in breathing may begin to emerge. Users with pre-existing respiratory complaints have reported easier breathing during exercise, reduced phlegm production, and less wheezing. These changes tend to be gradual rather than dramatic. Some users report no perceptible changes during the active course, with improvements becoming apparent only weeks after completion.
Days 21–40 (extended protocols):
For those following longer protocols, the trend of gradual respiratory improvement may continue. One user tracking spirometry data noted measurable improvements in FEV1 (forced expiratory volume) and PEF (peak expiratory flow) over this period, though this is a single data point.
Post-course (weeks to months):
Consistent with the bioregulator model, benefits are expected to persist and potentially continue developing after the course ends. One community member reported that improvements were "more gradual" after stopping but continued to progress, suggesting ongoing cellular repair triggered during the active course. Most protocols recommend repeating the cycle every 3 to 6 months for maintenance.
Important caveats: Individual responses vary significantly. Some users report minimal perceptible changes despite completing full courses. Bronchogen is designed for long-term tissue restoration, not acute symptom relief. Users stacking Bronchogen with other peptides (BPC-157, TB-500, Chonluten) may find it difficult to attribute improvements specifically to Bronchogen.
Interaction Compatibility
Good With (Synergistic Compounds)
- Chonluten (not in registry, see note) — Another respiratory bioregulator (tripeptide EDG). Multiple community sources recommend pairing Bronchogen with Chonluten for comprehensive respiratory support, as they target complementary pathways in lung tissue.
- Epithalon — Systemic geroprotective tetrapeptide from the same Khavinson bioregulator family. Often used alongside organ-specific bioregulators for comprehensive anti-aging protocols.
- BPC-157 — Broad-spectrum healing peptide. Community members have stacked with Bronchogen, though no formal interaction data exists.
- TB-500 — Tissue repair peptide. Some community members use alongside Bronchogen for combined healing protocols.
- Thymosin Alpha-1 — Immune modulator. Suggested as a complement for comprehensive respiratory and immune support protocols.
- GHK-Cu — Copper peptide with tissue remodeling properties. One community member noted potential for COPD-related lung tissue support.
- VIP — Vasoactive intestinal peptide. One community source recommended VIP alongside Bronchogen for lung health.
- Pinealon — Neurological bioregulator from the same Khavinson family. Often combined in multi-organ bioregulator protocols.
- Cardiogen — Cardiovascular bioregulator. Commonly paired in multi-organ support protocols.
Note: Chonluten does not currently have a page in the Doserly peptide registry.
Not Good With (Potential Concerns)
No formal interaction contraindications have been established for Bronchogen. The following are theoretical considerations:
- Immunosuppressive medications: Bronchogen's immunomodulatory effects (increased secretory IgA, altered cytokine profile) could theoretically interfere with immunosuppressive therapy. Consult a healthcare provider before combining.
- Other bioregulator peptides targeting the same tissue: Using multiple lung-targeting bioregulators simultaneously may produce unpredictable additive effects. Some practitioners recommend sequential rather than simultaneous use.
Administration Guide
Bronchogen is most commonly administered as a subcutaneous injection. Oral capsule formulations exist (primarily from Russian manufacturers), though subcutaneous injection is the predominant route discussed in research and community settings.
Materials typically used:
- Insulin syringes (U-100, 29-31 gauge)
- Alcohol swabs (70% isopropanol)
- Bacteriostatic water for reconstitution
- Sharps disposal container
Reconstitution:
A common reconstitution approach uses 2.0 mL of bacteriostatic water per 10 mg vial, yielding a concentration of 5.0 mg/mL. Some practitioners prefer 3.0 mL per 20 mg vial (approximately 6.67 mg/mL). Use the reconstitution calculator for precise volume calculations based on your specific vial size and target dose.
Timing considerations:
Timing recommendations vary across sources. One protocol suggests administration at bedtime, at least 2 hours after the last meal. Another suggests morning administration, reasoning that bioregulators are most effective when the target organ is in its peak active state (lungs are working hardest during daytime activity). Both approaches are reported in the community, and no comparative data exists to determine which is superior.
Post-administration observations:
Some users report brief flushing and a temporary increase in heart rate (resolving within minutes). This appears to be a common, benign response. Monitor for any unusual reactions, particularly during the first few administrations.
Consistent administration is where protocols succeed or fail. Doserly helps you build and maintain your daily routine: reminders tuned to your compound's optimal timing, a log for every administration with dose, time, and any immediate observations, and the ability to track post-administration reactions so you build a clear picture of how each session goes.
Over time, this daily logging reveals patterns. You might notice that morning administration produces fewer injection site reactions than evening. Or that timing relative to meals, as discussed above, correlates with better tolerance. These are the kind of practical insights that emerge from consistent tracking and turn a generic protocol into one that's optimized for your body and schedule.
Build reminders around the routine, not just the compound.
Doserly can keep timing, skipped doses, and schedule changes organized so the plan you read about becomes easier to follow and review.
Today view
Upcoming reminders

Reminder tracking supports consistency; it does not select a protocol for you.
Supplies & Planning
The following materials are generally associated with Bronchogen protocols:
Peptide:
- Bronchogen is commonly available in 10 mg or 20 mg lyophilized vials from research peptide suppliers
Reconstitution and Injection Supplies:
- Bacteriostatic water (BAC water with 0.9% benzyl alcohol)
- U-100 insulin syringes (29-31 gauge, 1/2" needle)
- Alcohol swabs (70% isopropanol)
- Sharps disposal container
Storage:
- Refrigerator space for reconstituted vials (2-8°C)
- Freezer space for unreconstituted vials (-20°C for long-term storage)
The specific quantities needed depend on individual dosing protocols and cycle duration. Consult with a healthcare provider for guidance on appropriate quantities, and use the reconstitution calculator for preparation math.
Storage & Handling
Lyophilized (powder) form:
- Store at -20°C (-4°F) or below for long-term storage (up to 36 months reported)
- Short-term storage at 2-8°C (35.6-46.4°F) is acceptable for weeks to months
- Keep in original sealed packaging with desiccant
- Protect from light and moisture
- Allow vials to reach room temperature before opening to prevent condensation
Reconstituted (liquid) form:
- Refrigerate immediately at 2-8°C (35.6-46.4°F)
- Use within 28 days when reconstituted with bacteriostatic water
- Do not freeze reconstituted solutions
- Avoid repeated freeze-thaw cycles
- Inspect for clarity before each use; discard if cloudy, discolored, or if particles are visible
Handling best practices:
- Use sterile technique when reconstituting and drawing doses
- Swab vial stopper with alcohol before each draw
- Label reconstituted vials with date and concentration
- Use a fresh needle for each injection
Lifestyle Factors
Several lifestyle factors may complement or undermine Bronchogen's respiratory-focused effects:
Air quality: Avoiding exposure to environmental pollutants, cigarette smoke, and aerosolized toxins is critical. Continuing to expose airways to irritants while using a lung-repair peptide works against the purpose of the protocol. For those using Bronchogen as part of post-smoking recovery, complete cessation of smoking or vaping is essential for meaningful benefit.
Physical activity: Regular aerobic exercise (brisk walking, swimming, cycling) supports pulmonary gas exchange and helps maintain lung capacity. Exercise also promotes circulation, which supports the delivery of nutrients and repair signals to lung tissue. Start gradually if respiratory function is currently compromised.
Nutrition: A diet rich in fat-soluble vitamins, particularly vitamins A, D, and E, supports mucosal health and immune function within the lungs. Antioxidant-rich foods (fruits, vegetables, particularly those high in vitamins C and E) may complement Bronchogen's antioxidant effects. Adequate protein intake supports the tissue repair processes that Bronchogen stimulates at the genetic level.
Hydration: Maintaining adequate hydration supports mucociliary clearance, the mechanism by which your airways sweep out debris and pathogens. Dehydration thickens mucus and impairs this process.
Sleep: Ensuring 7 to 9 hours of quality sleep facilitates natural tissue repair processes and maintains immune function. Respiratory tissue repair, like most regenerative processes, is enhanced during sleep.
Regulatory Status & Research Classification
United States (FDA):
Bronchogen is not approved by the FDA for any therapeutic indication. It is classified as a research chemical. No Investigational New Drug (IND) applications or clinical trials are registered on ClinicalTrials.gov as of early 2026. It is available from research peptide suppliers for in vitro and laboratory use only.
Russia:
Bronchogen was developed within the Russian bioregulator research tradition and has been available as a dietary supplement (biologically active additive, or BAA) and as part of clinical protocols at longevity and gerontology clinics, particularly those associated with the Institute of Bioregulation and Gerontology in Saint Petersburg. Six peptide-based pharmaceuticals and 64 peptide food supplements were introduced into Russian clinical practice by Khavinson.
European Union (EMA):
No marketing authorization. Not registered as a medicinal product.
United Kingdom (MHRA):
No marketing authorization. Classification status unclear.
Australia (TGA):
Not listed or registered on the Australian Register of Therapeutic Goods.
Canada (Health Canada):
No Drug Identification Number (DIN) or Natural Product Number (NPN) assigned.
WADA Status:
Bronchogen does not appear on the World Anti-Doping Agency Prohibited List as of 2026. However, athletes should verify current status with their sport's anti-doping authority, as regulatory classification can change.
Active clinical trials:
None registered internationally as of March 2026.
Regulatory status changes frequently. Always verify the current legal status of any compound in your specific country or jurisdiction before making any decisions.
FAQ
What is Bronchogen used for?
Bronchogen is a tetrapeptide bioregulator studied primarily for its effects on respiratory tissue. Preclinical research has focused on its ability to support bronchial epithelial repair, reduce airway inflammation, and stabilize DNA in lung cells. It is explored by individuals interested in post-smoking lung recovery, chronic respiratory conditions, environmental pollution exposure, and age-related respiratory decline.
How is Bronchogen different from other respiratory peptides?
Bronchogen is distinguished by its organ specificity. While peptides like BPC-157 or TB-500 promote healing across many tissue types, Bronchogen preferentially accumulates in and affects lung tissue. This specificity is attributed to its interaction with lung-specific transcription factors and chromatin states. Chonluten (EDG tripeptide) is a related respiratory bioregulator that targets complementary pathways.
Is there human clinical evidence for Bronchogen?
No. All published evidence for Bronchogen comes from animal models (primarily rats with induced COPD) and in vitro cell culture studies. No human clinical trials have been conducted or registered. The peptide's use in human protocols is based on the broader Russian bioregulator clinical tradition rather than formal clinical trial evidence.
What doses are commonly discussed in the available literature?
Based on available sources, commonly reported ranges are 0.5 to 5 mg per day administered subcutaneously, with 1 to 2 mg per day being the most frequently cited range. Cycle lengths vary from 10 to 40 days, typically repeated every 3 to 6 months. These are not clinically validated dosing protocols. Consult a qualified healthcare professional for guidance specific to your situation.
Can Bronchogen be taken orally?
Oral bioregulator capsules are available in some markets, particularly from Russian manufacturers. Some evidence from related ultra-short peptides suggests resistance to intestinal peptidase degradation, which could support oral bioavailability. However, no formal bioavailability comparison between oral and injectable routes has been published for Bronchogen specifically.
What side effects have been reported?
Published preclinical studies report no significant adverse effects. Community reports describe high tolerability, with occasional brief flushing and temporary heart rate elevation (lasting minutes) being the most commonly noted response. The limited nature of the safety data means that rare or long-term adverse effects cannot be ruled out.
Can Bronchogen be combined with other peptides?
Community members frequently discuss stacking Bronchogen with Chonluten (a complementary respiratory bioregulator), Epithalon (systemic geroprotective), BPC-157, TB-500, or Thymosin Alpha-1. No formal interaction studies exist. Combining multiple bioactive compounds increases complexity and makes it difficult to attribute effects to any single agent. Discuss any combination protocols with a healthcare professional.
Sources & References
Animal Studies
- Kuzubova, N. A., Lebedeva, E. S., Dvorakovskaya, I. V., Surkova, E. A., Platonova, I. S., & Titova, O. N. (2015). "Modulating Effect of Peptide Therapy on the Morphofunctional State of Bronchial Epithelium in Rats with Obstructive Lung Pathology." Bulletin of Experimental Biology and Medicine, 159(5), 685-688. https://pubmed.ncbi.nlm.nih.gov/26468022/
- Titova, O. N., Kuzubova, N. A., Lebedeva, E. S., Preobrazhenskaya, T. N., Surkova, E. A., & Dvorakovskaya, I. V. (2017). "Antiinflammatory and Regenerative Effect of Peptide Therapy in the Model of Obstructive Lung Pathology." Rossiiskii Fiziologicheskii Zhurnal imeni I.M. Sechenova, 103(2), 201-208. https://pubmed.ncbi.nlm.nih.gov/30199201/
In Vitro / Molecular Studies
- Monaselidze, J. R., Khavinson, V. K., Gorgoshidze, M. Z., Khachidze, D. G., Lomidze, E. M., Jokhadze, T. A., & Lezhava, T. A. (2011). "Effect of the Peptide Bronchogen (Ala-Asp-Glu-Leu) on DNA Thermostability." Bulletin of Experimental Biology and Medicine, 150(3), 375-377. https://pubmed.ncbi.nlm.nih.gov/21240358/
- Fedoreyeva, L. I., Kireev, I. I., Khavinson, V. K., & Vanyushin, B. F. (2020). "Peptide AEDL alters chromatin conformation via histone binding." AIMS Biophysics, 7(1), 1-16. https://doi.org/10.3934/biophy.2020001
- Khavinson, V. K., Linkova, N. S., Polyakova, V. O., Kheifets, O. V., Tarnovskaya, S. I., & Kvetnoy, I. M. (2012). "Peptides tissue-specifically stimulate cell differentiation during their aging." Bulletin of Experimental Biology and Medicine, 153(1), 148-151. https://doi.org/10.1007/s10517-012-1664-1
- Khavinson, V. K., et al. (2014). "Peptide Regulation of Gene Expression and Protein Synthesis in Bronchial Epithelium." Lung, 192(5). https://doi.org/10.1007/s00408-014-9620-7
Reviews
- Ashapkin, V. V., Linkova, N. S., Khavinson, V. K., & Vanyushin, B. F. (2015). "Epigenetic mechanisms of peptidergic regulation of gene expression during aging of human cells." Biochemistry (Moscow), 80(3), 310-322. https://doi.org/10.1134/s0006297915030062
- Khavinson, V. K., Linkova, N. S., Diatlova, A., & Trofimova, S. (2019). "Peptide Regulation of Cell Differentiation." Stem Cell Reviews and Reports, 16, 118-125. https://doi.org/10.1007/s12015-019-09938-8
- Khavinson, V. K., et al. (2020). "Peptides: Prospects for Use in the Treatment of COVID-19." Molecules, 25(19), 4389. https://pmc.ncbi.nlm.nih.gov/articles/PMC7583759/
Supplementary References
- Zakutskii, A. N., et al. (2006). "The tissue-specific effect of synthetic peptides-biologic regulators in organotypic tissues culture in young and old rats." Advances in Gerontology, 19, 93-96.
- Fedoreyeva, L. I., et al. (2017). "Short Exogenous Peptides Regulate Expression of CLE, KNOX1, and GRF Family Genes in Nicotiana tabacum." Biochemistry (Moscow), 82(4), 521-528. https://doi.org/10.1134/S0006297917040149
Related Peptide Guides
- Epithalon — Systemic geroprotective bioregulator from the same Khavinson research program
- BPC-157 — Broad-spectrum healing peptide frequently discussed alongside Bronchogen
- TB-500 — Tissue repair peptide used in complementary stacking protocols
- Thymosin Alpha-1 — Immune modulator often paired with bioregulators
- GHK-Cu — Copper peptide with tissue remodeling properties, discussed for lung tissue support
- VIP — Vasoactive intestinal peptide recommended for complementary lung health support
- Pinealon — Neurological bioregulator from the Khavinson family
- Cardiogen — Cardiovascular bioregulator commonly paired in multi-organ protocols
- Cartalax — Connective tissue bioregulator from the same research program
- Vilon — Immune bioregulator dipeptide
Need the reconstitution math for Bronchogen: Complete Research Guide?
Open the calculator with Bronchogen: Complete Research Guide prefilled to estimate concentration, draw volume, and related measurement math from the reconstitution details you already have.