HCG (Human Chorionic Gonadotropin): Complete Research Guide
On this page
Quick Reference Card
Attribute
Also Known As
- Detail
- Human Chorionic Gonadotropin, hCG, Pregnyl, Novarel, Ovidrel, Choriogonadotropin alfa
Attribute
Administration
- Detail
- Injectable (subcutaneous, intramuscular)
Attribute
Research Status
- Detail
- FDA-approved for female infertility (ovulation induction), male hypogonadism, and cryptorchidism. Off-label use common as TRT adjunct for testicular maintenance and fertility preservation.
Attribute
Typical Dose Range
- Detail
- Maintenance: 250-500 IU 3x/week; Monotherapy: 500-1500 IU 3x/week; Recovery: 1,500-2,500 IU 3x/week
Attribute
Half-Life
- Detail
- Approximately 36 hours
Attribute
Cycle Length
- Detail
- 8-16 weeks typical; some protocols extend 6+ months
Attribute
Storage
- Detail
- Lyophilized: 2-8°C (refrigerate); Reconstituted: 2-8°C, stable up to 60 days. Do not freeze.
Overview / What Is HCG?
The Basics
HCG (Human Chorionic Gonadotropin) is a hormone that your body naturally produces during pregnancy. While that might sound like an odd starting point for a compound used primarily by men in hormone optimization, it makes perfect sense once you understand what HCG actually does at a cellular level: it mimics the signal your brain sends to your testes telling them to produce testosterone.
Your body has a chain of command for testosterone production. The brain sends a hormone called LH (luteinizing hormone) to the testes, and the testes respond by making testosterone along with other important hormones like pregnenolone and DHEA. HCG looks enough like LH to bind to the same receptors on testicular cells, effectively delivering that same "produce testosterone" signal. The key difference is that HCG sticks around much longer. Natural LH clears from your bloodstream in about 30 minutes. HCG lasts roughly 36 hours, providing a sustained signal that keeps the testes active [1][2].
This makes HCG particularly valuable in two scenarios. First, men on testosterone replacement therapy (TRT) often use HCG to prevent their testes from shrinking and shutting down, since exogenous testosterone tells the brain to stop sending the natural LH signal. Second, men with low testosterone who want to preserve their fertility may use HCG as a standalone therapy, since it stimulates natural testosterone production without shutting down sperm production the way exogenous testosterone does [3][4].
HCG has been used in medicine for decades and is one of the few peptide hormones with full FDA approval for multiple indications. It has also been used off-label for weight loss in combination with very low calorie diets, though clinical evidence does not support this application [14].
The Science
Human Chorionic Gonadotropin (hCG) is a heterodimeric glycoprotein hormone consisting of a 92-amino-acid alpha subunit (shared with LH, FSH, and TSH) and a unique 145-amino-acid beta subunit that confers receptor specificity [1]. With a molecular weight of approximately 25,700 daltons, HCG is substantially larger than most peptide therapeutics, and its glycosylation pattern is critical for biological activity and extended half-life [5].
HCG binds to the luteinizing hormone/choriogonadotropin receptor (LHCGR), a G-protein coupled receptor expressed primarily on testicular Leydig cells in males and ovarian theca/granulosa cells in females [1][2]. In males, this receptor activation triggers the cAMP/PKA signaling cascade, stimulating steroidogenesis through upregulation of StAR (Steroidogenic Acute Regulatory Protein) and CYP11A1 (cholesterol side-chain cleavage enzyme), the rate-limiting enzymes in testosterone biosynthesis [1].
Beyond testosterone production, HCG stimulates the full spectrum of testicular steroidogenesis, including pregnenolone, DHEA, progesterone, and estradiol. This distinguishes it from exogenous testosterone administration, which suppresses intratesticular hormone production through negative feedback on the hypothalamic-pituitary axis [3][4]. Clinical studies demonstrate that low-dose HCG (250-500 IU every other day) maintains intratesticular testosterone at near-baseline levels in men receiving exogenous testosterone therapy [4].
Molecular Identity
Attribute
Common Names
- Detail
- Human Chorionic Gonadotropin, hCG, HCG
Attribute
Classification
- Detail
- Glycoprotein hormone
Attribute
Molecular Weight
- Detail
- ~25,700 Da
Attribute
Subunit Structure
- Detail
- Alpha subunit (92 aa) + Beta subunit (145 aa)
Attribute
Origin
- Detail
- Naturally produced by placental trophoblast cells during pregnancy; pharmaceutical HCG sourced from pregnant urine or recombinant production
Attribute
Brands
- Detail
- Pregnyl, Novarel (urinary-derived); Ovidrel (recombinant choriogonadotropin alfa)
Mechanism of Action
The Basics
To understand how HCG works, think of testosterone production as a factory with three levels of management. The hypothalamus (top management) sends a signal called GnRH to the pituitary gland (middle management), which then sends LH and FSH to the testes (the factory floor). The testes receive these signals and produce testosterone, along with other hormones and sperm.
When a man takes exogenous testosterone, his brain detects the high testosterone levels and stops sending the LH/FSH signals. Without that signal, the testes gradually shrink and stop producing testosterone, sperm, and the full suite of downstream hormones. HCG enters this picture by mimicking LH. It goes directly to the factory floor and tells the testes to keep working, regardless of what the brain is (or is not) telling them.
This is also why HCG supports what researchers call the "neurosteroid advantage." Your testes do not just produce testosterone. They produce precursor hormones like pregnenolone and DHEA that play important roles in mood, cognition, stress resilience, and sleep quality. Exogenous testosterone alone cannot replicate this downstream hormone production. HCG, by stimulating the entire steroidogenic pathway, preserves access to this broader hormonal cascade.
The Science
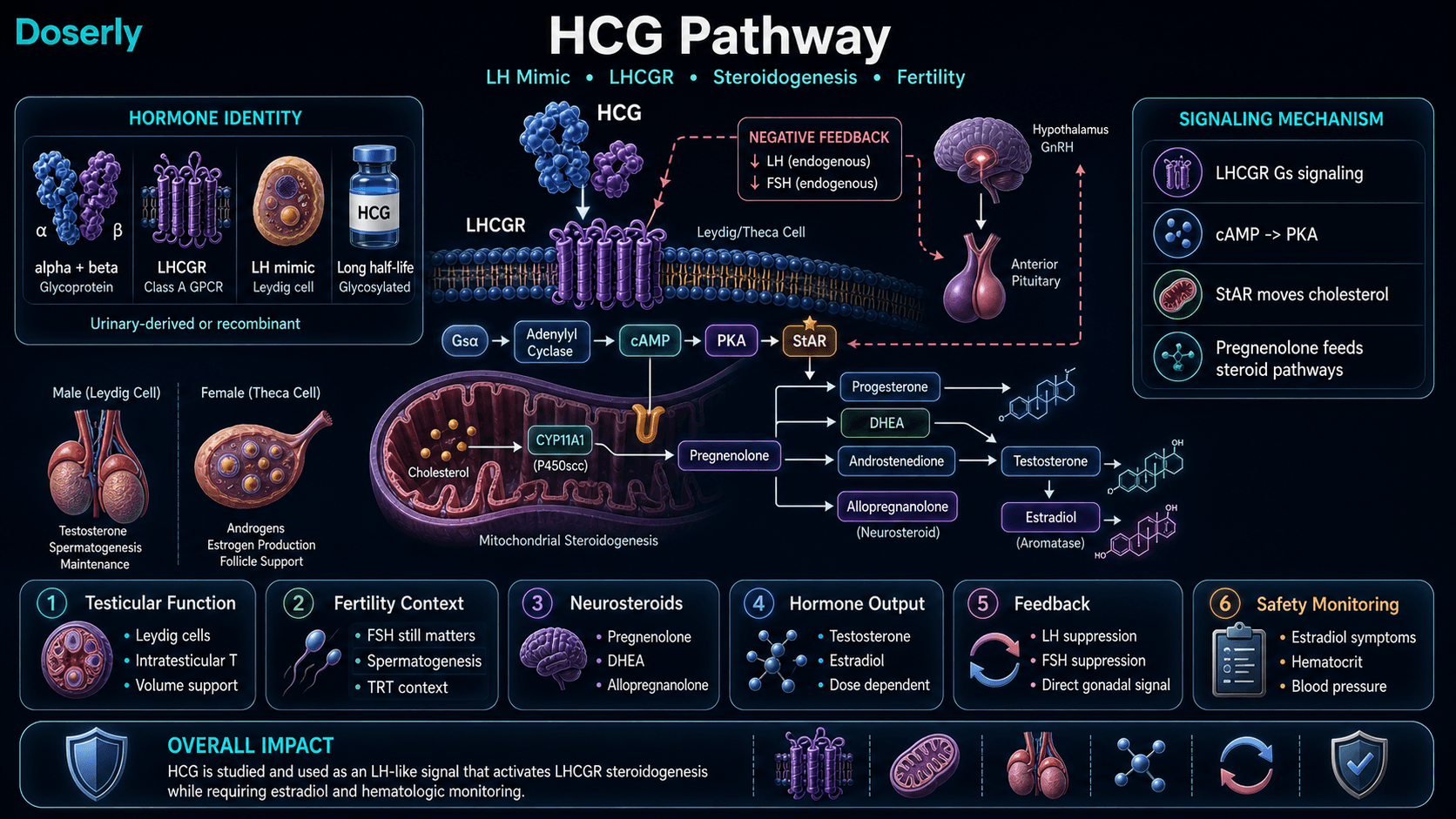
HCG exerts its effects through high-affinity binding to the LHCG receptor (LHCGR), a class A rhodopsin-like G-protein coupled receptor (GPCR). Upon ligand binding, LHCGR activates the Gs alpha subunit, stimulating adenylyl cyclase and increasing intracellular cyclic adenosine monophosphate (cAMP) concentrations [1][2].
The cAMP/PKA signaling cascade initiates acute steroidogenesis through phosphorylation and translocation of StAR protein to the outer mitochondrial membrane, facilitating cholesterol transport to the inner mitochondrial membrane where CYP11A1 catalyzes the first committed step of steroid biosynthesis: conversion of cholesterol to pregnenolone [1].
Pregnenolone then serves as the substrate for multiple downstream pathways:
- Delta-4 pathway: Pregnenolone to progesterone to androstenedione to testosterone (via 3beta-HSD and CYP17A1)
- Delta-5 pathway: Pregnenolone to DHEA to androstenediol to testosterone
- Neurosteroid pathway: Pregnenolone to allopregnanolone (a potent positive allosteric modulator of GABA-A receptors)
HCG's extended half-life (approximately 36 hours vs. 30 minutes for endogenous LH) results from extensive glycosylation of the beta subunit, which reduces renal clearance and hepatic degradation [2]. This pharmacokinetic profile enables a three-times-weekly dosing schedule to maintain sustained gonadal stimulation.
Notably, while HCG stimulates the LHCGR, it does suppress endogenous LH and FSH secretion through negative feedback from the resulting testosterone and estradiol elevation. However, because HCG directly stimulates testicular function, intratesticular testosterone and spermatogenesis are maintained even in the presence of suppressed gonadotropins [3][4].
Pathway Visualization Image
Pharmacokinetics
The Basics
HCG stays active in your body much longer than the natural hormone it mimics. While your body's own LH disappears from the bloodstream in about 30 minutes, HCG persists for approximately 36 hours. This extended activity is the main reason HCG works with a three-times-per-week dosing schedule rather than requiring daily or multiple daily injections.
After a subcutaneous injection, HCG levels in the blood peak within a few hours and then gradually decline over the next day and a half. The sustained stimulation means your testes receive a consistent "produce testosterone" signal across the dosing interval, though there will be some natural fluctuation between doses.
One practical consideration: because HCG also stimulates estradiol production through testicular aromatase, the estrogen effects from a single dose can linger. This is why some individuals find that dose adjustments or estrogen management strategies take time to show their full effect.
The Science
Following subcutaneous administration, HCG demonstrates rapid absorption with time to peak plasma concentration (Tmax) of approximately 6-16 hours, depending on formulation and individual factors [2]. The terminal elimination half-life is approximately 29-36 hours, substantially longer than endogenous LH (half-life ~30 minutes) due to extensive sialylation and glycosylation of the HCG beta subunit [2].
Bioavailability following subcutaneous injection is approximately 75-80%, comparable to intramuscular administration. The volume of distribution is approximately 5-6 L, indicating primarily extracellular distribution [2].
HCG clearance occurs primarily through hepatic metabolism and renal excretion of metabolic fragments. The extended half-life supports a dosing interval of 48-72 hours (three-times-weekly or every-other-day protocols) for sustained gonadal stimulation without the need for daily administration [2][4].
Testosterone response kinetics following HCG administration show measurable increases in intratesticular testosterone within 2-4 hours, with peak response at approximately 24-72 hours depending on dose. At maintenance doses (250-500 IU), steady-state testosterone elevation is typically achieved within 1-2 weeks of initiating a consistent dosing schedule [4].
Research & Clinical Evidence
The Basics
HCG has one of the strongest evidence bases of any compound in this guide series, partly because it is FDA-approved and has been used in clinical medicine for decades. The research spans fertility treatment, testosterone optimization, testicular maintenance during TRT, and (controversially) weight loss.
The most robust evidence supports HCG for maintaining testicular function and fertility in men on testosterone therapy. Studies consistently show that adding HCG to a TRT protocol prevents the testicular atrophy and fertility decline that typically accompany exogenous testosterone use. For men who want the benefits of testosterone therapy without sacrificing their ability to father children, HCG addresses a real and well-documented problem.
As a standalone therapy for low testosterone (HCG monotherapy), the evidence is more mixed. Some men achieve significant testosterone increases and symptom relief, while others find the response insufficient compared to direct testosterone replacement. The response appears to depend heavily on the underlying cause of low testosterone, particularly whether the problem originates in the brain's signaling (secondary hypogonadism) or in testicular function itself (primary hypogonadism).
The weakest evidence surrounds HCG for weight loss. Despite widespread promotion as a weight loss aid alongside very low calorie diets, a meta-analysis concluded there is no scientific evidence that HCG contributes to weight loss beyond what the severe caloric restriction alone would achieve [14].
The Science
Male Hypogonadism and TRT Adjunct Therapy
Coviello et al. (2005) demonstrated in a controlled study that low-dose HCG (250 IU every other day) co-administered with 200 mg/week testosterone enanthate maintained intratesticular testosterone (ITT) at 25% of baseline, compared to a 94% reduction with testosterone alone [4]. At 500 IU every other day, ITT was maintained at 7-fold above the testosterone-only group. This landmark study established the evidence basis for HCG as a fertility-preserving adjunct to TRT.
Fertility Preservation
Lee and Ramasamy (2018) reviewed the evidence for HCG in male infertility, noting that HCG at doses of 1,500-5,000 IU administered 2-3 times weekly stimulates spermatogenesis and testosterone production in hypogonadotropic hypogonadism [3]. When combined with human menopausal gonadotropin (HMG), HCG-based protocols can restore sperm production in the majority of men with gonadotropin deficiency.
HCG Monotherapy
HCG monotherapy (without concurrent TRT) has been used for men who wish to raise testosterone while preserving natural hormonal architecture. Clinical protocols typically employ 500-2,000 IU three times weekly. Response rates vary, with men demonstrating secondary hypogonadism (low LH/FSH) generally showing better testosterone responses than those with primary testicular failure (elevated LH/FSH) [3][5].
Weight Loss
Lijesen et al. (1995) conducted a meta-analysis of clinical trials examining HCG for weight loss and concluded that there is no scientific evidence supporting HCG as an effective adjunct to caloric restriction for weight reduction [14]. The FDA has not approved HCG for weight loss, and the American Medical Association has stated that HCG has no proven benefit for this indication.
Biomarker Evidence Matrix
Category
Libido
- Evidence Strength
- 7/10
- Reported Effectiveness
- 8/10
- Summary
- Strong clinical evidence for testosterone-mediated libido improvement. Community reports consistently describe significant libido increases, often exceeding TRT alone.
Category
Sexual Function
- Evidence Strength
- 7/10
- Reported Effectiveness
- 7/10
- Summary
- Clinical evidence supports improved erectile function through testosterone restoration. Community reports note increased sensitivity, semen volume, and testicular size.
Category
Mood & Wellbeing
- Evidence Strength
- 6/10
- Reported Effectiveness
- 7/10
- Summary
- Moderate clinical evidence via testosterone normalization. Community reports strong improvements in mood, sense of wellbeing, and reduced depression; attributed to neurosteroid production.
Category
Hormonal Symptoms
- Evidence Strength
- 8/10
- Reported Effectiveness
- 6/10
- Summary
- Well-established clinical mechanism (LH receptor agonism). Community reports mixed due to estradiol elevation as a complicating factor.
Category
Energy Levels
- Evidence Strength
- 5/10
- Reported Effectiveness
- 7/10
- Summary
- Limited HCG-specific energy data; general testosterone normalization improves energy. Community reports consistently positive.
Category
Motivation & Drive
- Evidence Strength
- 4/10
- Reported Effectiveness
- 6/10
- Summary
- Mechanism-inferred via testosterone and neurosteroid pathways. Some community support.
Category
Sleep Quality
- Evidence Strength
- 3/10
- Reported Effectiveness
- 6/10
- Summary
- Limited direct evidence. Neurosteroid (allopregnanolone) pathway provides mechanistic rationale. Few direct community reports.
Category
Anxiety
- Evidence Strength
- 3/10
- Reported Effectiveness
- 5/10
- Summary
- No direct HCG-anxiety studies. Community reports mixed; some report reduction, others report worsening linked to estradiol elevation.
Category
Emotional Regulation
- Evidence Strength
- 3/10
- Reported Effectiveness
- 5/10
- Summary
- No direct evidence. Community reports mixed; depends on estrogen management.
Category
Fluid Retention
- Evidence Strength
- 6/10
- Reported Effectiveness
- 5/10
- Summary
- Well-characterized pharmacological effect via estradiol elevation. Community commonly reports puffiness and water retention.
Category
Skin Health
- Evidence Strength
- 3/10
- Reported Effectiveness
- 4/10
- Summary
- Known side effect of acne/oily skin from androgen elevation. Mixed community reports.
Category
Fat Loss
- Evidence Strength
- 2/10
- Reported Effectiveness
- 5/10
- Summary
- Meta-analysis found no evidence for direct fat loss benefit. Weight loss reports confounded by VLCD protocols.
Category
Muscle Growth
- Evidence Strength
- 4/10
- Reported Effectiveness
- 5/10
- Summary
- Indirect support via testosterone elevation. HCG monotherapy typically achieves lower testosterone levels than TRT.
Category
Side Effect Burden
- Evidence Strength
- 7/10
- Reported Effectiveness
- 5/10
- Summary
- Well-characterized side effect profile. Generally well-tolerated at standard doses; estrogen-related effects are the primary management challenge.
Category
Blood Pressure
- Evidence Strength
- 5/10
- Reported Effectiveness
- 5/10
- Summary
- Testosterone products carry FDA BP monitoring requirements per TRAVERSE trial data. Community reports occasional concerns.
Benefits & Potential Effects
The Basics
HCG offers a set of benefits that center on keeping your body's testosterone-producing machinery running, even when other treatments or conditions would otherwise shut it down. The most clearly established benefits include:
Testicular maintenance and fertility preservation. For men on testosterone therapy, HCG prevents the testicular shrinkage (atrophy) that naturally occurs when external testosterone tells the brain to stop sending production signals. This is not just a cosmetic concern. Maintaining testicular function preserves sperm production and the full range of hormones the testes produce.
Testosterone restoration. Men with low testosterone may experience meaningful increases in testosterone levels on HCG. How much of an increase depends on the underlying cause. If the problem is weak signaling from the brain (secondary hypogonadism), HCG can sometimes restore testosterone to normal ranges. If the testes themselves are the limiting factor (primary hypogonadism), the response may be more modest.
Neurosteroid production. This is where HCG distinguishes itself from simple testosterone replacement. By stimulating the entire steroidogenic pathway, HCG supports production of pregnenolone, DHEA, progesterone, and allopregnanolone. These downstream hormones influence mood, cognitive function, stress tolerance, and sleep quality in ways that exogenous testosterone alone does not replicate.
Libido and sexual function. Community reports consistently describe HCG as a strong enhancer of sexual desire and function, with many users reporting that it provides benefits above and beyond what testosterone alone achieves. Increased sensitivity, semen volume, and erectile quality are among the most commonly reported effects.
The Science
The therapeutic benefits of HCG derive from its ability to stimulate LHCGR-mediated steroidogenesis, providing both direct androgenic effects (via testosterone) and indirect effects through the broader steroidogenic cascade [1][3][4].
Intratesticular testosterone maintenance: Coviello et al. demonstrated that 250 IU HCG every other day maintains intratesticular testosterone at levels sufficient to support spermatogenesis in men receiving exogenous testosterone [4]. This finding has direct clinical relevance for fertility preservation.
Neurosteroid cascade: Unlike exogenous testosterone, which suppresses gonadotropin-driven intratesticular steroidogenesis, HCG maintains production of pregnenolone and its metabolites. Allopregnanolone, a potent positive allosteric modulator of GABA-A receptors, has demonstrated anxiolytic, sedative, and neuroprotective properties in preclinical models [6]. DHEA serves as a precursor for both androgens and estrogens and has been associated with improved mood and cognitive function in aging populations [7].
Testicular volume preservation: HCG maintains Leydig cell mass and function, preventing the atrophy that occurs with gonadotropin suppression during TRT. Testicular volume is a validated clinical marker of spermatogenic capacity [3].
Reading about potential benefits is the starting point. Knowing whether you're actually experiencing them is where real value begins. Doserly lets you track the specific health markers that matter for your protocol, from body composition and energy levels to sleep quality, mood, and recovery time, building a personal dataset that goes beyond subjective impressions.
The app's proactive monitoring doesn't wait for you to notice a problem. It surfaces patterns in your logged data that might suggest suboptimal timing, flags potential interactions with other items in your health stack, and helps you identify which benefits are tracking with what the research suggests and which aren't materializing. Think of it as a second set of eyes on your protocol, always watching the trends.
Connect protocol changes to labs and health markers.
Doserly can keep lab results, biomarkers, symptoms, and dose history close together so follow-up conversations have better context.
Insights
Labs and trends

Doserly organizes data; it does not diagnose or interpret labs for you.
Side Effects & Safety Considerations
The Basics
HCG is generally well-tolerated at standard doses, and its side effect profile is well-understood given decades of clinical use. The most important thing to know is that nearly all significant side effects trace back to one mechanism: estrogen elevation.
When HCG stimulates testosterone production, some of that testosterone gets converted to estradiol by an enzyme called aromatase. The testes have their own aromatase, so HCG can increase estradiol more directly than you might expect. At standard maintenance doses (250-500 IU three times weekly), most men manage fine. At higher doses (1,000+ IU per injection), estradiol can climb quickly and cause noticeable symptoms.
Common effects to be aware of:
- Water retention and puffiness. The most frequently reported cosmetic side effect, driven by elevated estradiol. Often described as looking "puffy" or carrying extra water weight.
- Breast tenderness or gynecomastia risk. Elevated estradiol can cause breast tissue sensitivity. Persistent cases may require estrogen management.
- Acne and oily skin. A consequence of increased testosterone and DHT production. Usually mild at standard doses.
- Testicular aching. Some men experience temporary testicular discomfort, particularly when reactivating dormant Leydig cells. Typically resolves within the first few weeks.
- Headaches. Reported in some clinical studies and patient reviews.
- Mood changes. Estradiol elevation can cause irritability, anxiety, or emotional reactivity in some individuals. Conversely, crashed estradiol from overzealous aromatase inhibitor use creates its own set of problems (joint pain, libido loss, mood flattening).
Important safety considerations:
- Blood pressure monitoring is recommended, particularly in the early weeks. Updated FDA labeling for testosterone products includes BP monitoring requirements based on the TRAVERSE trial data.
- Hematocrit monitoring is important for any testosterone-elevating therapy. Rising hematocrit (commonly using a threshold around 54%) warrants clinical evaluation.
- HCG is not appropriate for men with certain conditions, including hormone-sensitive cancers.
The Science
The adverse effect profile of HCG is primarily driven by supraphysiologic estradiol production via intratesticular aromatase (CYP19A1) activation [3]. Unlike peripheral aromatization of exogenous testosterone, intratesticular estradiol production from HCG-stimulated testosterone may be less responsive to systemic aromatase inhibitors, as the local concentration gradient within the testes is high [8].
Clinically documented adverse effects include:
- Estradiol elevation: Dose-dependent increase in serum estradiol. At doses above 1,000 IU three times weekly, estradiol commonly exceeds 40-60 pg/mL, and may reach 80-100+ pg/mL at higher doses [8].
- Gynecomastia: Incidence is low at maintenance doses but increases with dose escalation. Related to the estradiol/testosterone ratio rather than absolute estradiol levels.
- Fluid retention/edema: Estrogen-mediated sodium and water retention. Generally mild and reversible with dose reduction.
- Hematocrit elevation: Any testosterone-elevating therapy can stimulate erythropoiesis. Standard monitoring protocols recommend CBC assessment at baseline, 3 months, and periodically thereafter [8].
- Blood pressure effects: The TRAVERSE trial (testosterone gel vs. placebo, N=5,204) documented modest increases in systolic and diastolic BP with testosterone use, leading to updated FDA labeling requirements for all testosterone products [8].
HCG is contraindicated in individuals with androgen-dependent neoplasia, precocious puberty, and severe hypersensitivity to HCG preparations [9].
The side effects and contraindications above give you a map of what to watch for. Doserly turns that map into a daily practice. Log the specific biomarkers and symptoms associated with this compound's known risk profile, and the app builds a timeline of how your body is responding across your cycle.
Trending in the wrong direction on a key marker? Noticing a pattern that started two weeks into your protocol? Doserly connects the dots between your protocol timeline and your logged data, making it easier to spot emerging issues early and have informed, data-backed conversations with your healthcare provider about what's working and what needs attention.
Capture changes while they are still fresh.
Log symptoms, energy, sleep, mood, and other observations alongside protocol events so patterns do not live only in memory.
Trend view
Symptom timeline

Symptom tracking is informational and should be interpreted with a qualified clinician.
Dosing Protocols
The Basics
HCG dosing varies significantly depending on the goal, and this is one of the most important distinctions to understand. A maintenance dose designed to keep the testes active during TRT is very different from a monotherapy dose intended to raise testosterone as a standalone treatment, which is itself different from a high-dose recovery protocol used after prolonged suppression.
Common protocol categories reported in the literature and community:
TRT Adjunct (Maintenance): The most frequently cited maintenance protocol involves 250-500 IU administered subcutaneously three times per week (e.g., Monday/Wednesday/Friday). At the lower end, 250 IU every other day has been shown in clinical research to maintain intratesticular testosterone. The 500 IU three-times-weekly protocol is the most commonly reported community standard for balancing testicular maintenance with manageable estradiol levels.
Monotherapy: For men using HCG as their sole testosterone-raising intervention, doses typically range from 500 to 1,500 IU three times per week. Some practitioners start at the lower end and titrate upward based on bloodwork and symptom response. The literature includes protocols as high as 2,000 IU every other day for specific clinical situations, though most sources suggest doses above 2,000 IU weekly substantially increase estradiol-related side effects.
Post-Cycle Recovery: Higher doses (1,500-2,500 IU three times weekly) have been used to reactivate testosterone production after prolonged androgen use. These protocols typically run 4-12 weeks and are often followed by dose tapering to maintenance levels.
Because HCG has a half-life of approximately 36 hours, three-times-weekly injection schedules provide consistent stimulation without the need for daily administration. Most protocols recommend maintaining consistent timing and rotating injection sites.
The Science
Evidence-based dosing parameters for HCG in male patients include:
Testicular maintenance during TRT: Coviello et al. established that 250 IU SC every other day (approximately 875 IU/week) maintains intratesticular testosterone at 25% of baseline during concurrent testosterone administration, while 500 IU EOD maintains higher levels [4]. The Drugs.com prescribing reference cites 500-1,000 IU IM three times weekly for male hypogonadism [9].
Hypogonadotropic hypogonadism: Lee and Ramasamy reviewed standard regimens of 1,500-5,000 IU administered 2-3 times weekly, with higher doses used for fertility induction, often combined with HMG (75-150 IU FSH three times weekly) [3].
Monotherapy: No standardized monotherapy protocol exists in the peer-reviewed literature. Clinical practice varies from 500 IU to 2,000 IU three times weekly, with dose adjustment guided by serum testosterone, free testosterone, and estradiol monitoring [3][5].
Dose-response considerations: The testosterone response to HCG demonstrates a dose-dependent relationship with diminishing returns at higher doses [4]. Estradiol production also increases with dose, and at doses exceeding 1,000 IU per injection, the estradiol increase may become disproportionate relative to testosterone gains.
Consistency is the difference between a protocol that delivers results and one that wastes time and money. Doserly was built for exactly this: keeping you on track with the precision your protocol demands.
The built-in calculators handle the math you shouldn't be doing in your head. The reconstitution calculator tells you exactly how much bacteriostatic water to add for your target concentration. The dose calculator converts between units, milligrams, and syringe markings so you draw the right amount every time. The injection site heat map tracks where you've administered and when, helping you rotate sites systematically to reduce tissue damage, scarring, and absorption inconsistencies from overusing the same area. Pair that with smart reminders tuned to your protocol's timing requirements, and you build the kind of daily consistency that separates optimized protocols from haphazard ones.
Track injection timing, draw notes, and site rotation.
Doserly helps keep syringe-related notes, injection site history, reminders, and reconstitution context together for easier review.
Injection log
Site rotation
Injection logs support record-keeping; follow clinician instructions for administration.
What to Expect
Weeks 1-2: Some users report noticeable effects within the first few days, including improved mood, increased sense of wellbeing, and enhanced libido. Testicular aching is common in the first week as dormant Leydig cells reactivate. Initial blood work typically shows some testosterone elevation by the end of week 2.
Weeks 3-4: Testosterone levels approach steady state on most protocols. Libido and energy improvements become more consistent. Testicular size begins to increase if atrophy was present. Estradiol-related effects (water retention, mood changes) may emerge, particularly at higher doses. First follow-up bloodwork is typically recommended around week 4.
Weeks 5-8: Full protocol effects are generally established. Testosterone and estradiol levels stabilize. Men using HCG for fertility should note that spermatogenesis takes approximately 72-74 days for a complete cycle, so sperm count improvements may not be evident until this timeframe. Body composition changes (if occurring) begin to become noticeable.
Weeks 8-12+: Long-term optimization phase. Second round of bloodwork recommended around week 8-12 to confirm stable hormone levels and assess whether dose adjustments are needed. Men on monotherapy protocols can evaluate whether their testosterone response is sufficient for their goals.
Long-term (3-6+ months): Some individuals have maintained HCG protocols for years. Long-term data from fertility clinic use supports sustained efficacy without significant tachyphylaxis at standard doses, though some community reports suggest diminishing response over time at very high doses.
Interaction Compatibility
Good With (Synergistic)
- Testosterone (TRT): HCG is most commonly used alongside testosterone replacement therapy to maintain testicular function and fertility. This is the most well-established combination.
- Gonadorelin: A GnRH analog that can be used alongside or as an alternative to HCG for maintaining gonadotropin levels during TRT.
- Kisspeptin: Stimulates GnRH release upstream, potentially enhancing the entire HPT axis. Some fertility protocols combine with HCG.
- Enclomiphene/Clomiphene: SERMs that stimulate LH/FSH release. Can be used sequentially with HCG in step-down protocols or for diagnostic purposes.
Use with Caution
- Aromatase Inhibitors (Anastrozole, Exemestane): May be needed to manage HCG-induced estradiol elevation but carry their own risks. Over-suppression of estradiol causes joint pain, libido loss, mood flattening, and negative lipid effects. Lab-guided, symptom-based use is strongly preferred over prophylactic dosing.
- PT-141: Combining two libido-enhancing compounds may produce excessive stimulation in sensitive individuals.
Not Good With
- Other LH-mimicking compounds at concurrent doses: Redundant receptor stimulation without additional benefit.
- 5-alpha reductase inhibitors (finasteride, dutasteride): May alter the androgenic profile of HCG-stimulated testosterone production and reduce DHT-mediated benefits.
Administration Guide
HCG is most commonly administered via subcutaneous injection using insulin syringes (29-31 gauge, 0.5 inch needle). Intramuscular injection is also an option but subcutaneous delivery is preferred for its convenience and comparable bioavailability.
Materials typically required:
- HCG vial (lyophilized powder, typically 5,000 or 10,000 IU)
- Bacteriostatic water for reconstitution
- Insulin syringes (U-100, 29-31 gauge)
- Alcohol swabs
- Sharps disposal container
Recommended reconstitution solution: Bacteriostatic water (BAC water) is the standard reconstitution solvent for HCG. The most common concentration used is 2.0 mL BAC water per 5,000 IU vial, yielding 2,500 IU/mL. This makes dose calculation straightforward on a U-100 insulin syringe (1 unit = 25 IU).
Timing considerations: There is no established optimal time of day for HCG administration. Some users report a stimulatory effect that can interfere with sleep, leading them to prefer morning or afternoon injections. Consistent timing relative to other protocol components (e.g., testosterone injections) is recommended.
Post-administration care: Monitor for injection site reactions (mild redness or discomfort is normal). Return the vial to refrigeration promptly. Document injection date, dose, and site for tracking purposes.
Supplies & Planning
Typical supplies associated with HCG protocols:
- HCG vials: Available in 5,000 IU and 10,000 IU lyophilized presentations (pharmaceutical brands include Pregnyl and Novarel; compounding pharmacies also produce HCG)
- Bacteriostatic water: 10 mL multi-use vials (approximately 2.0 mL used per 5,000 IU vial reconstitution)
- Insulin syringes: U-100, 0.5-1.0 mL capacity, 29-31 gauge, 0.5 inch needle. One new syringe per injection (do not reuse)
- Alcohol swabs: Two per injection session (one for vial stopper, one for injection site)
- Sharps container: For safe disposal of used syringes
The specific quantities depend on the protocol, dose, and duration selected in consultation with a healthcare provider. Use the reconstitution calculator to determine appropriate mixing volumes for your specific vial size and target concentration.
Storage & Handling
Lyophilized (unreconstituted) HCG:
- Store refrigerated at 2-8°C (35.6-46.4°F)
- Can tolerate room temperature for short periods but refrigeration is strongly preferred for maintaining potency
- Protect from light; store in original packaging or light-protected container
Reconstituted HCG:
- Must be refrigerated at 2-8°C (35.6-46.4°F)
- Stable for up to 60 days when reconstituted with bacteriostatic water (per FDA prescribing information for Pregnyl/Novarel)
- Do NOT freeze reconstituted HCG; freezing denatures the protein and destroys biological activity
- Label the vial with the reconstitution date and concentration
- Discard if the solution becomes cloudy, discolored, or contains visible particles
Handling best practices:
- Always use sterile technique when drawing doses
- Wipe the vial stopper with an alcohol swab before each needle insertion
- Minimize repeated temperature fluctuations (take the vial out, draw your dose, return it promptly)
- Store away from direct sunlight and heat sources
Lifestyle Factors
The effectiveness of any testosterone-related protocol, including HCG, is significantly influenced by foundational health factors. Addressing these creates the conditions for optimal hormonal response.
Sleep: Aim for 7-9 hours of quality sleep per night. Sleep deprivation is one of the most potent suppressors of testosterone production and impairs the hormonal recovery that HCG aims to support. If you are experiencing symptoms suggestive of sleep apnea (loud snoring, witnessed breathing pauses, excessive daytime sleepiness), evaluation is recommended, as untreated sleep apnea both suppresses testosterone and magnifies the cardiovascular risks associated with any testosterone-elevating therapy.
Nutrition: Adequate dietary fat intake (particularly saturated and monounsaturated fats) supports the cholesterol substrate pool needed for steroidogenesis. Zinc (found in oysters, red meat, pumpkin seeds) acts as a mild aromatase modulator. Vitamin D and magnesium are also associated with testosterone production. Protein intake supports the anabolic response to testosterone.
Exercise: Resistance training is the exercise modality most consistently associated with supporting anabolic hormone production. Chronic excessive endurance training can suppress testosterone through cortisol elevation. A balanced approach combining resistance training with moderate cardiovascular exercise is generally recommended.
Body composition: Higher body fat percentage increases aromatase activity, which can exacerbate HCG's estradiol-elevating effects. Maintaining a healthy body composition (generally below 20% body fat for men) creates a more favorable testosterone-to-estradiol ratio.
Stress management: Chronic stress elevates cortisol, which directly antagonizes testosterone production and can worsen the mood-related side effects of hormonal fluctuation. Structured stress management practices (meditation, breathing exercises, adequate recovery) support the hormonal environment HCG aims to optimize.
Alcohol: Excessive alcohol consumption impairs testosterone production, increases aromatase activity, and stresses the liver. Moderation is recommended during any hormone optimization protocol.
Testicular temperature: Elevated scrotal temperature impairs spermatogenesis. For men using HCG for fertility preservation, minimizing hot tub/sauna exposure, avoiding tight underwear, and reducing laptop-on-lap positioning may be beneficial.
Regulatory Status & Research Classification
United States (FDA): HCG is FDA-approved for the treatment of female infertility (ovulation induction), male hypogonadism, and prepubertal cryptorchidism. Pharmaceutical preparations include Pregnyl and Novarel (urinary-derived) and Ovidrel (recombinant choriogonadotropin alfa). Compounding pharmacies also produce HCG preparations. HCG was briefly impacted by FDA Category 2 compounding restrictions but remains available through both prescription pharmaceutical products and compounding pharmacies.
Canada (Health Canada): HCG is available by prescription for approved indications similar to FDA approvals.
United Kingdom (MHRA): Available as a prescription medication for fertility and hypogonadism indications.
Australia (TGA): Available as a prescription medication. Schedule 4 (Prescription Only).
European Union (EMA): Available across EU member states under various brand names for approved fertility and hypogonadism indications.
WADA Status: HCG is prohibited at all times (in-competition and out-of-competition) under the World Anti-Doping Agency Prohibited List, classified under S2 (Peptide Hormones, Growth Factors, Related Substances and Mimetics). A Therapeutic Use Exemption (TUE) is required for athletes with legitimate medical need.
Active clinical trials: Multiple ongoing clinical trials are registered on ClinicalTrials.gov examining HCG in contexts including male infertility, TRT adjunct therapy, and reproductive endocrinology. As an FDA-approved compound, HCG has an extensive clinical evidence base spanning decades.
Regulatory status changes frequently. Always verify the current legal status of any compound in your specific country or jurisdiction before making any decisions.
FAQ
What is the difference between HCG and testosterone replacement therapy (TRT)?
TRT introduces testosterone directly into the body from an external source. HCG stimulates your testes to produce testosterone naturally. The key practical differences are that HCG preserves testicular function, fertility, and the full spectrum of testicular hormone production (including pregnenolone and DHEA), while TRT suppresses these functions. However, TRT generally achieves higher and more predictable testosterone levels. Many protocols combine both.
Can HCG be used to preserve fertility while on TRT?
This is one of HCG's most well-established clinical applications. Research demonstrates that HCG co-administered with exogenous testosterone maintains intratesticular testosterone at levels sufficient to support spermatogenesis. Most fertility-focused TRT protocols include HCG for this reason.
Does HCG raise estrogen?
Yes. HCG stimulates testicular aromatase, which converts a portion of the newly produced testosterone into estradiol. The degree of estradiol elevation is dose-dependent. At maintenance doses (250-500 IU three times weekly), most men manage without issue. At higher doses, estrogen management strategies may be needed. Monitoring bloodwork is the most reliable way to assess individual estradiol response.
How long does it take to feel the effects of HCG?
Some users report mood and wellbeing changes within the first few days, though these early effects may involve placebo response. Measurable testosterone elevation typically occurs within 1-2 weeks. Full protocol effects (including fertility markers) require 8-12 weeks. Spermatogenesis takes approximately 72-74 days for a complete cycle.
Is HCG effective for weight loss?
Based on available clinical evidence, HCG does not contribute to weight loss beyond what caloric restriction alone achieves. A meta-analysis published in the British Journal of Clinical Pharmacology found no scientific evidence supporting HCG as a weight loss agent. Any weight loss observed on "HCG diet" protocols is attributable to the very low calorie diet (typically 500 calories/day), not HCG itself [14].
What should I monitor while using HCG?
Based on clinical practice patterns, commonly monitored parameters include: total and free testosterone, estradiol (sensitive assay), hematocrit/hemoglobin (CBC), blood pressure, and PSA (age/risk-dependent). Baseline values before starting and follow-up at approximately 6 weeks, 3 months, and periodically thereafter is a schedule many practitioners follow. Additional markers such as LH, FSH, DHEA-S, and pregnenolone may be relevant depending on the clinical context.
Can HCG be used long-term?
HCG has been used for extended periods (1-2+ years) in fertility clinic settings. Data from long-term use supports sustained efficacy without clinically significant tachyphylaxis at standard therapeutic doses. Some community reports suggest diminishing response at very high doses over extended periods, though this is not well-documented in the clinical literature.
Sources & References
Clinical Studies and Reviews
[1] National Center for Biotechnology Information (NCBI). Human Chorionic Gonadotropin: structure, function, and LH receptor binding mechanisms. https://www.ncbi.nlm.nih.gov/
[2] Seminars in Reproductive Medicine. Pharmacokinetics and pharmacodynamics of HCG: extended half-life and sustained activity.
[3] Lee JA, Ramasamy R. Indications for the use of human chorionic gonadotropic hormone for the management of infertility in hypogonadal men. Translational Andrology and Urology. 2018;7(Suppl 3):S348-S352. https://pubmed.ncbi.nlm.nih.gov/30159241/
[4] Coviello AD, Matsumoto AM, Bremner WJ, et al. Low-dose human chorionic gonadotropin maintains intratesticular testosterone in normal men with testosterone-induced gonadotropin suppression. Journal of Clinical Endocrinology & Metabolism. 2005;90(5):2595-2602. https://pubmed.ncbi.nlm.nih.gov/15713727/
[5] Morita H, Maruo T. Human chorionic gonadotropin (hCG) and subunits. 2005.
[6] Schumacher A. Human Chorionic Gonadotropin as a Pivotal Endocrine Immune Regulator Initiating and Preserving Fetal Tolerance. International Journal of Molecular Sciences. 2017;18(10):2166.
[7] Szczerba A, Bialas P, Pieta PP, Jankowska A. hCG-related molecules and their measurement. 2016.
[8] Male Infertility Guide. Clinical commentary on hCG dosing: 500 IU SC 3x/week for maintenance; 1,000-4,000 IU 3x/week for post-androgen recovery.
[9] Drugs.com. HCG Dosage Guide. Adult dose for male hypogonadism: 500-1,000 IU IM 3x/week. https://www.drugs.com/dosage/chorionic-gonadotropin-hcg.html
[10] Mayo Clinic. Chorionic Gonadotropin drug description: uses for ovulation induction, sperm production, and cryptorchidism treatment.
[11] FDA Prescribing Information. Chorionic Gonadotropin (Pregnyl/Novarel): reconstituted solution stable for 60 days when refrigerated; do not freeze.
[12] University Hospitals Fertility Center. SC injection technique for HCG.
[13] CDC. Vaccine administration guidelines: subcutaneous injection technique.
[14] Lijesen GK, Theeuwen I, Assendelft WJ, Van Der Wal G. The effect of human chorionic gonadotropin (HCG) in the treatment of obesity by means of the Simeons therapy: a criteria-based meta-analysis. British Journal of Clinical Pharmacology. 1995;40(3):237-243. https://pubmed.ncbi.nlm.nih.gov/8527285/
Related Peptide Guides
- Gonadorelin — GnRH analog used for gonadotropin stimulation; alternative mechanism for maintaining testicular function
- Kisspeptin — Upstream reproductive peptide regulating GnRH release; complementary approach to HPT axis stimulation
- PT-141 (Bremelanotide) — FDA-approved melanocortin receptor agonist for sexual dysfunction; different mechanism from HCG's hormonal approach
- Oxytocin — Social bonding hormone with stress relief properties; complementary reproductive hormone
- Tesamorelin — FDA-approved GH secretagogue; sometimes co-administered in comprehensive hormone optimization protocols
- Ipamorelin — Selective GH secretagogue; often part of broader peptide protocols alongside HCG
- Sermorelin — GHRH analog; commonly discussed alongside HCG in comprehensive hormone optimization
- Follistatin-344 — Myostatin inhibitor for muscle growth; different pathway from HCG's androgenic effects
Need the reconstitution math for HCG (Human Chorionic Gonadotropin): Complete Research Guide?
Open the calculator with HCG (Human Chorionic Gonadotropin): Complete Research Guide prefilled to estimate concentration, draw volume, and related measurement math from the reconstitution details you already have.