Gonadorelin: Complete Research Guide
On this page
Quick Reference Card
Attribute
Also Known As
- Detail
- GnRH, LHRH, Luteinizing Hormone-Releasing Hormone, Gonadoliberin, Gonadotropin-Releasing Hormone, LRF (Luteinizing Hormone-Releasing Factor)
Attribute
Administration
- Detail
- Injectable (subcutaneous, intravenous); pulsatile infusion pump for clinical use
Attribute
Research Status
- Detail
- FDA-approved for diagnostic testing of pituitary gonadotroph function and treatment of hypogonadotropic hypogonadism (brand names: Factrel, Lutrepulse). Also used in veterinary medicine (Cystorelin, Fertagyl).
Attribute
Typical Dose Range
- Detail
- 100-500 mcg per injection; frequency varies by protocol (see Dosing Protocols section)
Attribute
Half-Life
- Detail
- 2-40 minutes (plasma elimination); highly variable by measurement method
Attribute
Cycle Length
- Detail
- 4-8 weeks (subcutaneous protocols); variable for pulsatile pump therapy
Attribute
Storage
- Detail
- Lyophilized: -20°C for long-term, 2-8°C for short-term; Reconstituted: 2-8°C, use within 28 days
Overview / What Is Gonadorelin?
The Basics
Gonadorelin is a synthetic copy of a hormone your brain naturally produces called gonadotropin-releasing hormone (GnRH). Your hypothalamus, a small region at the base of your brain, releases this hormone in rhythmic pulses roughly every one to two hours. Each pulse tells the pituitary gland to release two other hormones: luteinizing hormone (LH) and follicle-stimulating hormone (FSH). Together, LH and FSH control testosterone production in men, estrogen and progesterone production in women, and fertility in both sexes.
Think of your hormonal system like a chain of command. Gonadorelin is the order from headquarters telling middle management (the pituitary) to send work instructions down to the production floor (the testes or ovaries). When that chain of command breaks down, whether from age, stress, certain medications, or medical conditions, hormone production drops. Gonadorelin attempts to restore the signal at the top of the chain rather than replacing the end product.
This distinction matters. Unlike testosterone replacement, which provides the final hormone directly but shuts down your body's own production system, gonadorelin works upstream to restart the natural cascade. That means it can preserve fertility and testicular function, which straight testosterone replacement cannot [1][2].
Gonadorelin has been used in medicine since the late 1970s. It received FDA approval for diagnostic testing of pituitary function and for treating a specific condition called hypogonadotropic hypogonadism, where the brain fails to send adequate signals to the pituitary [3]. More recently, it has gained attention in TRT (testosterone replacement therapy) clinics as a potential fertility-preserving adjunct, though this use remains controversial in the community due to challenges with its very short active life in the body.
The Science
Gonadorelin is a synthetic decapeptide structurally identical to endogenous gonadotropin-releasing hormone (GnRH), also known as luteinizing hormone-releasing hormone (LHRH). Its amino acid sequence (pGlu-His-Trp-Ser-Tyr-Gly-Leu-Arg-Pro-Gly-NH2) is highly conserved across mammalian species, underscoring its fundamental role in reproductive endocrinology [1][4].
The peptide binds to GnRH receptors (GnRHR) on gonadotroph cells of the anterior pituitary, activating a Gq/11-coupled signaling cascade that triggers phospholipase C (PLC) activation, inositol trisphosphate (IP3) generation, and intracellular calcium mobilization. This cascade stimulates both the immediate release of stored LH and FSH and the longer-term upregulation of gonadotropin gene transcription [1][4].
A critical pharmacological distinction separates pulsatile and continuous GnRH exposure. Physiological pulsatile delivery maintains and stimulates gonadotropin secretion, while sustained continuous exposure leads to GnRH receptor downregulation, desensitization of gonadotroph cells, and paradoxical suppression of LH and FSH. This biphasic response is the mechanistic basis for both the therapeutic use of pulsatile gonadorelin in hypogonadism and the deliberate suppressive use of long-acting GnRH agonists (leuprolide, goserelin) in conditions like prostate cancer and endometriosis [1][5][6].
FDA-approved indications include diagnostic evaluation of hypothalamic-pituitary-gonadal axis integrity (Factrel) and induction of ovulation/spermatogenesis via pulsatile subcutaneous delivery (Lutrepulse) in patients with hypothalamic GnRH deficiency [3].
Molecular Identity
Attribute
Common Names
- Detail
- Gonadorelin, GnRH, LHRH, Gonadoliberin, Luteinizing Hormone-Releasing Factor
Attribute
Amino Acid Sequence
- Detail
- pGlu-His-Trp-Ser-Tyr-Gly-Leu-Arg-Pro-Gly-NH2
Attribute
Sequence Length
- Detail
- 10 amino acids (decapeptide)
Attribute
Molecular Formula
- Detail
- C55H75N17O13
Attribute
Molecular Weight
- Detail
- 1182.31 g/mol (free peptide); 1218.76 g/mol (hydrochloride salt)
Attribute
CAS Number
- Detail
- 33515-09-2 (primary); 9034-40-6 (alternative); 52699-48-6 (acetate salt)
Attribute
PubChem CID
- Detail
- 638793
Attribute
UniProt
- Detail
- P01148 (human GnRH precursor); P09672 (GnRH receptor)
Attribute
FDA UNII
- Detail
- 9O7312W37G
Attribute
Structural Type
- Detail
- Linear peptide; N-terminal pyroglutamate ring; C-terminal glycine amide
Attribute
Salt Forms
- Detail
- Free peptide, acetate salt, hydrochloride salt, diacetate tetrahydrate
Attribute
Brand Names
- Detail
- Factrel (diagnostic), Lutrepulse (pulsatile pump), Cystorelin (veterinary), Fertagyl (veterinary)
The pyroglutamate modification at position 1 and C-terminal amidation are both essential for biological activity and receptor binding. The conserved N- and C-terminal residues across species highlight the evolutionary importance of this signaling peptide in reproductive biology [4].
Mechanism of Action
The Basics
Your brain releases gonadorelin (GnRH) in pulses, roughly every 60 to 120 minutes. Each pulse acts like a timed signal telling your pituitary gland to produce and release two key hormones: LH and FSH. LH travels to the testes (in men) to trigger testosterone production, while FSH supports sperm development. In women, these same hormones coordinate the menstrual cycle, egg maturation, and ovulation.
The timing of these pulses is everything. If gonadorelin arrives in short, rhythmic bursts, the pituitary responds by maintaining healthy hormone production. But if the signal becomes constant (no pulses, just a steady stream), something counterintuitive happens: the pituitary actually shuts down. The receptors become overwhelmed and stop responding. This is why long-acting GnRH drugs are used to deliberately suppress hormones in prostate cancer treatment, and it is also why getting the dosing frequency right with gonadorelin is so critical [5][6].
Synthetic gonadorelin is structurally identical to what your brain produces naturally. When injected, it mimics that natural pulse. The challenge is that it breaks down very quickly in the body, which means a single injection produces only a brief spike in LH and FSH before the signal disappears.
The Science
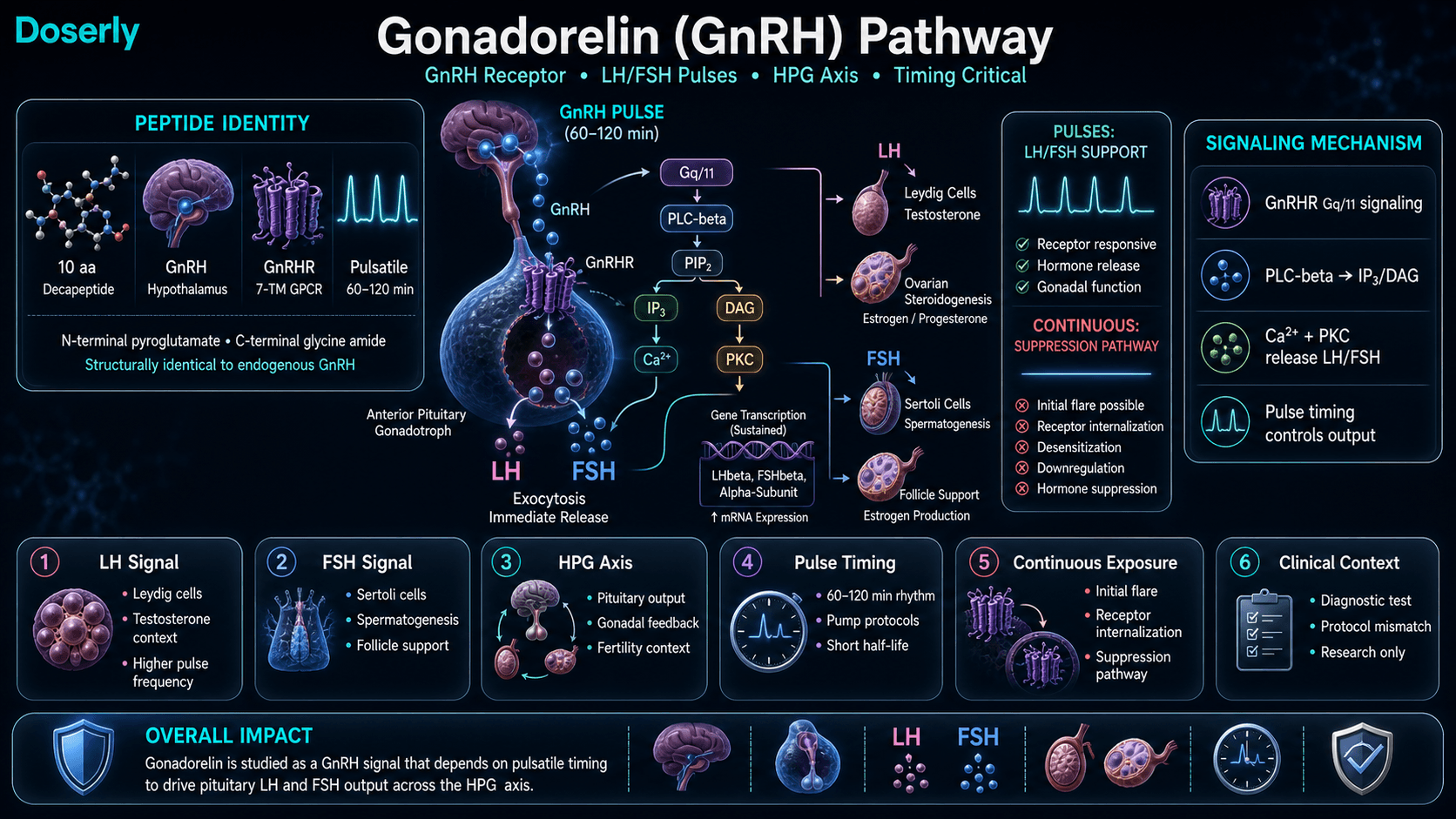
Gonadorelin activates the GnRH receptor (GnRHR), a seven-transmembrane G protein-coupled receptor expressed on anterior pituitary gonadotroph cells. Receptor binding triggers the Gq/11 signaling pathway: phospholipase C-beta (PLCbeta) hydrolyzes phosphatidylinositol 4,5-bisphosphate (PIP2) into IP3 and diacylglycerol (DAG). IP3-mediated calcium release from endoplasmic reticulum stores, combined with DAG-mediated protein kinase C (PKC) activation, drives both immediate exocytotic release of LH and FSH from secretory granules and transcriptional upregulation of gonadotropin subunit genes (LHbeta, FSHbeta, and common alpha-subunit) [1][4].
The frequency and amplitude of GnRH pulses differentially regulate LH and FSH secretion. Higher-frequency pulses (approximately every 60 minutes) favor LH secretion, while lower-frequency pulses (every 120-240 minutes) preferentially stimulate FSH [7]. This frequency-dependent modulation explains the physiological shift from FSH-dominant follicular phase signaling to LH-dominant luteal phase signaling during the menstrual cycle.
Continuous GnRH exposure produces an initial "flare" of gonadotropin release (2-4 days), followed by progressive receptor downregulation through internalization, reduced receptor recycling, and desensitization of post-receptor signaling. This mechanism underlies the therapeutic use of GnRH agonists (leuprolide, goserelin, triptorelin) for androgen/estrogen suppression in hormone-sensitive cancers, endometriosis, precocious puberty, and gender-affirming care [5][6].
Pathway Visualization Image
Pharmacokinetics
The Basics
Gonadorelin has one of the shortest active lives of any injectable peptide. After injection, it enters the bloodstream quickly but is broken down within minutes. Most sources describe a plasma half-life somewhere between 2 and 40 minutes, with the variation depending on how the measurement is done and whether you are looking at the peptide itself or its downstream effects.
What this means practically: a single injection produces a brief burst of LH and FSH release, but the effect fades quickly. This is why clinical protocols designed for ongoing therapy use either frequent injections throughout the day or specialized pump devices that deliver small doses every 90 to 120 minutes, mimicking the brain's natural pulsatile pattern.
For individuals using subcutaneous injections, the short active window creates a real challenge. Most TRT clinic protocols prescribing once or twice weekly injections are widely considered insufficient by both the clinical literature and the user community. The pharmacokinetics of this peptide demand more frequent administration than most other injectable compounds.
The Science
Following subcutaneous administration, gonadorelin demonstrates rapid absorption with peak plasma concentrations reached within minutes. The peptide undergoes rapid enzymatic hydrolysis in plasma, with a terminal elimination half-life reported between 2 and 40 minutes depending on the assay methodology and population studied [1][3].
The extremely rapid clearance is attributable to ubiquitous peptidase activity, particularly endopeptidases that cleave at the Gly6-Leu7 and Trp3-Ser4 bonds. Renal excretion of metabolites follows enzymatic degradation [3].
Bioavailability via subcutaneous injection is adequate for clinical use, though significantly lower than intravenous administration. No oral bioavailability exists due to gastrointestinal proteolysis and first-pass hepatic metabolism [3].
The pharmacokinetic profile necessitates pulsatile delivery for sustained therapeutic effect. The Lutrepulse pump, the FDA-approved delivery system, administers 5-20 mcg pulses intravenously or subcutaneously every 90 minutes, achieving physiological gonadotropin patterns [3]. Alternative protocols using 2-3 daily subcutaneous injections represent a practical compromise between clinical efficacy and patient compliance, though they deviate from true pulsatile physiology.
The half-life and clearance data above tells you how long the compound stays active, but what does that mean for your daily schedule? Doserly's pharmacokinetic tools let you plug in your dose and frequency to see a projected concentration timeline, helping you understand when you're at peak levels and when the compound has largely cleared.
This becomes especially useful when titrating. If you're increasing your dose gradually, the estimator shows how each step changes your projected peak and trough levels, giving you and your healthcare provider concrete data to discuss at check-ins rather than relying on subjective feel alone.
See where a dose, cycle, or change fits in time.
Doserly gives each protocol a timeline so dose changes, pauses, restarts, and observations are easier to compare later.
Timeline
Cycle history

Timeline tracking helps with recall; it is not a treatment recommendation.
Research & Clinical Evidence
Hypogonadotropic Hypogonadism and Fertility
The Basics
The strongest clinical evidence for gonadorelin is in treating hypogonadotropic hypogonadism, a condition where the brain fails to send proper signals to the pituitary gland, resulting in low testosterone, low sperm production, and impaired fertility. When gonadorelin is delivered in a pulsatile pattern (mimicking the brain's natural rhythm), it can restart the entire hormonal cascade and restore fertility.
In men with this condition, pulsatile gonadorelin therapy has demonstrated success rates of approximately 96% for restoring ovulation in women with hypothalamic amenorrhea, and it can induce spermatogenesis in men who were previously azoospermic (zero sperm count) [2][7]. A 2019 study found that pulsatile gonadorelin pump therapy induced earlier spermatogenesis compared to alternative treatments [8].
The Science
Pulsatile GnRH administration in men with congenital or acquired hypogonadotropic hypogonadism normalizes LH pulsatility, restores intratesticular testosterone levels, and initiates spermatogenesis. A 2015 study in males with isolated hypogonadotropic hypogonadism demonstrated that pulsatile gonadorelin therapy achieved normalization of gonadotropin levels and induction of spermatogenesis in the majority of subjects [8][9].
A 2019 study specifically examined the pulsatile gonadorelin pump in male patients and found that it induced earlier onset of spermatogenesis compared to combined gonadotropin therapy (HCG + FSH), suggesting potential advantages in the speed of fertility restoration [8].
In women with hypothalamic amenorrhea, pulsatile GnRH therapy has demonstrated ovulation induction rates exceeding 90% in properly selected patients, making it one of the most effective interventions for this specific subset of infertility [7][10].
Prostate Cancer
The Basics
Prostate cancer is highly sensitive to testosterone. Gonadorelin and its longer-acting relatives (leuprolide, goserelin) have been used since 1979 to suppress testosterone production in men with prostate cancer, a treatment sometimes called "medical castration." When GnRH agonists are administered continuously (rather than in pulses), they paradoxically shut down the very hormones they initially stimulate [5].
Combined androgen blockade (CAB), which pairs GnRH-based suppression with localized anti-androgen drugs, has become a cornerstone of prostate cancer treatment. Research suggests that when combined with early detection, CAB can achieve cure rates approaching 99% for prostate cancer [6][11].
The Science
Continuous GnRH agonist administration in prostate cancer exploits the receptor downregulation phenomenon. After an initial LH/testosterone flare lasting 2-4 days, sustained GnRH receptor stimulation leads to progressive receptor internalization and desensitization, achieving castrate levels of serum testosterone (below 50 ng/dL) within 2-4 weeks [5][6].
Labrie et al. demonstrated that intraprostatic androgen synthesis via intracrine mechanisms contributes to castration-resistant prostate cancer (CRPC), leading to the development of combined androgen blockade strategies that pair systemic GnRH suppression with local anti-androgen agents [6][11]. Two drugs approved by the FDA for CRPC emerged from this line of research.
Breast Cancer Prevention
The Basics
Research has explored gonadorelin's potential role in breast cancer prevention by suppressing ovarian estrogen production. Studies suggest that long-term GnRH treatment in postmenopausal women with excess androgen production can reduce estrogen levels and potentially lower breast cancer risk. One analysis estimated that 10 years of gonadorelin use could reduce breast cancer risk by approximately 50%, and 15 years could reduce it by roughly 70% [12][13].
The Science
Estrogen-receptor-positive breast cancers require estrogen for growth. GnRH agonist-mediated suppression of ovarian steroidogenesis represents a non-surgical alternative to oophorectomy for reducing estrogen exposure in high-risk populations [12][13].
Secreto et al. proposed that reducing excessive ovarian androgen production in postmenopausal women represents a targeted cancer prevention strategy, demonstrating that GnRH agonist treatment achieved sustained reduction of sex steroid levels without serious adverse effects [12]. Spicer and Pike estimated breast cancer risk reductions of 50% (10 years) and 70% (15 years) with GnRH agonist exposure, based on estrogen-exposure modeling [13].
Alzheimer's Disease Research
The Basics
Emerging research suggests connections between reproductive hormones and Alzheimer's disease. Elevated levels of LH after menopause have been correlated with increased Alzheimer's risk and decreased memory performance. Researchers are investigating whether modulating GnRH signaling could influence Alzheimer's pathology, though this work remains in its early stages [14][15].
The Science
Burnham et al. demonstrated that LH acts directly on hippocampal receptors to impair spatial memory in animal models [14]. Rao reported that elevated LH levels correlate with increased amyloid plaque deposition [15]. Genetic ablation of the LH receptor in Alzheimer's mouse models improved amyloid pathology [16].
Bowen et al. found that leuprolide (a GnRH agonist) was associated with decreased Alzheimer's risk compared to other androgen deprivation therapies, suggesting that the specific downstream effects of different GnRH modulators on LH suppression may have differential neuroprotective properties [17]. Caceres et al. identified epistatic interactions between APOE/MS4A6A genetic loci and GnRH signaling pathways in late-onset Alzheimer's, opening new avenues for understanding genotype-specific risk modulation [18].
Biomarker Evidence Matrix
The following matrix scores gonadorelin across relevant biomarker categories. Evidence Strength reflects the quality of research data (clinical trials, animal studies, mechanistic evidence). Reported Effectiveness reflects real-world community reports from the sentiment analysis.
Category
Libido
- Evidence Strength
- 6/10
- Reported Effectiveness
- 3/10
- Summary
- Clinical data supports restoration of libido through testosterone normalization in hypogonadal patients. Community reports are predominantly negative, but this reflects inadequate dosing protocols (1-3x/week) rather than the peptide's inherent capability.
Category
Sexual Function
- Evidence Strength
- 6/10
- Reported Effectiveness
- 3/10
- Summary
- Pulsatile therapy restores gonadal function in hypogonadotropic hypogonadism. Community experience is negative due to protocol mismatch with pharmacokinetics.
Category
Hormonal Symptoms
- Evidence Strength
- 7/10
- Reported Effectiveness
- 4/10
- Summary
- Well-documented ability to modulate LH, FSH, testosterone, and estrogen. Hot flashes and hormonal fluctuation symptoms are expected pharmacological effects during treatment.
Category
Nausea & GI Tolerance
- Evidence Strength
- 4/10
- Reported Effectiveness
- 3/10
- Summary
- Limited clinical documentation of GI effects. Community reports consistent GI distress (stomach cramps, gas, bowel disruption) in multiple independent reports.
Category
Side Effect Burden
- Evidence Strength
- 5/10
- Reported Effectiveness
- 3/10
- Summary
- Clinical trials report generally mild side effects (headache, flushing, injection site reactions). Community reports a worse profile, likely reflecting protocol-dependent issues.
Category
Treatment Adherence
- Evidence Strength
- 3/10
- Reported Effectiveness
- 2/10
- Summary
- The 2-40 minute half-life makes adherence to effective protocols extremely challenging without a pulsatile pump. Standard clinic injection protocols are widely considered insufficient.
Category
Muscle Growth
- Evidence Strength
- 4/10
- Reported Effectiveness
- 4/10
- Summary
- Indirect support through testosterone restoration. No direct muscle-building mechanism. Limited community data.
Category
Mood & Wellbeing
- Evidence Strength
- 5/10
- Reported Effectiveness
- 4/10
- Summary
- Testosterone normalization expected to improve mood. Community data is mixed and heavily confounded by TRT context.
Category
Energy Levels
- Evidence Strength
- 5/10
- Reported Effectiveness
- 4/10
- Summary
- Expected improvement through HPG axis restoration. Insufficient community data for confident scoring.
Category
Longevity & Neuroprotection
- Evidence Strength
- 5/10
- Reported Effectiveness
- N/A
- Summary
- Emerging Alzheimer's research shows promise but remains preclinical. No community data on neuroprotective outcomes.
Category
Immune Function
- Evidence Strength
- 3/10
- Reported Effectiveness
- N/A
- Summary
- Limited evidence from GnRH analog studies showing thymus modulation. No community data.
Category
Skin Health
- Evidence Strength
- 2/10
- Reported Effectiveness
- 3/10
- Summary
- No clinical evidence for skin effects. One community report of body acne on gonadorelin.
Categories not scored (insufficient data): Fat Loss, Weight Management, Appetite & Satiety, Food Noise, Sleep Quality, Focus & Mental Clarity, Memory & Cognition, Anxiety, Stress Tolerance, Motivation & Drive, Emotional Aliveness, Emotional Regulation, Joint Health, Inflammation, Pain Management, Recovery & Healing, Physical Performance, Gut Health, Digestive Comfort, Hair Health, Heart Health, Blood Pressure, Heart Rate & Palpitations, Temperature Regulation, Fluid Retention, Body Image, Bone Health, Cravings & Impulse Control, Social Connection, Withdrawal Symptoms, Daily Functioning
Benefits & Potential Effects
The Basics
Gonadorelin's primary value lies in restoring your body's own hormone production rather than replacing hormones from outside. When it works as intended (with proper pulsatile delivery), the benefits include:
Testosterone restoration. By restarting the LH signal, gonadorelin can help raise testosterone levels naturally. This is particularly relevant for men with hypogonadotropic hypogonadism where the problem originates in the brain's signaling, not in the testes themselves.
Fertility preservation. Unlike exogenous testosterone, which shuts down sperm production, gonadorelin stimulates both LH and FSH, maintaining the full hormonal cascade needed for spermatogenesis. This makes it valuable for men who want hormone optimization without sacrificing fertility [2][8].
Testicular function maintenance. Some practitioners prescribe gonadorelin alongside TRT to help prevent testicular atrophy, though community reports on this application are mixed and dependent on dosing frequency.
Diagnostic utility. A single gonadorelin injection and subsequent blood draw can reveal whether the pituitary gland is functioning normally, helping clinicians distinguish between hypothalamic and pituitary causes of hormone deficiency [3].
The Science
Demonstrated and investigated benefits of pulsatile gonadorelin administration include:
- Restoration of physiological gonadotropin pulsatility and normalization of LH/FSH levels in hypogonadotropic hypogonadism [1][2][9]
- Induction of spermatogenesis in previously azoospermic men with hypothalamic GnRH deficiency [8][9]
- Ovulation induction in women with hypothalamic amenorrhea, with success rates exceeding 90% [7][10]
- Diagnostic assessment of anterior pituitary gonadotroph reserve via the GnRH stimulation test [3]
- Preservation of intratesticular testosterone and Leydig cell function when used adjunctively with exogenous testosterone [2]
It is important to note that many of these benefits require pulsatile delivery at physiological frequency (every 60-120 minutes), which is not achievable with standard subcutaneous injection protocols used by most clinical settings.
Side Effects & Safety Considerations
The Basics
Gonadorelin is generally considered well-tolerated when used at appropriate doses and frequencies. The most commonly reported side effects include:
- Headache. Transient headaches are among the most frequently noted effects.
- Flushing and hot flashes. These reflect the hormonal modulation occurring at the pituitary level and are an expected pharmacological response.
- Injection site reactions. Mild redness, discomfort, or swelling at the injection location.
- GI distress. Multiple community reports describe stomach cramps, gas, and bowel disruption lasting 1-2 days following injection. While not prominently featured in clinical literature, this appears to be a recurring pattern in real-world use.
- Testicular discomfort. Some users report transient testicular pain, particularly at higher doses.
- Lightheadedness. Occasional reports of dizziness or lightheadedness post-injection.
- Skin changes. Isolated reports of body acne (abdomen, flanks, buttocks) during gonadorelin use.
The most serious risk with gonadorelin is paradoxical hormone suppression from improper dosing. Continuous or too-frequent administration can overwhelm pituitary GnRH receptors and cause them to downregulate, leading to decreased rather than increased LH and FSH production. This is the same mechanism used intentionally by long-acting GnRH agonists to suppress hormones in cancer treatment. Getting the dosing frequency right is essential to avoid this effect [5][6].
The Science
Adverse effects reported in clinical trials of pulsatile gonadorelin include injection site reactions (erythema, induration), headache, nausea, and abdominal discomfort. Ovarian hyperstimulation syndrome (OHSS) is a recognized risk in female patients undergoing ovulation induction, requiring monitoring of estradiol levels and ovarian size [3][10].
The receptor downregulation phenomenon following continuous or supraphysiological GnRH exposure is well-characterized. Initial administration triggers a gonadotropin "flare" lasting 2-4 days, followed by progressive desensitization of the GnRHR-Gq signaling cascade, internalization of receptors via beta-arrestin-mediated endocytosis, and reduced gonadotropin gene transcription [5]. This results in chemical castration levels of sex steroids, an effect that is reversible upon discontinuation.
Safety monitoring should include periodic assessment of LH, FSH, testosterone (men) or estradiol (women), and in fertility contexts, semen analysis or ovarian ultrasound [3].
Side effect profiles are most useful when you can compare them against your own experience in real time. Doserly lets you log symptoms, severity, and timing alongside your dosing data, creating a side-by-side view of your protocol and your body's response.
This kind of systematic tracking catches things that memory alone misses. A subtle mood shift that began three days after a dose increase. Sleep disruption that correlates with evening administration. These patterns become visible when the data is laid out on a timeline, and they give your healthcare provider actionable information rather than vague concerns. Early detection of emerging side effects means earlier intervention.
Keep side effects, flags, and follow-up notes visible.
Doserly helps you document safety observations, side effects, medication changes, and follow-up questions so important context is not scattered.
Safety log
Flags and notes

Safety notes are not emergency guidance; seek medical help when appropriate.
Dosing Protocols
The Basics
Dosing gonadorelin correctly is more important than with almost any other injectable peptide, and it is where most protocols go wrong. The peptide's extremely short active life (minutes, not hours) means that dosing frequency matters as much as dose size.
Commonly reported dose ranges include:
- Standard (starting): 100 mcg per injection
- Moderate: 250 mcg per injection
- Intensive: 500 mcg per injection
The critical variable is frequency. Three broad protocol approaches exist in the available sources:
- Pulsatile pump delivery (clinical gold standard). Small doses (5-20 mcg) delivered every 90 minutes via a subcutaneous or intravenous pump. This is the FDA-approved method and produces the most physiological results, but requires specialized equipment and is impractical for most users [3].
- Daily or every-other-day subcutaneous injections. The most commonly discussed community approach. Doses of 100-500 mcg administered daily or every other day represent a practical compromise. Results are less consistent than pulsatile delivery.
- Two to three times weekly subcutaneous injections. The most common clinic protocol, but widely criticized by both the community and clinical literature as pharmacologically insufficient given the peptide's rapid clearance.
The reconstitution approach most commonly described involves adding 2.0 mL of bacteriostatic water to a 2 mg vial, producing a concentration of 1 mg/mL (1000 mcg/mL). Morning administration is generally preferred. Cycle lengths of 4-8 weeks are commonly reported.
The Science
FDA-approved dosing for pulsatile gonadorelin (Lutrepulse) specifies 5 mcg per pulse delivered intravenously every 90 minutes for 21 days per cycle, with dose adjustments based on clinical response [3]. Subcutaneous pulsatile delivery has also been studied at 20 mcg per pulse with comparable efficacy [7].
For the GnRH stimulation test (diagnostic use), a single intravenous dose of 100 mcg is administered with serial LH and FSH measurements at baseline, 15, 30, 45, 60, and 120 minutes post-injection [3].
Non-pulsatile subcutaneous protocols lack standardized evidence-based dosing. The commonly cited range of 100-500 mcg per injection at frequencies from daily to three times weekly represents community-derived and clinic-derived protocols that have not been validated in controlled trials for efficacy in maintaining gonadotropin levels during exogenous testosterone use.
The dosing protocols above involve numbers that matter: specific microgram amounts, reconstitution ratios, and timing windows. Getting any of these wrong compounds across every subsequent dose from that vial.
Doserly's dose and reconstitution calculators eliminate the guesswork. Enter your vial size, peptide amount, and target dose, and get the exact bacteriostatic water volume, units per tick mark, and doses per vial. The injection site tracker maps your administration history as a visual heat map across your body, flagging areas that need rest and suggesting rotation patterns. Combined with dose reminders that include compound name, amount, and route, every aspect of your daily protocol is handled with the precision it requires.
Build reminders around the routine, not just the compound.
Doserly can keep timing, skipped doses, and schedule changes organized so the plan you read about becomes easier to follow and review.
Today view
Upcoming reminders

Reminder tracking supports consistency; it does not select a protocol for you.
What to Expect
Week 1-2: Most users report minimal noticeable effects during the first two weeks. Blood work may show early changes in LH and FSH levels, but subjective symptoms are unlikely to shift yet. Some users report mild side effects such as headache, flushing, or GI discomfort as the body adjusts. Testicular changes (if occurring) may begin to be noticed toward the end of this period.
Week 3-4: Users who are responding to the protocol may begin to notice changes in testicular fullness and, in some cases, modest improvements in energy and mood. Blood work at this stage provides the most useful feedback on whether the protocol is achieving its intended hormonal effects. Ejaculate volume changes have been reported by some users within this timeframe.
Week 5-8: If the protocol is effective, hormonal markers should show measurable improvement. Men using gonadorelin for fertility support may see early indicators of spermatogenesis. For those using it alongside TRT for testicular maintenance, this is typically the evaluation point where the protocol's success or failure becomes clear through blood work.
Important context: Community experience varies dramatically based on dosing frequency. Users on once or twice weekly protocols frequently report no noticeable effects at any timepoint. Users on daily or more frequent protocols report more consistent, though still modest, outcomes. The "timeline" for gonadorelin is less about patience and more about whether the dosing protocol matches the peptide's pharmacokinetics.
Interaction Compatibility
Good With (Synergistic or Complementary)
- HCG — HCG acts directly on Leydig cells (bypassing the pituitary), while gonadorelin acts at the pituitary level. Combined use addresses both arms of the HPG axis. One community report described achieving pregnancy from zero sperm count using gonadorelin + HCG together.
- Kisspeptin — Kisspeptin acts upstream of GnRH in the hypothalamic cascade. Some users and researchers suggest kisspeptin as an alternative or adjunct to gonadorelin, as it can stimulate endogenous GnRH release and may have additional benefits including DHEA/aldosterone production and libido enhancement.
- Enclomiphene — While not a peptide, enclomiphene (a selective estrogen receptor modulator) is frequently discussed alongside gonadorelin as an alternative for LH stimulation with potentially better compliance due to oral administration.
Use With Caution
- Exogenous Testosterone — While gonadorelin is sometimes prescribed alongside TRT, exogenous testosterone suppresses the HPG axis via negative feedback at the hypothalamus and pituitary. This reduces the pituitary's responsiveness to GnRH, potentially limiting gonadorelin's effectiveness. Estradiol from testosterone aromatization further suppresses GnRH receptor sensitivity [1][5].
- Aromatase Inhibitors — Sometimes co-prescribed during TRT to manage estrogen levels. May theoretically improve gonadorelin's pituitary-stimulating effects by reducing estradiol-mediated negative feedback, but clinical data supporting this combination is limited.
Not Good With
- Long-acting GnRH Agonists (leuprolide, goserelin, triptorelin) — These work by overwhelming and desensitizing GnRH receptors. Combining them with gonadorelin would be pharmacologically contradictory.
- GnRH Antagonists (cetrorelix, degarelix, ganirelix) — These directly block GnRH receptors, completely negating gonadorelin's mechanism of action.
Administration Guide
Materials required:
- Bacteriostatic water (BAC water) for reconstitution
- Insulin syringes (0.5-1 mL, 29-31 gauge)
- Alcohol swabs (70% isopropyl)
- Sharps disposal container
Recommended reconstitution solution: Bacteriostatic water (0.9% benzyl alcohol preserved) is the standard reconstitution solution for gonadorelin. The most commonly described approach is 2.0 mL of BAC water into a 2 mg vial, yielding 1 mg/mL (1000 mcg/mL).
Timing considerations: Morning administration is generally preferred. Gonadorelin should be injected on non-consecutive days at minimum (Mon/Wed/Fri is a commonly cited schedule), though daily or more frequent administration produces better results based on the peptide's short active life. Administration on an empty stomach is not required, unlike many other peptides.
Post-administration care: Monitor for common immediate reactions including mild flushing, headache, or injection site discomfort. GI symptoms (stomach cramps, gas) have been reported to appear within hours of injection and may persist for 1-2 days. If symptoms of hormonal suppression appear (testicular shrinkage, decreased libido, fatigue), this may indicate receptor desensitization from dosing that is too frequent or doses that are too large, and the protocol should be reviewed with a healthcare provider.
Supplies & Planning
Common vial sizes: 2 mg is the most widely available vial size for research-grade gonadorelin.
General supplies:
- Bacteriostatic water (0.9% benzyl alcohol) for reconstitution
- Insulin syringes: 29-31 gauge, 0.5 mL or 1 mL capacity
- Alcohol swabs (70% isopropyl alcohol)
- Sharps disposal container
- Optional: temperature-controlled storage bag for transport
Reconstitution solution volume: Varies by desired concentration. The reconstitution calculator can determine exact volumes based on the vial size, peptide amount, and target dose per injection.
Storage containers: Reconstituted vials should be stored upright in a refrigerator. Protect from light by wrapping in foil or storing in an opaque container.
Consult with a healthcare provider for guidance on specific quantities and protocol duration.
Storage & Handling
Lyophilized (powder) form:
- Optimal long-term storage: -20°C (-4°F) or below for up to 2-3 years
- Short-term storage: 2-8°C (35.6-46.4°F) for weeks to months
- Room temperature is acceptable for brief periods (days) during shipping, but is not recommended for extended storage
- Keep in sealed packaging with desiccant to minimize moisture exposure
- Store in a dry, dark environment
Reconstituted (liquid) form:
- Refrigerate at 2-8°C (35.6-46.4°F) immediately after reconstitution
- Use within 28 days when reconstituted with bacteriostatic water
- Do not freeze reconstituted solutions
- Avoid freeze-thaw cycles, which cause irreversible degradation
- Inspect for clarity before each use; solution should be colorless and clear with no particles or cloudiness
Handling best practices:
- Allow lyophilized vials to reach room temperature (10-30 minutes) before opening to prevent condensation
- Wrap vials in foil to protect from UV light
- Swab stopper with alcohol before each use
- Use sterile needles and syringes for every draw
- Label vials with reconstitution date
Lifestyle Factors
Supporting gonadorelin's mechanism of action through lifestyle optimization can improve outcomes:
Nutrition. A nutrient-dense, balanced diet rich in healthy fats and zinc supports endogenous hormone production and the restoration of the hypothalamic-pituitary-gonadal axis. Zinc is a cofactor in testosterone synthesis, and deficiency can impair HPG axis function independently of gonadorelin use.
Exercise. Regular physical activity, particularly resistance training, supports healthy testosterone levels and metabolic function during bioregulation protocols. Overtraining, however, can suppress GnRH pulsatility through stress-mediated hypothalamic dysfunction.
Sleep. Ensuring 7-9 hours of quality sleep is critical for optimal endocrine function. The majority of testosterone production occurs during sleep, and sleep deprivation independently suppresses gonadotropin release.
Stress management. High cortisol levels directly inhibit pulsatile GnRH release from the hypothalamus. Chronic stress can counteract the peptide's goal of restoring hormonal homeostasis. Meditation, breathwork, and consistent stress reduction practices support protocol effectiveness.
Regulatory Status & Research Classification
United States (FDA):
Gonadorelin is FDA-approved for two indications: (1) diagnostic evaluation of pituitary gonadotroph function (brand name: Factrel, approved by Ayerst Laboratories) and (2) induction of ovulation in women with hypothalamic amenorrhea via pulsatile delivery (brand name: Lutrepulse). It is also widely used in veterinary medicine for ovulation induction (brand names: Cystorelin, Fertagyl). Off-label use as an adjunct to TRT for fertility preservation is common in clinical practice but is not an FDA-approved indication.
WADA Status:
Gonadorelin and GnRH analogs are included on the WADA Prohibited List under Section S2 (Peptide Hormones, Growth Factors, Related Substances, and Mimetics). Athletes subject to anti-doping testing should be aware that use of gonadorelin may result in an adverse analytical finding.
Other Jurisdictions:
GnRH analogs are available by prescription in most developed countries, though specific brand availability and approved indications vary. Long-acting GnRH agonists (leuprolide, goserelin, triptorelin) are more widely prescribed than native gonadorelin due to practical advantages in most clinical settings.
Active Clinical Research:
Clinical research on pulsatile gonadorelin continues primarily in the fields of reproductive endocrinology and fertility. A 2021 systematic review and meta-analysis confirmed the safety and efficacy of GnRH analog treatment across multiple indications [19]. Ongoing research explores potential applications in Alzheimer's disease prevention and novel delivery mechanisms.
Regulatory status changes frequently. Always verify the current legal status of any compound in your specific country or jurisdiction before making any decisions.
FAQ
What is gonadorelin used for?
Gonadorelin is a synthetic version of gonadotropin-releasing hormone (GnRH), the hormone your brain uses to signal the pituitary gland to produce LH and FSH. It is FDA-approved for diagnosing pituitary function and for treating certain types of infertility. It is also used off-label by some clinics alongside testosterone replacement therapy to help maintain fertility and testicular function.
How is gonadorelin different from HCG?
Both support reproductive hormone function, but they work at different levels. HCG mimics LH and acts directly on the testes, bypassing the brain and pituitary entirely. Gonadorelin works at the pituitary level, stimulating the brain's own LH and FSH production. This difference means HCG produces more predictable and immediate results, while gonadorelin attempts to restore the natural signaling pathway. Community experience consistently reports HCG as more effective for most TRT-adjunct applications.
Why do some people say gonadorelin does not work?
Based on available community data, the most common reason for negative experiences is dosing frequency. Gonadorelin has a very short active life in the body (minutes, not hours). Most clinic protocols prescribe it once or twice weekly, which clinical literature and community experience both suggest is insufficient. Effective clinical use typically requires either a pulsatile pump delivering doses every 90 minutes or, at minimum, daily injections. Individuals considering gonadorelin should discuss appropriate dosing frequency with a knowledgeable healthcare provider.
Can gonadorelin be used for fertility while on TRT?
Some practitioners prescribe gonadorelin alongside TRT to help maintain FSH and LH stimulation and preserve spermatogenesis. However, exogenous testosterone suppresses the HPG axis through negative feedback, which may reduce the pituitary's responsiveness to GnRH. Community reports on this application are mixed. Some individuals have reported fertility success using gonadorelin in combination with HCG during TRT, though the relative contribution of each compound is difficult to isolate.
What are the common side effects of gonadorelin?
Commonly reported side effects based on available sources include headache, flushing, hot flashes, injection site discomfort, and gastrointestinal symptoms (stomach cramps, gas, bowel changes). The most significant safety consideration is the risk of paradoxical hormone suppression if dosing is too frequent or doses are too large, which overwhelms pituitary GnRH receptors and causes them to shut down rather than activate.
Is gonadorelin FDA-approved?
Yes. Gonadorelin is FDA-approved under the brand names Factrel (for diagnostic pituitary function testing) and Lutrepulse (for pulsatile ovulation induction in hypothalamic amenorrhea). Its use as a TRT adjunct for fertility preservation is off-label.
Sources & References
[1] Gonadorelin Peptide: Studies in Gonadotropin Release and Synthesis. Core Peptides Research Summary. Available at: https://www.corepeptides.com/gonadorelin-peptide-studies-in-gondotropin-release-and-synthesis/
[2] Kumar P, Sharma A. "Gonadotropin-releasing hormone analogs: Understanding advantages and limitations." J Hum Reprod Sci. 2014;7(3):170-174. doi:10.4103/0974-1208.142476
[3] Factrel (gonadorelin) prescribing information. U.S. Food and Drug Administration.
[4] UniProt: P01148 (human GnRH precursor protein); P09672 (GnRH receptor).
[5] Labrie F. "Hormonal therapy of prostate cancer." Prog Brain Res. 2010;182:321-341.
[6] Labrie F. "GnRH agonists and the rapidly increasing use of combined androgen blockade in prostate cancer." Endocr Relat Cancer. 2014;21(4):R301-317.
[7] Clinical applications of gonadotropin-releasing hormone agonists in gynaecological conditions. ScienceDirect. 2023. Available at: https://www.sciencedirect.com/science/article/pii/S2666334123000089
[8] "The Pulsatile Gonadorelin Pump Induces Earlier Spermatogenesis in Men." PMC. 2019. Available at: https://pmc.ncbi.nlm.nih.gov/articles/PMC6775549/
[9] "Pulsatile Gonadorelin therapy in males with isolated hypogonadotropic hypogonadism." PubMed. 2015. Available at: https://pubmed.ncbi.nlm.nih.gov/25603310/
[10] "Gonadorelin as a diagnostic tool for hypothalamic-pituitary-gonadal axis." PubMed. 2017. Available at: https://pubmed.ncbi.nlm.nih.gov/28330982/
[11] Labrie F. "Combined blockade of testicular and locally made androgens in prostate cancer: a highly significant medical progress based upon intracrinology." J Steroid Biochem Mol Biol. 2015;145:144-156.
[12] Secreto G, et al. "A novel approach to breast cancer prevention: reducing excessive ovarian androgen production in elderly women." Breast Cancer Res Treat. 2016;158(3):553-561.
[13] Spicer DV, Pike MC. "Sex steroids and breast cancer prevention." J Natl Cancer Inst Monogr. 1994;(16):139-147.
[14] Burnham V, Sundby C, Laman-Maharg A, Thornton J. "Luteinizing hormone acts at the hippocampus to dampen spatial memory." Horm Behav. 2017;89:55-63.
[15] Rao CV. "Involvement of Luteinizing Hormone in Alzheimer Disease Development in Elderly Women." Reprod Sci. 2017;24(3):355-368.
[16] Lin J, et al. "Genetic ablation of luteinizing hormone receptor improves the amyloid pathology in a mouse model of Alzheimer disease." J Neuropathol Exp Neurol. 2010;69(3):253-261.
[17] Bowen RL, Butler T, Atwood CS. "Not All Androgen Deprivation Therapies Are Created Equal: Leuprolide and the Decreased Risk of Developing Alzheimer's." J Clin Oncol. 2016;34(23):2800.
[18] Caceres A, Vargas JE, Gonzalez JR. "APOE and MS4A6A interact with GnRH signaling in Alzheimer's disease: Enrichment of epistatic effects." Alzheimers Dement. 2017;13(4):493-497.
[19] "Safety and efficacy of GnRH analog treatment: A systematic review and meta-analysis." PMC. 2021. Available at: https://pmc.ncbi.nlm.nih.gov/articles/PMC8248422/
[20] "Long-term outcomes of GnRH agonist treatment in girls with central precocious puberty." PMC. 2025. Available at: https://pmc.ncbi.nlm.nih.gov/articles/PMC11917394/
[21] Torrini F, Scarano S, Palladino P, Minunni M. "Advances and perspectives in the analytical technology for small peptide hormones analysis: A glimpse to gonadorelin." 2023.
[22] Schwentner C, et al. "Neoadjuvant gonadotropin-releasing hormone therapy before surgery may improve the fertility index in undescended testes: a prospective randomized trial." J Urol. 2005;173(3):974-977.
[23] Secreto G, et al. "Medical ovariectomy in menopausal breast cancer patients with high testosterone levels." Endocr Relat Cancer. 2017;24(11):C21-C29.
[24] Vollaard ES, et al. "Gonadotropin-releasing hormone agonist treatment in postmenopausal women with hyperandrogenism of ovarian origin." J Clin Endocrinol Metab. 2011;96(5):1197-1201.
[25] Labrie F. "Key role of endocrinology in the victory against prostate cancer." Bull Cancer (Paris). 2006;93(9):949-958.
[26] Smith MA, et al. "Putative Gonadotropin-Releasing Hormone Agonist Therapy and Dementia." J Alzheimers Dis. 2018;63(4):1269-1277.
Related Peptide Guides
- HCG — Direct LH analog; most common comparator to gonadorelin for testicular function support during TRT
- Kisspeptin — Upstream HPG axis stimulator; emerging alternative to gonadorelin
- Sermorelin — GHRH analog (different axis, but frequently discussed alongside gonadorelin in clinical peptide contexts)
- Ipamorelin — Growth hormone secretagogue (different axis but commonly co-prescribed in peptide protocols)
- PT-141 — Melanocortin receptor agonist for sexual dysfunction (complementary for sexual health goals)
- Oxytocin — Reproductive hormone with complementary reproductive health applications
- Melanotan II — Melanocortin receptor agonist with sexual function effects
Need the reconstitution math for Gonadorelin: Complete Research Guide?
Open the calculator with Gonadorelin: Complete Research Guide prefilled to estimate concentration, draw volume, and related measurement math from the reconstitution details you already have.